Shock KVB What is shock Shock is the

Shock KVB

What is shock? Shock is the clinical syndrome that results from inadequate tissue perfusion
, due to")
Classification of shock § Cardiogenic, due to heart failure § Hypovolemic (oligemic), due to fluid or blood loss § Distributive (hypotensive) owing to peripheral vasodilation

Types of Shock • • • Hypovolemic Cardiogenic Neurogenic Anaphylactic Septic

Types of Shock • • • Hypovolemic Cardiogenic Neurogenic Anaphylactic Septic Distributive shock

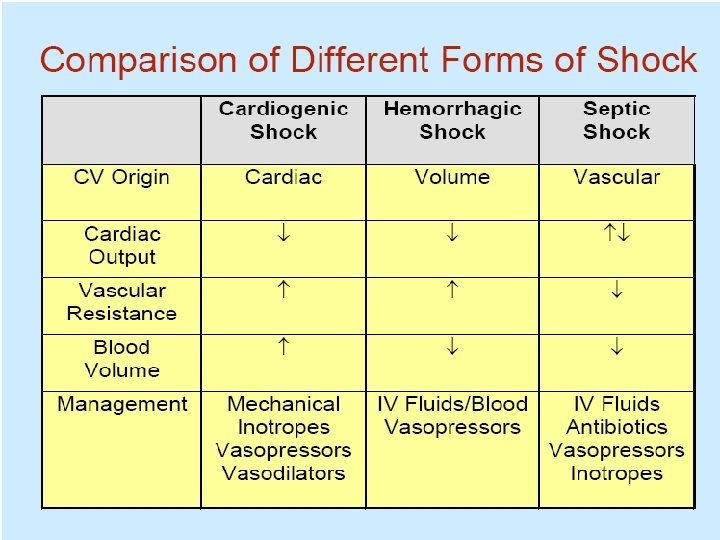
Common types of shock: – Cardiogenic shock – Hypovolemic shock – Septic shock

Less common types of shock • Neurogenic shock • Anaphylactic shock • Hypoadrenal shock

Common factor • Circulatory collapse resulting from a disproportion between circulating blood volume & the vascular space that it has to fill. • The ensuing tissue hypoxia or anoxia leads to multiple organ failure.

What happens with the perfusion deficit? 1. Insufficient delivery of oxygen & nutrients to cells and tissues. 2. Inadequate clearance of metabolites.

Outcomes of cellular hypoxia 1. Shift from aerobic to anaerobic metabolism. 2. This results in increased lactate production and later on, lactic acidosis.

• The metabolic & hemodynamic derangements are correctible at the outset & are associated with reversible cell injury. • Persistence or worsening of the shock state leads to irreversible injury and death of cells and possibly , death of the patient.

Cellular Response to Shock O 2 use Anaerobic metabolism ATP synthesis Na+ Pump Function Tissue perfusion Stimulation of clotting cascade & inflammatory response Intracellular Na+ & water Impaired cellular metabolism Impaired glucose usage Cellular edema Vascular volume

Hypovolemic Shock • Decreased intravascular volume • Causes: – Diarrhoea – Prolonged & excessive vomiting – Massive haemorrhage – Burns

Hypovolemic Shock • Hemorrhage – external – internal • GI tract • hemothorax • peritoneal or retroperitoneal space • Loss of fluid into third space – burns – pancreatitis

Causes of cardiogenic shock 1. Pump failure: Ø Ejection fraction < 20% Ø Associated with myocardial infarction Ø Associated with Conduction disturbances ( heart block or arrhythmias) 2. Obstructive heart failure Ø Caused by massive pulmonary emboli or valvular disease (Aortic stenosis)

Cardiogenic Shock • Myocardial pump failure – myocardial infarction – myocardial rupture – cardiac arrhythmia • Extrinsic compression – cardiac tamponade • Outflow obstruction – pulmonary embolus

Cardiogenic Shock R. A. S. Activation Volume/ Preload Impaired myocardial function Catecholamine Release CO Myocardial O 2 demand Dyspnea SVR O 2 supply Peripheral & pulmonary edema

Neurogenic Shock Sympathetic Tone Or Parasympathetic Tone Tissue perfusion Cardiac Output Vascular Tone Massive Vasodilation SVR & Preload

Anaphylactic Shock • Massive & systemic allergic reaction • Large release of histamine • Increases membrane permeability & vasodilation

Anaphylactic Shock Caused by a hypersensitivity reaction to an allergen in a previously sensitised patient

Common allergens:

Common Features • • Angio-oedema Bronchoconstriction Vasodilatation and hypotension Urticareal rash

Angio-oedema Normal Oedematous glottis

Septic Shock • “Circulatory failure” • Due to systemic infection

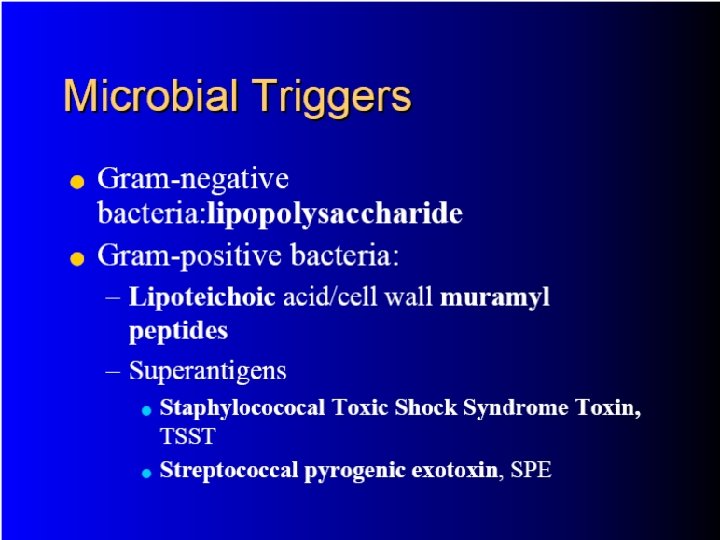
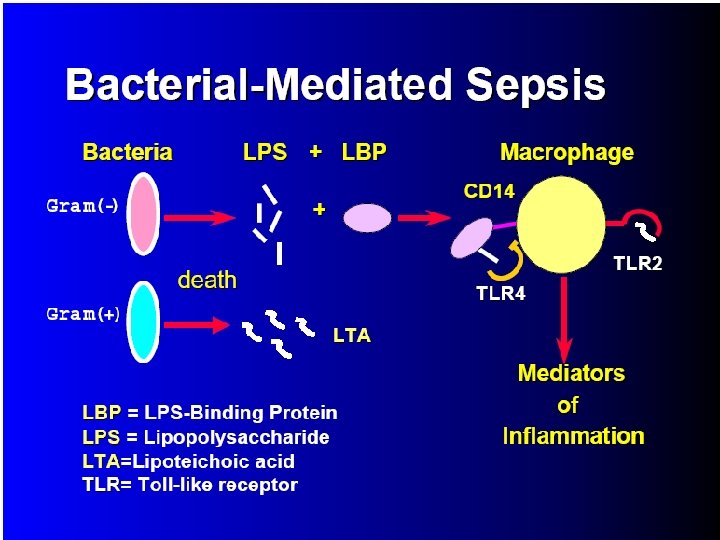
Septic Shock • Leading cause of death in intensive care units • Most cases (70%) are caused by gram negative bacteria (LPS-lipopolysaccharide) • Also can occur with gram positive bacteria and fungal organisms
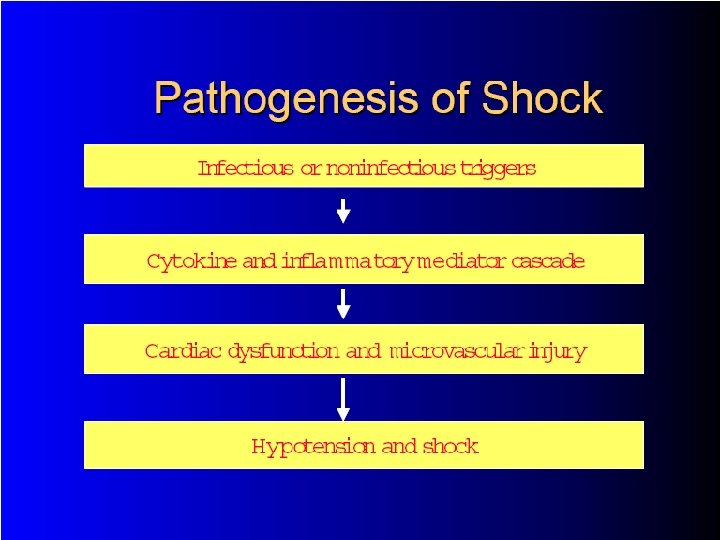
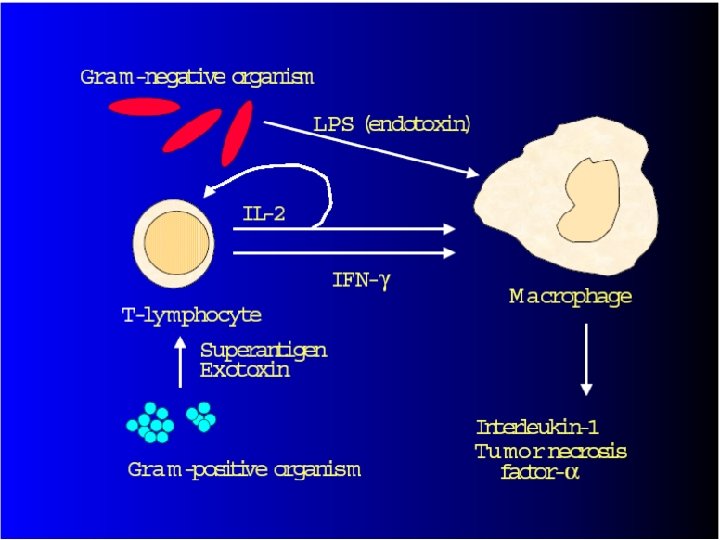

Effects of cytokine release
 And Secondarily Induced Effector Molecules")
Effects Of Lipopolysaccharide (LPS) And Secondarily Induced Effector Molecules

MODS= Multiple organ dysfunction syndrome

Multiple Organ Dysfunction System • Progressive dysfunction of two or more organ systems • Caused by uncontrolled inflammatory response to injury or illness – Typically sepsis

Stages of Shock • Compensated • Uncompensated • Irreversible
 Nonprogressive stage (compensatory) Progressive")
STAGES OF SHOCK • • Initial stage (early compensation stage) Nonprogressive stage (compensatory) Progressive stage (intermediate) Refractory stage (irreversible)

Homeostatic Mechanisms in Shock • Baroreceptor reflexes and catecholamine release – maintain cerebral and cardiac perfusion – decrease perfusion to gut, skin and kidneys • Activation of renin-angiotensin system – angiotensin II constricts efferent arteriole of glomerulus to maintain GFR – aldosterone promotes sodium retention • Release of Arginine Vasopressin (ADH) – promotes renal conservation of water
![Renin-Angiotensin-Aldosterone Plasma volume &/Or [Na+] Detected by Via ACE (Angiotensin Converting Enzyme) Kidney (juxtaglomerular](http://slidetodoc.com/presentation_image/db833470ba72f69b785d2781cd2a570b/image-38.jpg "Renin-Angiotensin-Aldosterone Plasma volume &/Or [Na+] Detected by Via ACE (Angiotensin Converting Enzyme) Kidney (juxtaglomerular")
Renin-Angiotensin-Aldosterone Plasma volume &/Or [Na+] Detected by Via ACE (Angiotensin Converting Enzyme) Kidney (juxtaglomerular apparatus) Releases Renin Converts Angiotensin II… Angiotensinogen


Uncompenstated Shock • Defense mechanisms begin to fail • Presentation – Hypotension – Marked increase in heart rate – Rapid, thready pulse – Agitation, restlessness, confusion

Irreversible Shock • Complete failure of compensatory mechanisms • Death even in presence of resuscitation

Symptoms of Shock General Symptoms • Anxiety /Nervousness • Dizziness • Weakness • Nausea & Vomiting • Thirst • Confusion • Decreased Urine Output Specific Symptoms • History of Trauma / other illness • Vomiting & Diarrhoea • Chest Pain • Fevers / Rigors • Shortness of breath (stridor)

Signs of Shock • • • Pallor Cold and clammy extremities Sweating Cyanosis Tachypnoea Tachycardia Confusion & agitation Stridor Hypotension Loss of consciousness

Features of compensated shock • Tachycardia • Skin pallor due to constriction of arterioles • Reduced urine production

Features of decompenstaed but still reversible shock • Hypotension • Dyspnoea & tachypnoea • Pulmonary oedema slowly develops, further worsening hypoxia • Oliguria (urine volume<500 ml/24 hr) • Acidosis due to anaerobic glycolysis
 • Respiratory")
Features of irreversible shock • Marked hypotension with extreme tachycardia (filiform pulse) • Respiratory distress which is not responsive to oxygen therapy & assisted ventilation • Loss of consciousness progressing to coma • Gastrointestinal bleeding • Anuria with elevated BUN & creatinine • Severe acidosis • Laboratory & clinical signs of DIC

Clinical Course • Hypovolemic shock – If patient is young and healthy, most survive if resuscitation restores perfusion • Cardiogenic shock and septic shock – Up to 75% mortality even with best care • Patients succumb with multi-organ failure – Tubular necrosis of kidneys – Ischemic enteropathy – Disseminated intravascular coagulation – Acute respiratory distress syndrome (septic shock)

Morphology of Shock Hypoxic injury to multiple organs • Kidneys – medulla and tubules most affected – acute tubular necrosis • Gastrointestinal tract – mucosa most sensitive to hypoxia • Brain • Heart – subendocardial necrosis of myocardium • Lungs – resistant to hypoxia but involved with septic shock

Kidney in shock: Coagulation necrosis of tubules

Renal Biopsy in DIC Capillary loops of glomeruli occluded by fibrin thrombi. H&E stain on left and MSB (Martius scarlet blue) for fibrin on the right
")
Myocardial necrosis(coagulation necrosis)
 Synonyms: – Shock lung – Diffuse alveolar damage – Acute")
Adult respiratory syndrome (ARDS) Synonyms: – Shock lung – Diffuse alveolar damage – Acute alveolar injury – Traumatic wet lungs These are descriptive terms for a syndrome caused by diffuse alveolar capillary damage.

Clinically characterized by: • Rapid onset of severe life-threatening respiratory insufficiency • Cyanosis • Severe arterial hypoxemia that is refractory to oxygen therapy • Frequently progresses to extrapulmonary multisystem organ failure.

Some causes of ARDS: • • Shock Sepsis Extensive surface burns Massive fractures & other trauma

Morphology: • In the acute edematous stage, the lungs are heavy, firm & boggy due to congestion, edema & inflammation.

Markedly congested & heavy lung

Microscopy • Alveoli are lined by waxy hyaline membranes.

This is followed by: • Proliferation of type II pneumocytes. • However resolution does not usually occur. • More commonly, there is organization of the fibrin exudate, with resultant intra-alveolar fibrosis. • There is marked thickening of the alveolar septae.
.")
• Mortality rate of ARDS is high (60%).

Approach to study: 1. 2. 3. 4. Definition of shock Classification of shock Causes of shock Pathogenesis of cardiac, neurogenic, septic & anaphylactic shock 5. Stages of shock including compensatory mechanisms 6. Clinical features of shock (at each stage) 7. Morphology of various organs & tissues in shock


Thank you
- Slides: 65