Top Ten Headache Tips Dr David PB Watson

Top Ten Headache Tips Dr David PB Watson GPw. SI Headache Hamilton Medical Group Aberdeen

Top Tip 1 • • Diagnosis is by history, history and history T timing O other associated symptoms S site S severity I influences aggravating/relieving factors T type: what it feels like

Top Tip 2 • Secondary Headache is Rare • Studies show PPV headache 0. 09% in primary care for brain tumour i. e. 1 in 1000 • Migraine CT Scan 2 in 1000 abnormal • Neurology OPD: 1 in 100 secondary cause • A and E : 1 in 10 secondary cause
 or expert opinion (Level 4) • •")
“Red flags” • Single cohort (Level 3) or expert opinion (Level 4) • • • • new onset headache in patients who are aged over 50 29 -31 abrupt onset (thunderclap) 28 -30, 32, 33 focal symptoms including atypical aura greater than one hour 28, 32, 34, 35 abnormal neurological examination 28, 29, 35, 36 altered mental status 28, 30, 34 altered characteristics or associated features of headache 28, 31 headache that changes with posture 37 headache worse during physical activity, and the valsalva manoeuvre 28, 38 patients with risk factors for thrombosis 34, 39, 40 new onset headache in a patient with a history of HIV infection 41 jaw claudication 16 neck stiffness 30 fever 42 new onset headache in a patient with a history of cancer 9
")
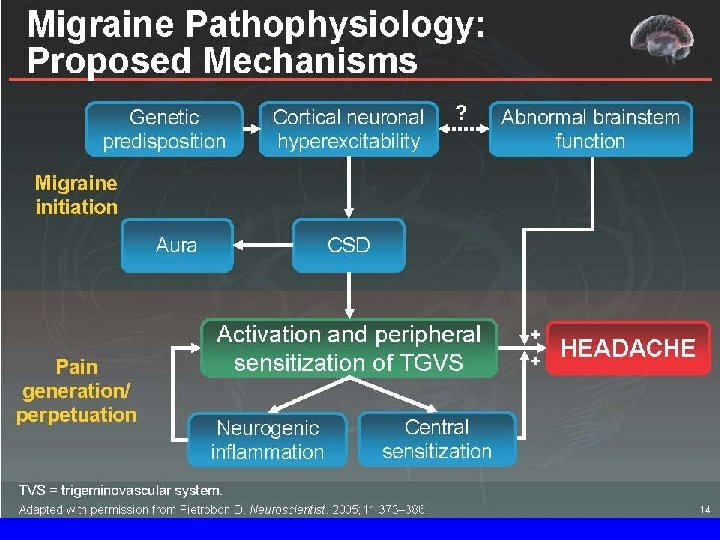
Episodic primary headaches Cluster Migraine +/aura Episodic primary headaches Probable migraine Tension-type headache (TTH)

Chronic primary headaches / chronic daily headaches New daily persistent Hemicrania continua Chronic daily headache (CDH) Chronic migraine +/medication overuse Chronic tension Chronic cluster

Top Tip 3 • Episodic disabling headache is migraine • Over diagnosis of sinus headache and TTH • 40% migraineurs miss ICHD-II criteria

What features make migraine more likely? • • episodic severe headache that causes disability 11, 23, 24 nausea 16, 23 sensitivity to light during migraine headache 16, 23 sensitivity to light between migraine attacks 25 aura 16, 18 sensitivity to noise 16 exacerbation by physical activity 16 • positive family history of migraine 16 • The features which give the greatest sensitivity and specificity are Disability, Nausea and Sensitivity to light 23 – ID Migraine validation study (Level 3)

Top Tip 4 • Choose acute migraine medication according to the patient’s symptoms • Can use a step approach

Top Tip 5 • Response to triptans is idiosyncratic and consistency across attacks is variable

Top Tip 6 • A good response to migraine prophylaxis is a 50% response in 50% of patients • Choice of prophylaxis is guided by comorbidites • Pizotifen is a poor drug

Top Tip 7 • Migraine with aura is an absolute contraindication to the combined contraceptive due to increased stroke risk

Top Tip 8 • All headache medications can cause headache

Top Tip 9 • There is no magic answer to the management of medication overuse headache other than to stop the medication

Top Tip 10 • Short lasting unilateral headaches with autonomic symptoms think of the trigeminal autonomic cephalalgias (TACs)

What features make TACs more likely? • The following features differentiate trigeminal autonomic cephalalgias from migraine: 16, 26 (Level 4) – – Onset: rapid in TAC, gradual in migraine Duration: TACs < 3 hours, migraine 4 - 72 hours Frequency: multiple attacks may occur daily in TACs Restlessness during an attack: 100% in cluster headache, 50% in paroxysmal hemicrania – Prominent ipsilateral autonomic features in TACs

Take home points • • • migraine common history is key to diagnosis impact is important remember overuse of medication tailor treatment to patient Refer if red flags, consider for chronic migraine/MOH, TACs, untoward patient angst

Any Questions?

Case 1 • • 22 years age Episodic headache for 5 years Attended for COP check What do you want to know?

Case 2 • 47 year old man • 2 migraine headaches 6 and 10 years ago • 3/12 ago had 3 weeks of headache awaking him from sleep • What do you want to know?

Case 3 • • • 27 year old lady Migraine since 16 Frequency is 1 -2 per month Woke at 5 am with worst ever migraine What do you want to ask her?

Case 4 • • 75 year old male migraine since 15, none for 10 years Last 3 days had migraine like headache Called GMEDs at 6 am as had D and V all night and still has headache • What do you want to ask him?

Case 5 • 40 year old man severe headache for 1 hour • Previous similar headaches diagnosed as migraine • Not responded to naratriptan 2. 5 mg • What do you want to ask him?

Case 6 • 48 year old lady • Migraine since 16, menstrually associated, none when pregnant • Last 2 years more frequent • Big headaches twice a month • Little headaches 3 times a week • What do you want to know?

Case 7 • 53 years, migraine since 15 • Last 6 years headache every day • History of depression, agoraphobia, back pain • Very noticeable profound parkinsonism tremor • What do you want to know?

Abbreviated diagnostic checklist based on IHS 2004 criteria Migraine Probable migraine Tension-type • Recurrent Essential (3) • Recurrent • No organic disease • Duration 4 -72 h • Duration 0. 5 h-7 days Essential (2) • • Unilateral Pulsating Moderate / severe Aggravated by movement • Moderate / severe + one other Essential (1) • Nausea / vomiting • Photo / phonophobia • Generalised • Pressure / tightness • Slight / moderate • Photo / phonophobia Essential (3) = all items essential for diagnosis; Essential (2) = two items from list essential for diagnosis; Essential (1) = one item from list essential for diagnosis IHS 2004

The migraine attack Symptom intensity Associated symptoms Prodrome Aura Headache Time Postdrome

Prodrome • 60% of migraine sufferers experience premonitory phenomena Excitatory Inhibitory l Irritability l Mental / physical slowing l Elation l Poor concentration l Hyperactivity l Word finding difficulty l Yawning l Weakness / fatigue l Food cravings l l Photophobia / phonophobia Constipation / abdominal bloating l Anorexia l Chill l Increased bowel / bladder activity

Aura • Affects 33% of migraine sufferers, but not in all attacks • Transient neurological symptoms resulting from cortical or brainstem dysfunction • May involve visual, sensory or motor systems • Can occur before or during headache phase • Slow evolution of symptoms • Lasts for 20 -60 minutes • Can be confused with transient ischaemic attack Ferrari 1998 Spierings 2003 Russell & Olesen 1996

Headache phase • Throbbing or pounding quality • If left untreated, headache pain will progress to moderate / severe intensity • Duration – 4 -72 hours in adults – 2 -8 hours in children • • Exacerbated by movement* One-sided temporo-orbital* Abated by sleep* Resolves spontaneously *Usually

Postdrome • Estimated to affect 90% of migraine sufferers • Phase after pain relief – duration up to 24 hours • Sufferers may experience: hyperaesthesia, mood changes, muscular weakness, fatigue, difficulty in concentrating • Extends period of migraine-related disability Blau 1982

Migraine characteristics that aid diagnosis l Frequent association with menstrual cycle l Characteristic triggers l Paradoxical relationship to sleep l Familial history of migraine l Cognitive impairment with attacks l Dizziness and / or vertigo

Migraine triggers Climate High altitude Hot baths Intense smells Noise External Glare stimuli Travel Fatigue Physical Exercise stresses Smoking Hunger Sleep Sex Chocolate Cheese Alcohol Oral contraceptives Caffeine Dietary Menstruation Hormonal Toothache Systemic Emotional stresses Anxiety Emotion Depression Shock Excitement Stress

Mode of action of triptans Trigeminal sensory afferent nerve fibres Photophobia Phonophobia Neuropeptides Neurokinin A Substance P CGRP Vasodilation extravasation Post-junctional receptor Postjunctional receptor Higher CNS centres PAIN Thalamus Trigeminal ganglion Direct vasoconstriction Nerve activation reduced Peptide release inhibited Decreased pain transmission Postjunctional receptor Trigeminal nucleus Caudalis Autonomic activation Nausea emesis CNS, central nervous system CGRP, calcitonin gene-related peptide Ferrari & Saxena 1993 Goadsby & Hoskin 1996

Trigeminovascular system: Anti-migraine targets PAIN Cortex Higher CNS Centres Phonophobia Photophobia Thalamus TARGET Trigeminal ganglion Autonomic activation Nausea, Emesis Trigeminal nucleus caudalis TARGET Intracranial blood vessels

The triptans • Stronger than sumatriptan 100 mg Rizatriptan, eletriptan • Equal to sumatriptan 100 mg almotriptan, zolmitriptan • Weaker than sumatriptan 100 mg, frovatriptan, naratriptan
 – Cluster headache – Paroxysmal Hemicrania")
Other primary headache • Trigeminal autonomic cephalalgias (TACs) – Cluster headache – Paroxysmal Hemicrania (indometacin) – SUNCT • Hemicrania continua (indometacin) • New daily persistent headache
 Verapamil ( 240 to")
Cluster prophylaxis • • Prednisolone high dose (60 mg daily) Verapamil ( 240 to 720 mg daily) Lithium (600 to 900 mg daily) Methysergide( fibrosis retroperitoneum, pleural pericardial linings)
")
Cluster Acute Rx • • • High flow oxygen (7 – 12 l/ min) Sumatriptan subcutaneously Nasal zolmitriptan Lignocaine nose drops IV dihydroergotamine ( not UK)
- Slides: 40