RADIODIAGNOSIS AND NUCLEARTHERAPY FOR THYROID DISEASE Hesti Gunarti



 � � Gray scale, color Doppler Transducer : linear frekuensi tinggi")














 131")
-131 THERAPY FOR: 1. 2. Hyperthyroid ( Thyrotoxicosis) Thyroid cancer: 1. Papillary 2.")
 – autoimmune Toxic adenoma –")











")













- Slides: 51
RADIODIAGNOSIS AND NUCLEARTHERAPY FOR THYROID DISEASE Hesti Gunarti Departemen Radiologi FK UGM/RSUP DR Sardjito
THYROID
Radiodiagnosis for Thyroid Disease 1. 2. 3. 4. Ultrasonography CT Scan MRI Thyroid scintigraphy
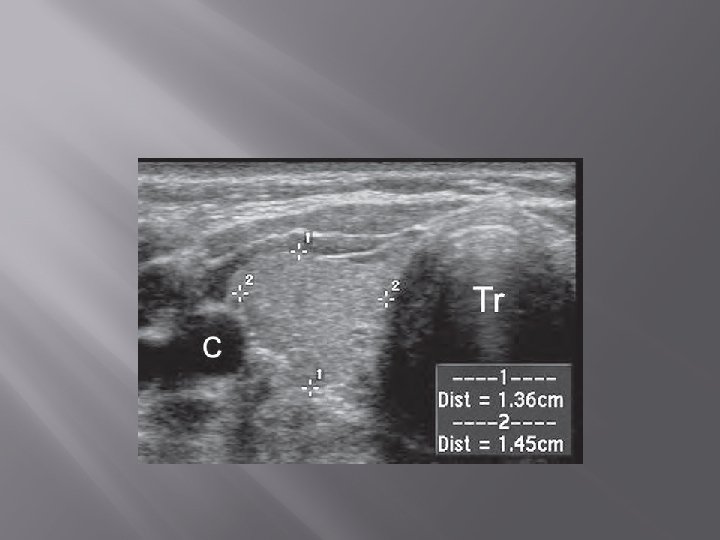
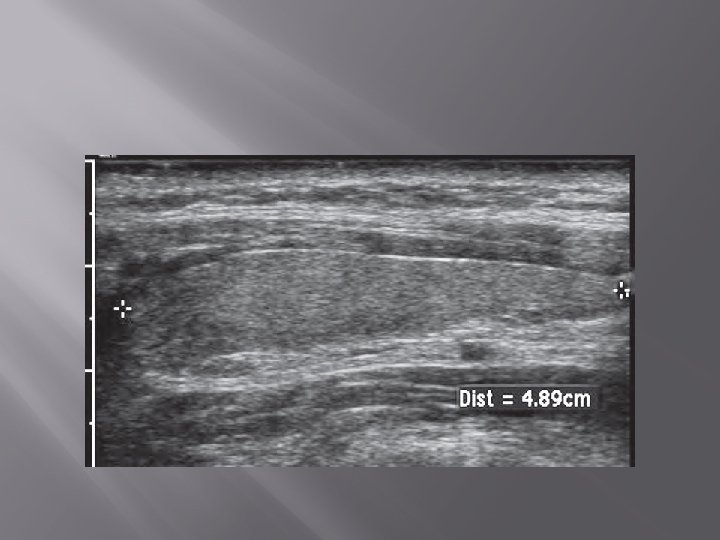
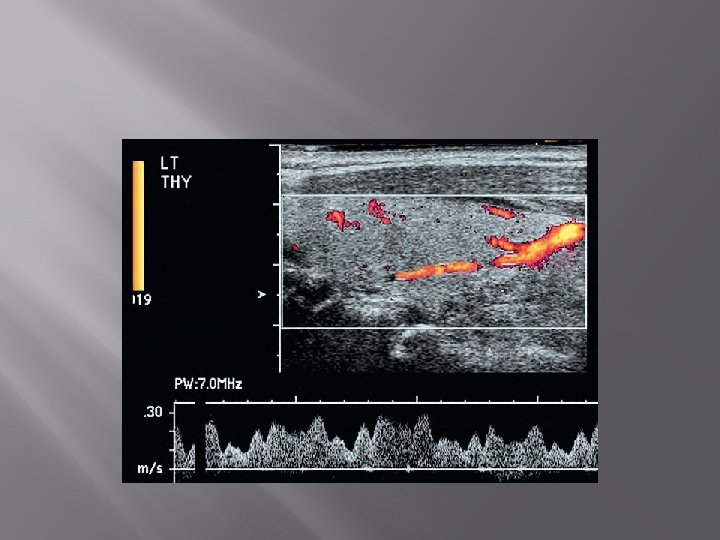
1. Ultrasonography (USG) � � Gray scale, color Doppler Transducer : linear frekuensi tinggi (7. 5 -15. 0 MHz)
� � Ukuran normal kelenjar thyroid orang dewasa Indonesia : 4 -4, 8 cm x 1, 0 -1, 8 cm x 0, 8 -1, 6 cm. Berat normal : neonatus 2 -3 gram. Orang dewasa 18 -20 gram
� Normal thyroid parenchyma has a homogeneous, medium-level to high-level echogenicity that makes detection of focal cystic or hypoechoic thyroid lesions relatively easy in most cases.
Gray scale
Color Doppler
2. CT Scan
3. MRI � Jarang dikerjakan
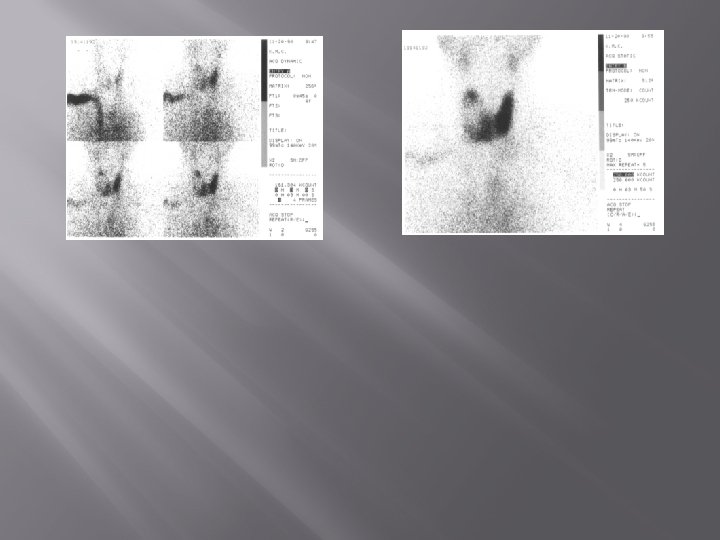
4. Thyroid scintigraphy
PEMERIKSAAN TIROID SKENING Radiofarmaka 1. Tc-99 m Pertechnetate 2. I-131 Pengambilan citra 1. Dinamik 2. Statik 3. Total body
Thyroid scintigraphy � � Thyroid nodule Congenital hypothyroidism Thyroid cancer follow up 131 I treatment
Tiroid normal dengan Te-99 m
Struma multinoduler
“Cold nodule” solitary
I 131
NUCLEARTHERAPY FOR THYROID DISEASE � Radioisotop : Iodine (I) 131
IODINE (I)-131 THERAPY FOR: 1. 2. Hyperthyroid ( Thyrotoxicosis) Thyroid cancer: 1. Papillary 2. Follicular 3. Mixed papillary and follicular
HYPERTHYROIDISM � � � Toxic diffuse goiter (Graves’ disease) – autoimmune Toxic adenoma – more common in elderly Toxic multinodular goiter- more common in elderly Painful subacute thyroiditis – viral infection Excessive iodine intake – too much hormone production Excessive thyroid hormone replacement therapy
Hyperthyroidism: Graves’ disease
Diagnosis � � � Clinical history and physical examination Routine thyroid hormone function test FT 4, T 4; T 3, FT 3. Thyroid autoantibodies, antithyroid peroxidase, antithyroglobuline antibodies. Radioactive iodine uptake Radioactive thyroid scan Tc-99 m and/or I-131
SIGN AND SYMPTOMS 1. 2. 3. 4. 5. 6. 7. Central nervous system Eye, ear, nose, and throat Musculoskeletal Skin / hair Cardiac Gastrointestinal Genitourinary
The criteria for establishing the diagnosis 1. 2. 3. Subtle symptoms and sign of hyperthyroidism A normal FT 4 level A suppressed serum TSH level
THERAPY General therapy 1. 2. Surgical Intervention Anti thyroid drugs Specific therapy Radioactive iodine (I)-131 is the most common form of therapy in USA. It is used if the general therapy is not response or not possible to be done
INDICATION Treatment of choice: Graves’ disease • Toxic nodular goiter • 25% pt will become hypothyroid 1 year later and will continue to increase yearly • If smaller doses are used, there is a higher incidence of recurrences of hyperthyroidism •
CONTRAINDICATION � � Pregnancy Breastfeeding
DOSES � � 185 – 553 MBq atau 5 – 15 m. Ci
COMPLICATION � � Permanent hypothyroidism Prevalence rises at a rate of 2 -3% per year
� � The success rate of I-131 therapy: �May vary from 75% - 100% Side effect: �Life long hypothyroidism (Radioiodine treatment of hyperthyroidism: prognostic factors for outcome. J Clin Endocrinol Metab. 2001. Aug; 86 (8): 3611 -7)
THYROID CANCER � � Incidence: varies 1 -4/100. 000/year Histological types: � Papillary(paling � Follicular � Anaplastic sering/most case)
THYROID CANCER Papillary: The most common, usually affects women of child bearing age (CBA) Follicular: 30% of all cases, greater rate of recurance and metastasis Medullary: Familial, the symptoms similar to Chushing’s Syndrome Anaplastic: Giant and Spindle Cell Cancer, the most malignant form, does not response to radioiodine therapy, quickly metastasis, invades nearby structures i. e trachea, causing compression, breathing difficulties
THYROID CANCER 1. Papillary cancer: a. b. c. Not an aggressive tumor Metastasizes locally 10 -years survival time more than 90% 2. Follicular cancer: a. b. More aggressive Metastasizes via the bloodstream
PREVENTION NO KNOWN PREVENTION
SYMPTOMS � � � Enlargement of thyroid gland or neck swelling Hoarseness or changing voice Cough or cough with bleeding Diarhea or constipation Very depending on the type of thyroid cancer
TESTS � Biopsy of the thyroid: � Anaplastic, � follicular, medullary, papillary US of the thyroid: � Nodule � Thyroid scan: � Cold � nodule Laryngoscopy: � Paralyzed � vocal cords Serum calcitonin: � Elevated � T 3, T 4, dexametasone supression test, CEA
Malignant follicular neoplasms
Multicentric medullary thyroid carcinoma
Seorang wanita 36 th dengan benjolan pada leher THYROID SCINTIGRAPHY Cold nodule” solitary
THERAPY OF DIFFERENTIATED THYROID CANCER � � SURGICAL RESECTION RADIOTHERAPY IN MANY CASES (RADIATION THERAPY WITH I-131)
RADIOIODINE THERAPY � � � � Thyroid scan: Tc-99 m and I-131 Blood routine, LFT (GOT/PT), KFT (Ur & Crea). Bone scanning, USG liver. Dosage: 100 -150 m. Ci orally. TB scan 10 days after I-131 Tx Follow-up: 2 w, 4 w, 1 m, 3 m, 6 m, and 12 m I-131 TB scan 6 m, 12 m.
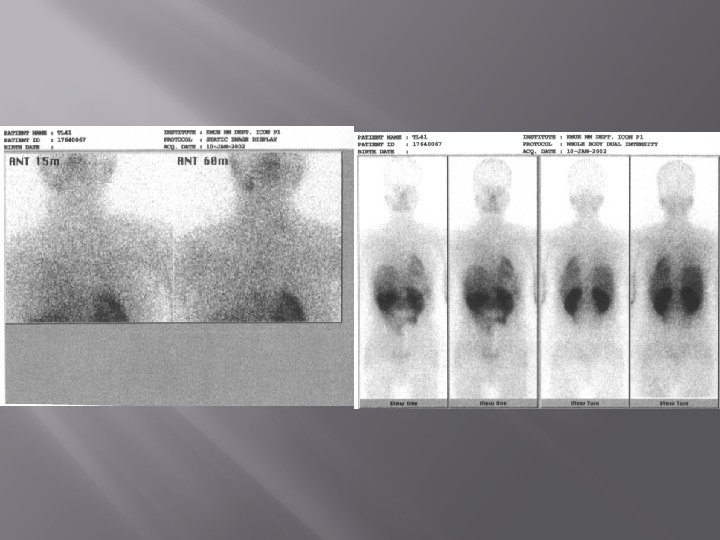
RADIOIODINE THERAPY Thyroid remnant Before ablated Thyroid remnant After ablated
I-131 TB SCAN 24 H AFTER TX
IS RADIOACTIVE IODINE SAFE? � � The long term safety seems excellent No excess cancer mortality after decades of follow-up. (Long term comparative cancer mortality after use of radioiodine in treatment of hyperthyroidism a fully reported multicenter study. J Insur Med. 2001; 33 (2): 13742) � There does not appear to be any significant excess total cancer mortality in patients after radioactive iodine therapy. (JAMA 1998 ; 280: 347355. The Lancet 1999; 353 : 2111 -2115)
1. Laki-laki 48 th post operasi total thyroidectomy karena malignansi thyroid. Sisa kelenjar thyroid yg sakit yang masih ada pada thyroid scan dengan TC-99 m 2. THYROID SCANN PRE RADIASI DAN POST RADIASI