Sepsis3 new definitions of sepsis and septic shock







 • Systemic inflammatory response •")
 of admissions to ICU")
 of admissions to")
 of admissions")

















- Slides: 31
Sepsis-3 new definitions of sepsis and septic shock
Outline • A brief overview of sepsis • Introduction to the new Sepsis-3 definitions of sepsis and septic shock* • Interactive bit – design a new sepsis care bundle for your hospital JAMA 2016: 315 (8): 801 -810 February 23
Summary of Sepsis-3
What is ‘sepsis’? Life-threatening organ dysfunction caused by a dysregulated host response to infection
Sepsis The result of the body’s over-response to infection Pathogen Infection Host response ++ Inflammation Loss of homeostasis Organ dysfunction Death Other factors Coagulation / fibrinolysis Endothelial dysfunction
Inflammatory response to infection Pathogen Infection Anti-inflammatory mediators IL-4, IL-10, IL-11, IL-13, IL-1 r Monocyte/ macrophage Pro-inflammatory cytokines Tumor necrosis factor, IL-1, IL-6, IL-8 Neutrophil activation, aggregation, degranulation; release of oxygen free radicals and proteases Platelet activation – aggregation Endothelial damage T-cell IL-2, Interferon- , GM-CSF
Coagulation factors and platelets are consumed faster than they can be replaced.
Therefore: ‘classical’ features of sepsis (classical means advanced stages) • Systemic inflammatory response • Reduced systemic vascular resistance / vasodilatation • Increased capillary permeability • Coagulopathy and microvascular thrombosis • Metabolic (lactic) acidosis • Organ dysfunction
Prevalence and hospital mortality associated with severe sepsis Proportion (%) of admissions to ICU with severe sepsis in the first 24 hours Hospital mortality (%) 70 60 40 30 20 10 15 4 – 1 20 9 – 2 25 4 – 2 30 9 – 3 35 4 – 3 40 9 – 4 45 4 – 4 50 9 – 5 55 4 – 5 60 9 – 6 65 4 – 6 70 9 – 7 75 4 – 7 80 9 – 8 85 4 – 8 9 90 + – 1 9 10 5– 4 0 0– % 50 Age group (years)
The prognostic effect of organ dysfunction in severe sepsis Proportion (%) of admissions to ICU with severe sepsis in the first 24 hours in ICU with (N) organ dysfunctions Hospital mortality (%) 100 80 % 60 40 20 0 1 2 3 4 Number of organ dysfunctions 5
Hospital mortality associated with severe sepsis by APACHE II score Proportion (%) of admissions to ICU with severe sepsis in the first 24 hours in ICU by APACHE II score Hospital mortality (%) 100 % 80 60 40 20 0 0– 4 5– 9 10– 14 15– 19 20– 24 25– 29 30– 34 APACHE II score groups 35– 39 40– 44 45+
Pathogens involved in severe sepsis Gram negative Gram positive Fungal infection 20% 45% Mixed bacterial 19% 3% 10% 3% Other mixed Unconfirmed • Only 60% of severe sepsis/septic shock cases are associated with confirmed infection • Disease progression is similar regardless of causative organism
Video of the microcirculation in sepsis
SIRS is dead – long live q. SOFA! • Respiratory rate > 22/minute • Altered mentation • Systolic blood pressure <100 mm. Hg • Outside ICU this predicts those with a higher mortality
Date of download: 5/9/2016 Copyright © 2016 American Medical Association. All rights reserved.
Date of download: 5/9/2016 Copyright © 2016 American Medical Association. All rights reserved.
How does this relate to NEWS?
Any questions at this point?
What is the Sepsis Six? Despite new research, there is still evidence that care bundles are effective in sepsis.
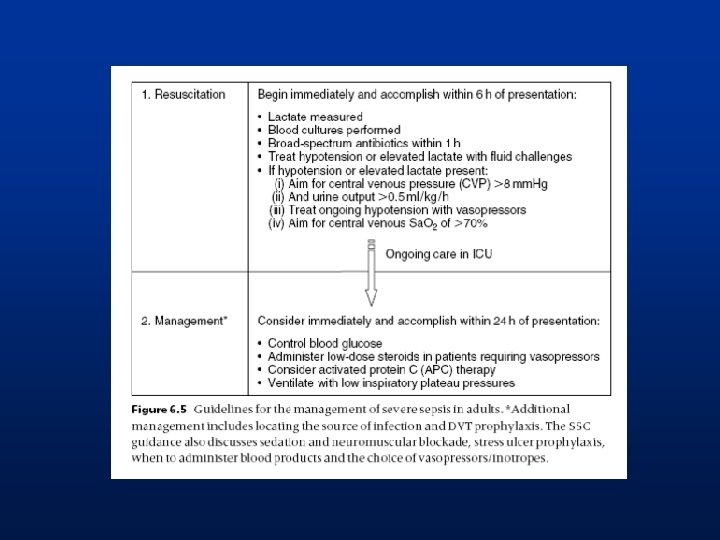
Sepsis Six – within the first hour survivingsepsis. org/guidel ines sepsistrust. org/clinicaltoolkit/ 1. Oxygen to achieve target sats 2. IV access and blood cultures 3. ABG/VBG to measure lactate 4. Fluid challenges to treat high lactate or low BP 5. IV antibiotics within 1 hour 6. Monitor urine output (catheter/fluid balance)
Early antibiotics matter – or do they?
What happens AFTER you’ve done the Sepsis Six?
Within the first 6 hours • If a patient does not respond to initial oxygen, iv fluid challenges and antibiotics … • Early senior decision making – For escalation? – Ceilings of care decisions • Move to a critical care area – Organ support (e. g. ventilation, vasopressors) and monitoring
Escalate early if patients do not respond to initial treatment! • Most patients who present with severe sepsis respond to oxygen, fluid challenges and iv antibiotics • ALL patients should be seen early by a senior Dr to decide whether ceilings of care apply
‘The greatest opportunity to improve outcomes for patients over the next quarter century will probably not come from discovering new treatments but from learning how to deliver existing effective therapies. ’ Lancet series on acute care 2005; 363: 1061 -67.
Any questions at this point?
Summary Severe sepsis has a high mortality Simple interventions outside the ICU improve outcome The SSC aims to reduce mortality from severe sepsis through education and the implementation of evidence based guidelines
In small groups – design a quick reference guideline for sepsis for your hospital