Prevalence Age Sex and agespecific prevalence of migraine


 Age Sex- and age-specific prevalence of migraine (Taipei)")

, 2004 Part one: Primary")
 (migraine without aura)- common migraine q 有預兆偏頭痛 (ICHD-II")



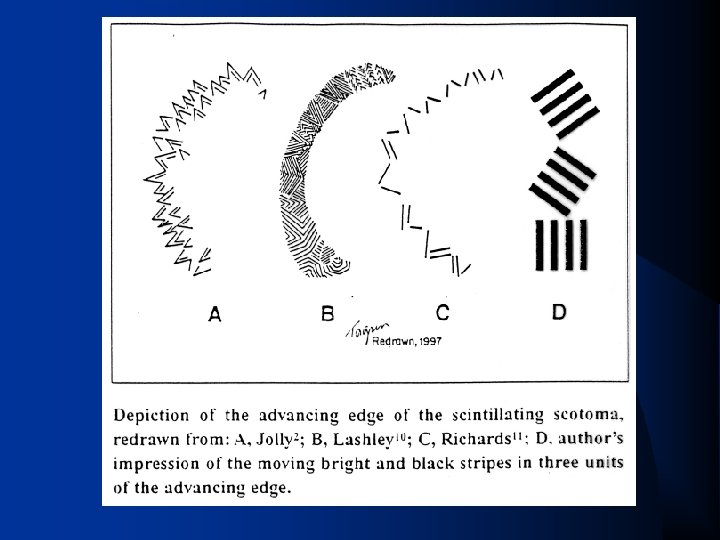
![Aura (預兆) q q visual symptoms (spots of light, scotoma, fortification [scintillating scotoma], zig-zag),](https://slidetodoc.com/presentation_image/4b1bc8567ff15df0befbd53d5a4140f0/image-18.jpg "Aura (預兆) q q visual symptoms (spots of light, scotoma, fortification [scintillating scotoma], zig-zag),")


 q A. At least 5 attacks 1 fulfilling criteria B–D")
 q 1. 5. 2 Status migrainosus v")
 Headache fulfilling migraine without aura on 15 days/month for")




 q CADASIL (cerebral autosomal dominant")
")
")
 q FHM 1: 19 p 13 missense mutations in CACNA")
: vrecurrent subcortical")








 vneurogenic plasma")





 (1) first or worst")
 2. 抗多巴胺藥物: 抗精神藥物、止吐劑、助腸蠕動劑 3. 麥角胺鹼 4. 輕度止痛藥 (aspirin與acetaminophen")

 原作用是抗精神藥物、止吐劑或 助腸蠕動劑 q 控制噁心、嘔吐。 q 可加強藥物於腸胃道吸收。 q metoclopromide(10 mg)(Primperan) prochlorperazine(10 mg)(Novamin)")





 q Epidemiology (USA): v 38% for one-year prevalence (female 42% and")


 men predominantly, q increasing in females in the Western countries, q")
 q q q q q very severe 'stabbing' pain over the")




 Tics q onset late in life (6 th and 7 th")



- Slides: 105
Prevalence (%) Age Sex- and age-specific prevalence of migraine (Taipei)
q Primary vs. secondary headache
The International Classification of Headache Disorders 2 nd edition (ICHD-II), 2004 Part one: Primary headaches 1. Migraine 2. Tension-type headache 3. Cluster headache and other trigeminal autonomic cephalalgias 4. Other primary headache Part two: The secondary headache 5. Headache attributed to head and /or neck trauma 6. Headache attributed to cranial or cervical vascular disorders 7. Headache attributed to non-vascular intracranial disorder 8. Headache attributed to a substance or its withdrawal 9. Headache associated with noncephalic infection 10. Headache attributed to disorder of homoeostasis 11. Headache or facial pain attributed to disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranial structures 12. Headache attributed to psychiatric disorder Part three: Cranial neuralgias, central and primary facial pain and other headaches 13. Cranial neuralgias and central causes of facial pain 14. Other headache, cranial neuralgia, central or primary facial pain
國際頭痛學會偏頭痛分類 無預兆偏頭痛 (ICHD-II code 1. 1) (migraine without aura)- common migraine q 有預兆偏頭痛 (ICHD-II code 1. 2) (migraine with aura)- classical migraine q 10: 1 to 3: 1
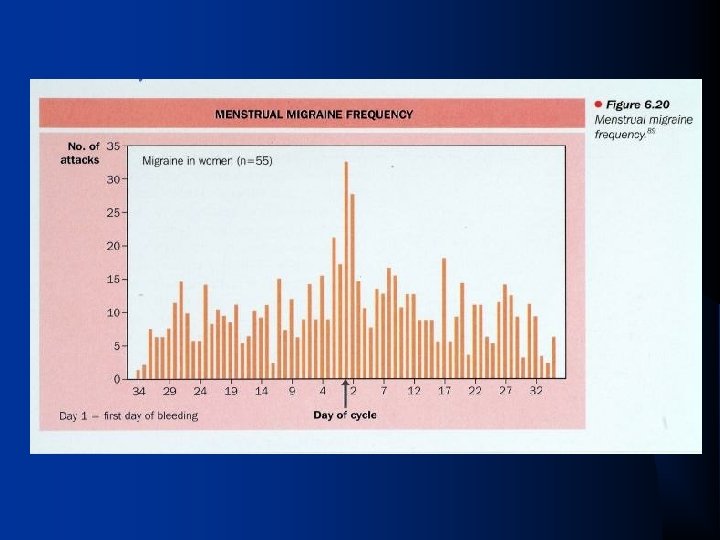
Headache profiles for migraine “Migraine, the Sick-headache” q Moderate to severe headache, q Onset between 10 -30 y/o, female predominant (3: 1) q Unilateral, pulsating, exacerbated during physical activities, functions prohibited or inhibited, associated with nausea, vomiting, photophobia, phonophobia, q Duration 4 to 72 hours; frequency varied (most 1/month) q Triggers: hypoglycemia, menstruation, red wine, stress, poor sleep, 3 C q Phases: prodrome, aura, headache, postdrome
Phases of Migraine Pre-Headache Premonitory symptoms Headache Aura Post-Headache Postdrome Migraine phase slide Mild © 2000 Primary Care Network Moderate Severe Rescue
Premonitory symptoms 前趨症狀
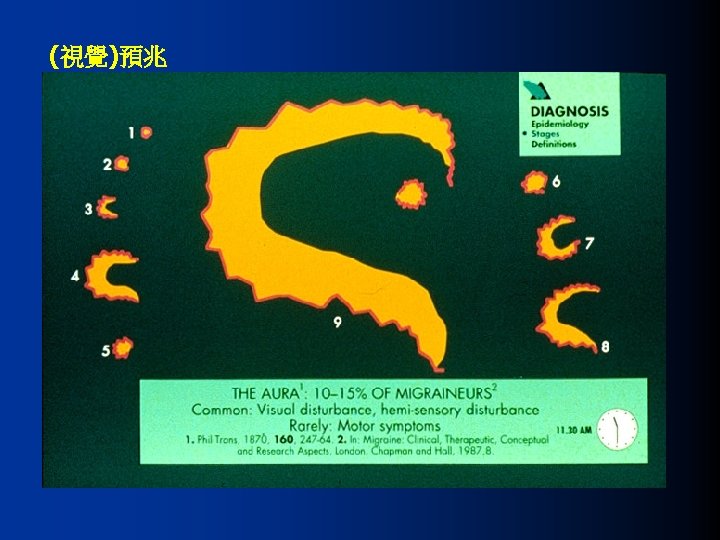
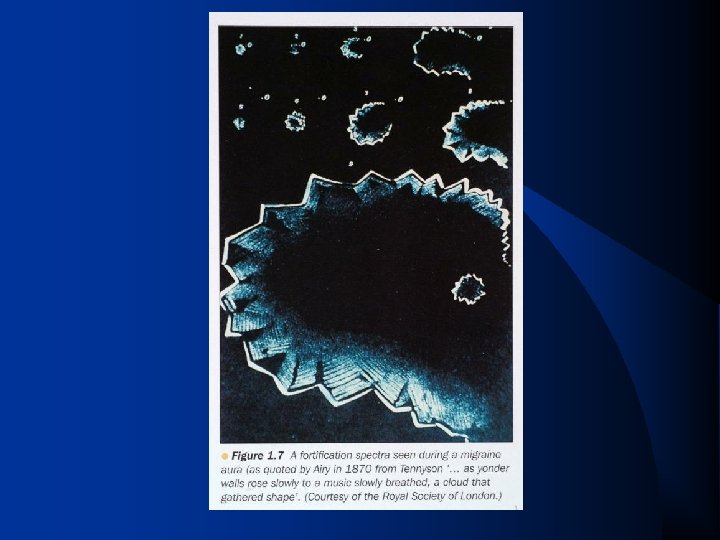
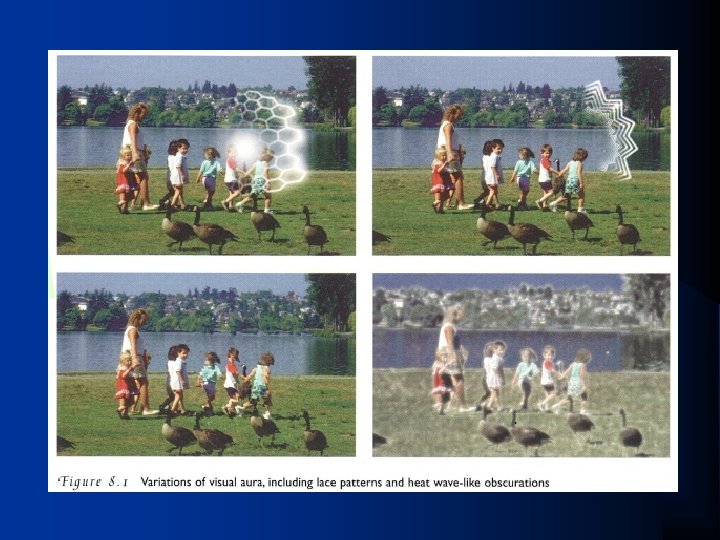
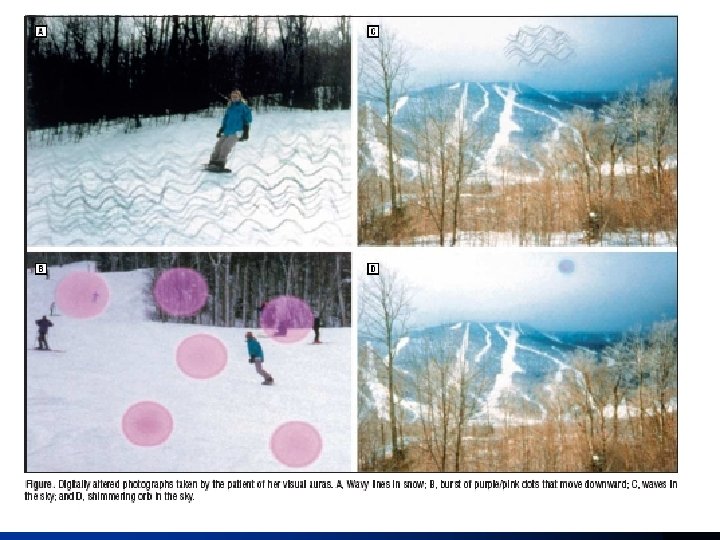
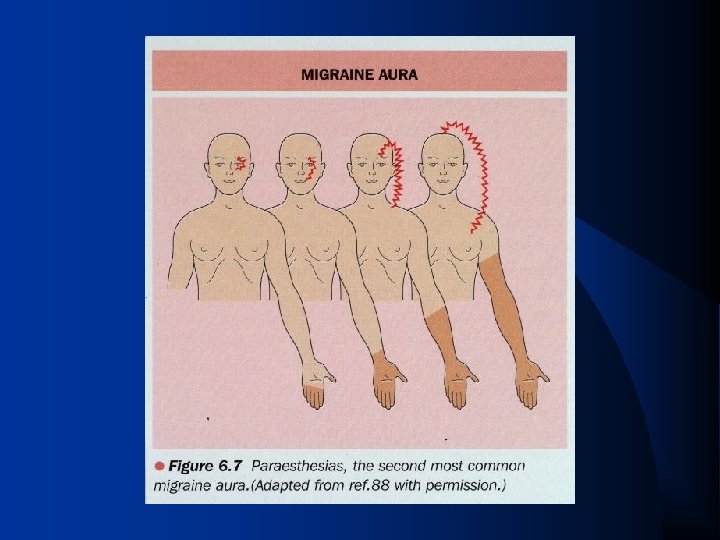
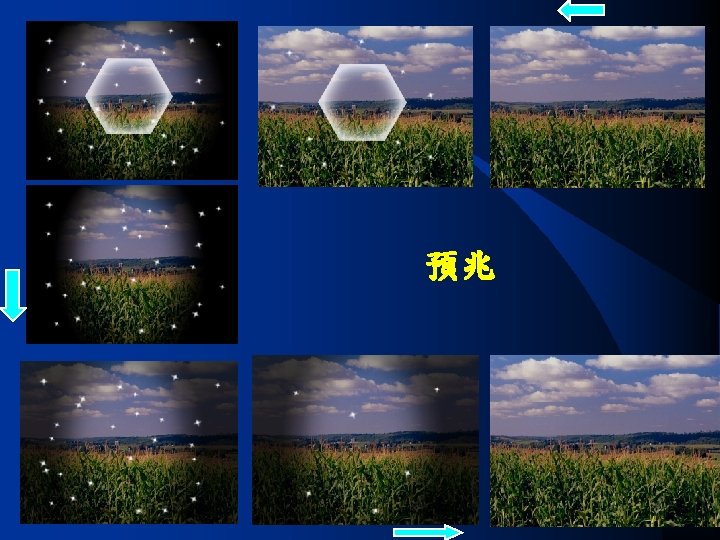
Aura (預兆) q q visual symptoms (spots of light, scotoma, fortification [scintillating scotoma], zig-zag), hemifield aphasia, sensory symptoms motor weakness q q q EXPLAINED BY FOCAL NEUROLOGICAL DEFICIT Reversible, lasting 5 to 60 minutes, headache follows within 1 hour
Migraine without aura (ICHD-II) q A. At least 5 attacks 1 fulfilling criteria B–D q B. Headache attacks lasting 4– 72 hours (untreated or unsuccessfully) C. Headache has at least two of the following characteristics: q q v v q 1. unilateral location 2. pulsating quality 3. moderate or severe pain intensity 4. aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs) D. During headache at least one of the following: v 1. nausea and/or vomiting v 2. photophobia and phonophobia q E. Not attributed to another disorder
Complications of migraine (ICHD-II code 1. 5) q 1. 5. 2 Status migrainosus v Headache lasts 72 hour whether treated or not v Severe headache q 1. 5. 4 Migrainous infarction v. Migraine with aura and > 60 minutes v. Neuroimage reveals ischemic infarction in the relevant area
Chronic migraine (1. 5. 1) Headache fulfilling migraine without aura on 15 days/month for 3 months q Medication overuse headache should be excluded q The most disabling type of chronic daily headache ( 15 days/month for 3 months) q
Migraine Transformation Episodic Migraine Tension-Type headache Mixed Headache Time Chronic Daily Headache
Migraine Symptomatology Hypersensitivity q vessels pulsing normally can be felt to throb; q fluid in an otherwise satisfied stomach is perceived as nausea; q normal lights, sounds, or smells are perceived as pungent or unpleasant; q and normal movement is perceived to jar and disturb the head.
Pathophysiology of Migraine q What causes migraine? vgenetic component va diathesis or constitution liable to headache
Genetics of Migraine q q q 70% positive family history (one parent: 46%, both parents: 66%) stronger relationship with migraine with aura multiple genes vs. monogene
Genetic study of migraine q Familiar hemiplegic migraine (FHM) q CADASIL (cerebral autosomal dominant arteriopahty with subcortical infracts and leukoencephalopathy)
1. 2. 4 Familial hemiplegic migraine (FHM)
1. 2. 4 Familial hemiplegic migraine (FHM)
Familial hemiplegic migraine (FHM) q FHM 1: 19 p 13 missense mutations in CACNA 1 A, which encodes the pore-forming 1 subunit of voltage -gated neuronal Cav 2· 1 (P/Q-type) calcium channels. (Ophoff et al. Cell 1996) q FHM 2: 1 q 23 missense mutations in ATP 1 A 2, which encodes the 2 subunit of the Na+/K+ pump (De Fusco et al. Nat Genet 2003) q FHM 3: 2 q 24 missense mutation in SCN 1 A, which encodes the neuronal voltage-gated sodium channel Nav 1· 1 (Dichgans et al. Lancet 2005)
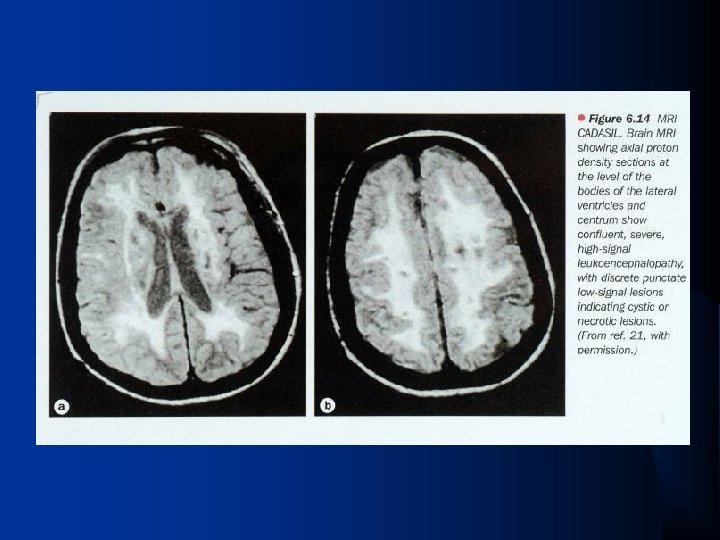
CADASIL q CADASIL (cerebral autosomal dominant arteriopahty with subcortical infracts and leukoencephalopathy): vrecurrent subcortical ischemic events vdementia (90% before death) vmigraine with aura (22%) v. Depression v. Chromosome 19, notch 3, point mutation
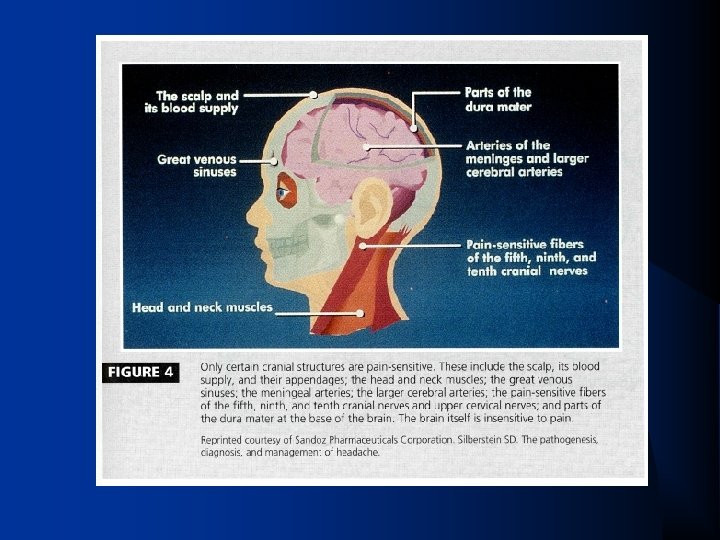
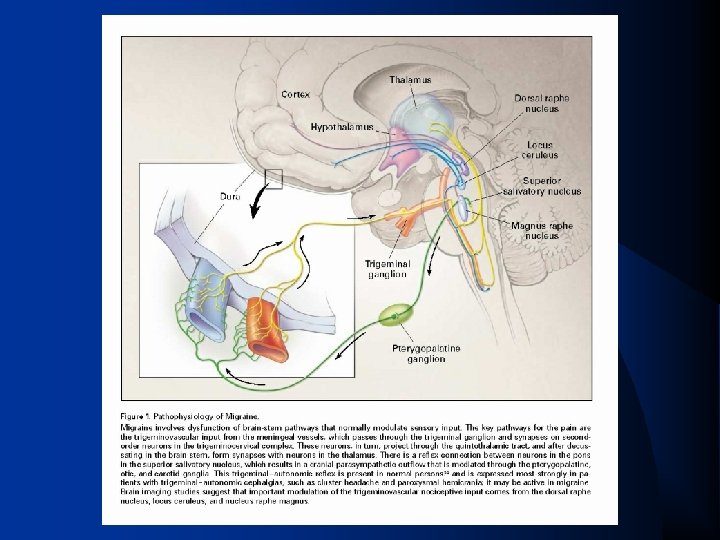
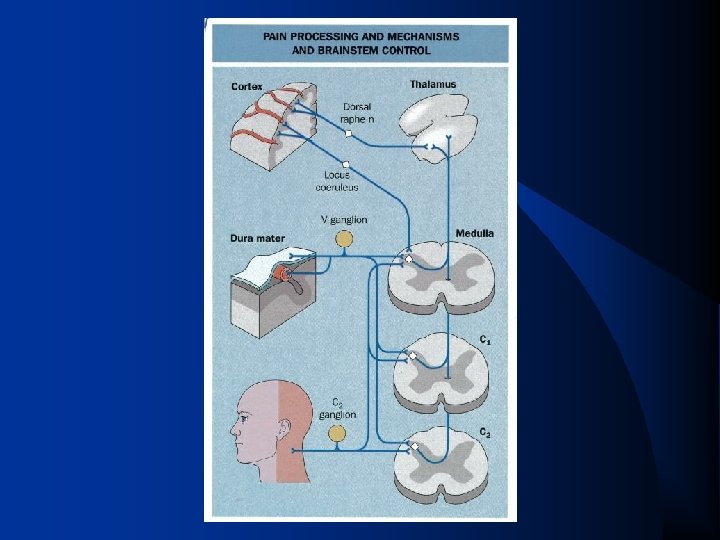
Pathophysiology of Migraine q Numb Brain: q Pain sensitive: skin, subcutaneous tissue, muscle, extracranial arteries, periosteum of the skull, venous sinuses, dura, middle meningeal and superficial temporal arteries, CN 2, 3, 5, 9, 10, first three cervical nerves q Traditional view: v tension-type headache: ”muscle theory” v migraine: “vascular theory”
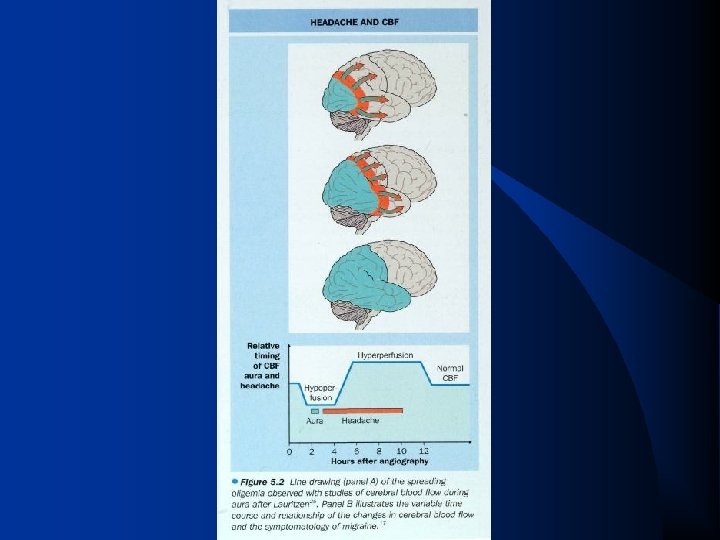
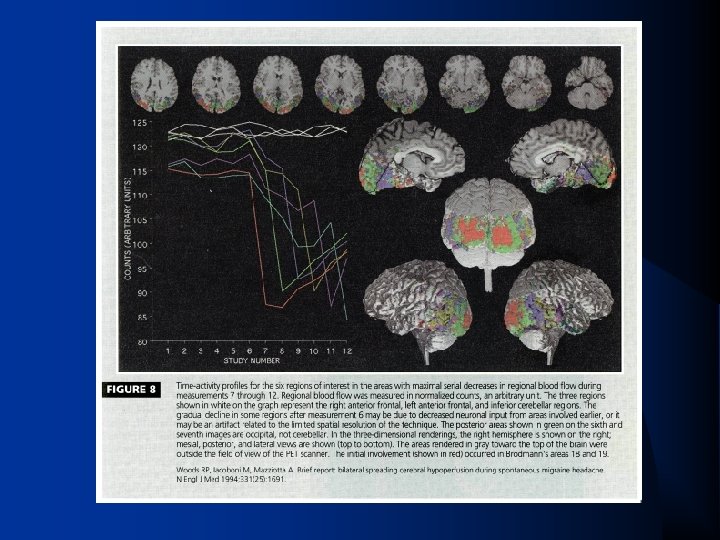
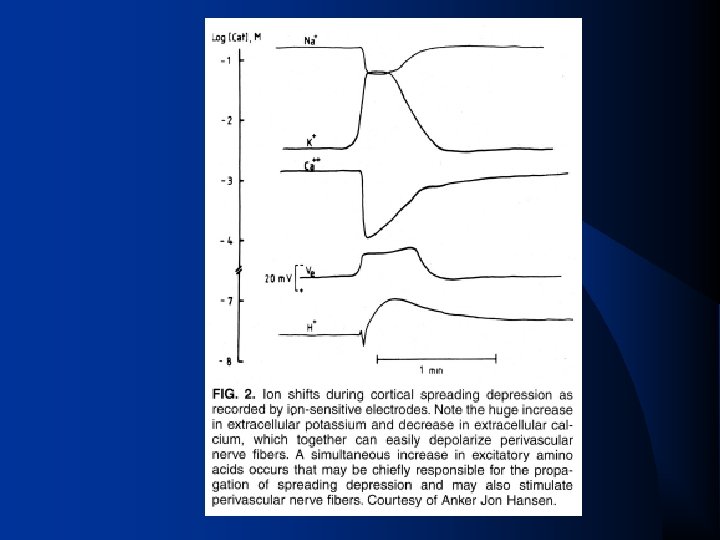
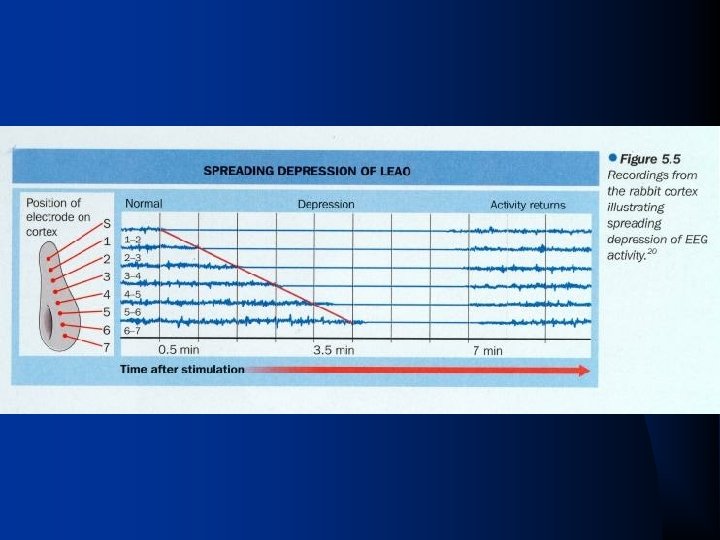
Aura- mechanisms spreading cortical depression of Leao 1 -3 mm/min q q cerebral blood flow reduction v spreading oligemia v posterior cortex (area 7 and area 19) v reduction enlarged to whole hemisphere flow changes in both with and without aura v flow-headache relationship is complex v Aura : initiator of migraine or parallel presentation?
margarita
Top, High-field magnetic resonance images of an "inflated" right cerebral hemisphere taken across a course of 20 minutes, including 12 minutes after the onset of exercise-induced migraine aura paracentrally in the left visual field (arrow) Spierings, E. L. H. Arch Neurol 2004; 61: 794 -799. Copyright restrictions may apply.
Blood flow and visual aura GB_15
30 minutes 6 hours 3 hours 24 hours
Blood flow through migraine attacks gb_18
Cortical spreading depression CSD. avi
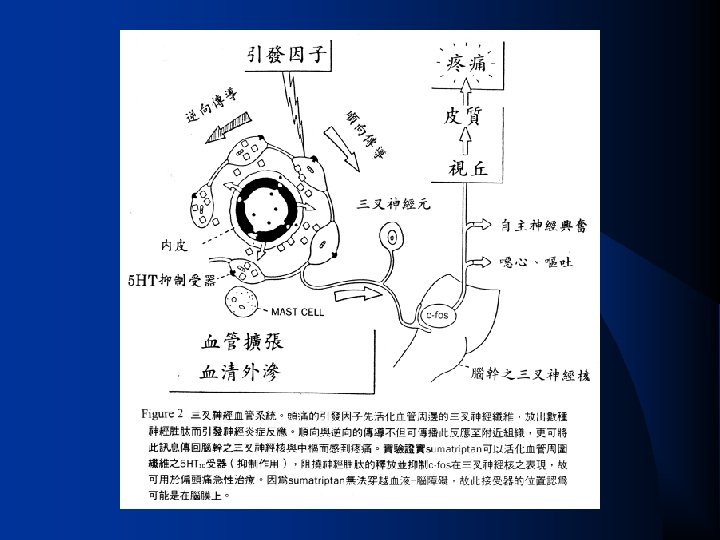
Headache q Source of Pain vcarotid artery dilatation vsterile neurogenic inflammation (Moskowitz) vneurogenic plasma extravasation as an index § blocked by 5 -HT 1 B/D-like agonist (such as sumatriptan),
Pulsation of temporal artery decreases after ergotamine treatment
Neurogenic inflammation GB_23
Classification of Serotonin Receptors modern 5 -HT 1 A, 1 B, 1 D, 1 F q 5 -HT 2 A, 2 B, 2 C q 5 -HT 3 q 5 -HT 4 q 5 -HT 5 A, 5 B q 5 -HT 6 q 5 -HT 7 q
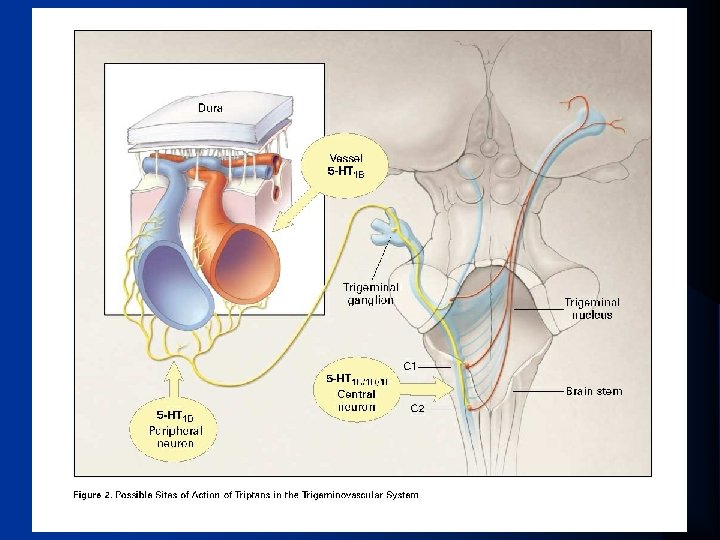
Therapy and Pathophysiology q 5 -HT 1 B/D -like agonist v 1 B more cerebrovascular receptors v 1 D more trigeminal neuronal receptors trigeminovascular system— the common focus of activity for vascular headaches q
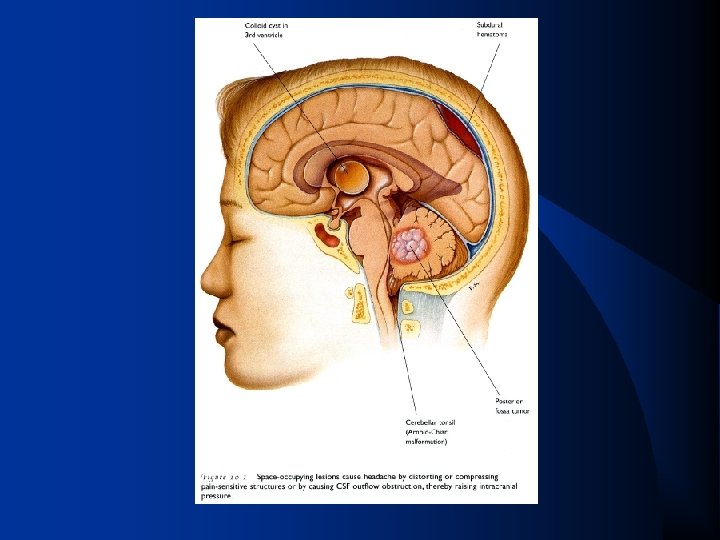
How to work out headache patients why further study? q q q History: headache profile, painkillers, triggers…. . physical exam lab neuroimaging studies: CT scan or MRI, EEG ? lumbar puncture other specialty: ENT, dentist, psychiatrist (associated with major depression, panic disorder, and generalized anxiety disorder), rehabilitation for neck problems
what patients should be kept an eye on? (secondary headaches) (1) first or worst headache (2) with fever (3) with confusion (4) post-traumatic (5) changing pattern (6) with convulsion (7) on awakening (8) nuchal rigidity
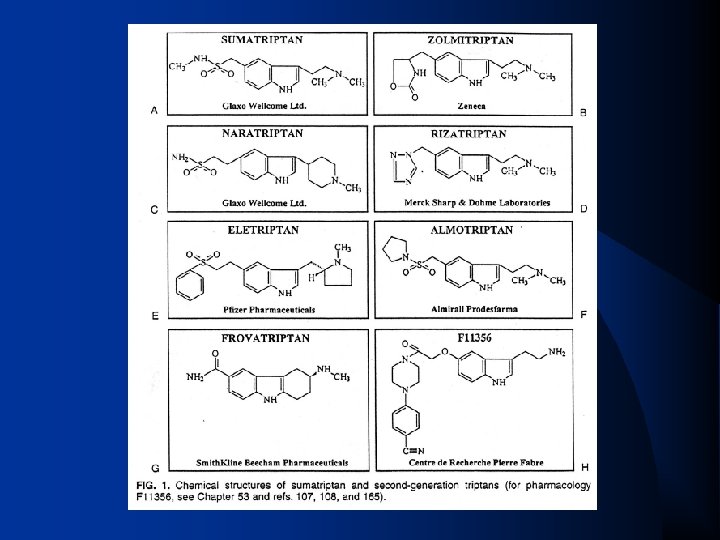
急性發作處理 1. Triptans (翠普登 英明格 Sumatriptan(Imigran) 2. 抗多巴胺藥物: 抗精神藥物、止吐劑、助腸蠕動劑 3. 麥角胺鹼 4. 輕度止痛藥 (aspirin與acetaminophen or combinations with or without caffeine) 5. NSAIDs 6. 類固醇 7. 麻醉劑
抗多巴胺藥物 (Anti-dopaminergic agents) 原作用是抗精神藥物、止吐劑或 助腸蠕動劑 q 控制噁心、嘔吐。 q 可加強藥物於腸胃道吸收。 q metoclopromide(10 mg)(Primperan) prochlorperazine(10 mg)(Novamin) promethazine(12. 5 -25 mg)(Pyrethia) droperidol(2. 5 mg) q
Triptans 台灣上市︰sumatriptan 50 健保給付︰sumatriptan 50 mg (每月八顆� 通過審核︰rizatriptan 10 mg naratriptan 2. 5 mg sumatriptan nasal spray 20 mg zomitriptan 2. 5 mg 完成臨床試驗︰eletriptan 40, 80 mg (未通過� 。
Tension-type Headache (緊縮型頭痛) q Epidemiology (USA): v 38% for one-year prevalence (female 42% and men, 36% ) q Headache profile: v. Episodic or chronic ( < or >= 15 days/month) v. Most frequent headaches, v. Mild to moderate, v. Bilateral, non-pulsating (band-like), vfunctions mildly or not inhibited, v. Duration varied 30 minutes to 7 days, v. No marked accompanied symptoms
Tension-type headache
Treatment Acetaminophen, aspirin, q NSAIDs, q biofeedback q TCA could be used as preventive agents q
Cluster Headache (叢發性頭痛) men predominantly, q increasing in females in the Western countries, q very low prevalence 0. 1 -0. 3% (USA), q onset 20 to 40 q
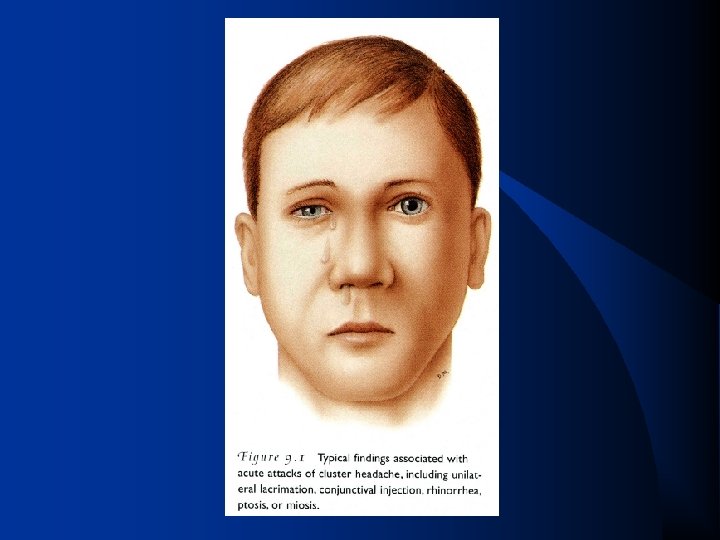
Cluster Headache (叢發性頭痛) q q q q q very severe 'stabbing' pain over the retro-bulbar region, unilateral, coming in clusters, lasting 2 -3 months, each headache 30 -90 (15 -180) minutes, autonomic symptoms (nasal congestion, rhinorrhea, lacrimation, conjunctival injection, forehead and facial sweating, miosis, ptosis, eyelid edema) restlessness 1 -8 times a day attacks of frequently fixed time schedule occurring most frequently during sleep
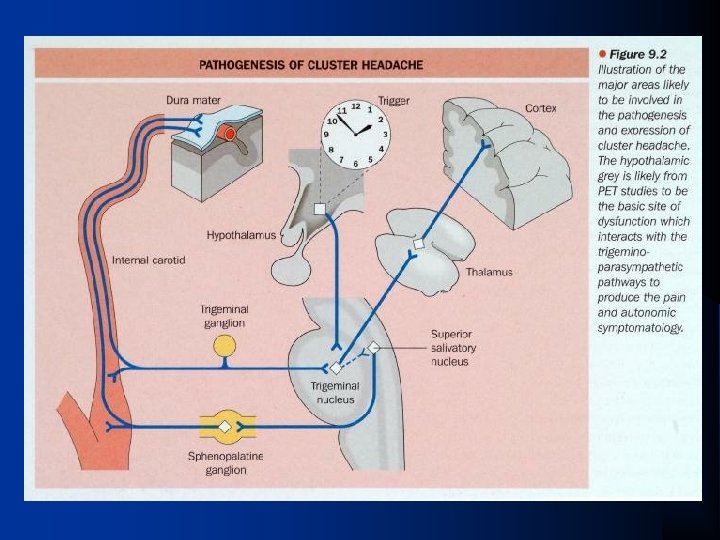
Mechanisms Hypothalamus lesion? Circadian rhythm dysfunction?
Autonomic mechanism of cluster headache
Hypothalamus in cluster period
Treatment of cluster headache q Abortive agents: q Preventive agents: voxygen inhalation v steroids vergotamine vdihydroergotamine, v verapamil v lithium vsumatriptan v methysergide v valproic acid
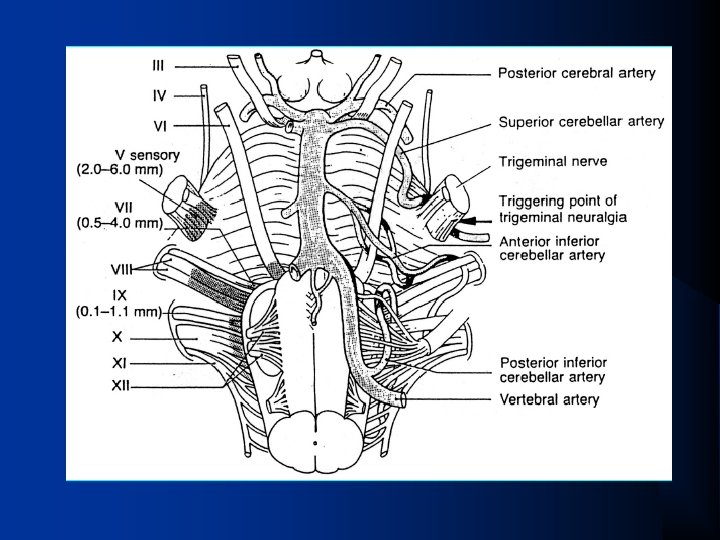
Trigeminal Neuralgia (三叉神經痛) Tics q onset late in life (6 th and 7 th decades), more in females Pain Characteristics: q vbrief (seconds to less than 2 minutes) vunilateral (95 -97%) paroxysms of electric-like and lanciating pain, distributed V 2 -3 (<5% in V 1) vmaximum intensity lasting a second or slightly longer and repetitively v‘triggers’: brushing teeth, chewing, talking, cold wind to the face, etc.
Mechanism focal demyelination of the trigeminal nerve q vascular compression just prior to entry into the pons (88%) q 6% tumor or aneurysm, 6% multiple sclerosis q
Treatment q Medical: vcarbamazepine, phenytoin, baclofen, valproic acid, lamotrigine q Surgery: v. Jenetta's operation: decompression of 5 th nerve v. Gamma Knife
Thank you for your attention!