EXAMINATION OF THE RESPIRATORY SYSTEM EXAMINATION OF THE














,")








")





















 of the thyroid")







 should be")
























- Slides: 100
EXAMINATION OF THE RESPIRATORY SYSTEM
EXAMINATION OF THE RESPIRATORY SYSTEM �The most critical initial question in Pediatrics is whether or not the patient is actually ill. Observation of the patient prior to the actual exam can be tremendously helpful in making this determination.
EXAMINATION OF THE RESPIRATORY SYSTEM �Exam should start with the organ systems requiring the greatest amount of cooperation. �The cardiovascular and pulmonary exam is the least disturbing. The head and neck exam tend to be the most disturbing to the patient and should be more successfully accomplished in the parent’s lap than on a cold exam table.
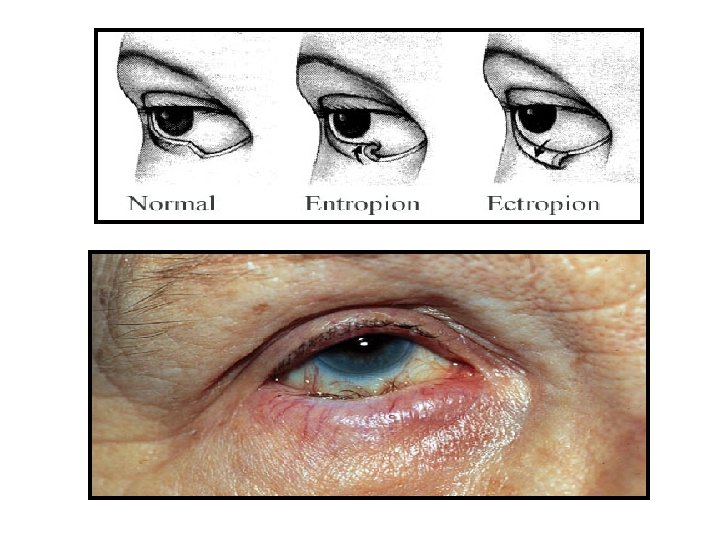
EXAMINATION OF THE RESPIRATORY SYSTEM �EYES: �A bluish discoloration of the lower orbitopalpebral groove is associated with allergic disorders (“allergic shiners”); Dennie’s sign is a prominent fold in the skin seen in patients with environmental allergies. The eyelids may reveal ptosis, entropion, or ectropion.
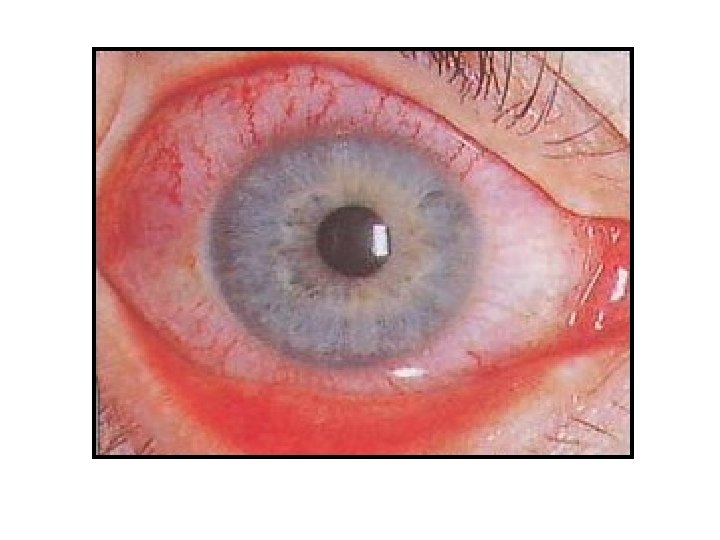
EXAMINATION OF THE RESPIRATORY SYSTEM �The palpebral and bulbar conjunctivae may reveal pallor or injection. Focal subconjunctival hemorrhages are commonly seen in the newborn period. The pattern of injection seen with Kawasaki disease is typically peripheral, in contrast to the pattern seen with iritis, which is commonly perilimbal.
EXAMINATION OF THE RESPIRATORY SYSTEM �Cobblestoning of the palpebral conjunctiva is seen in patients with severe environmental allergies. Any discharge should be noted. Nasolacrimal duct stenosis is the most common nonpathologic cause of eye discharge. The nasolacrimal duct may become inflamed, causing dacryocystitis
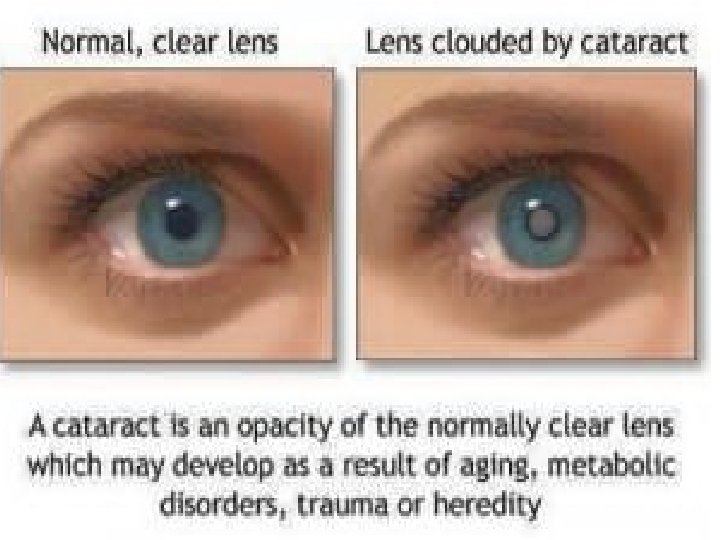
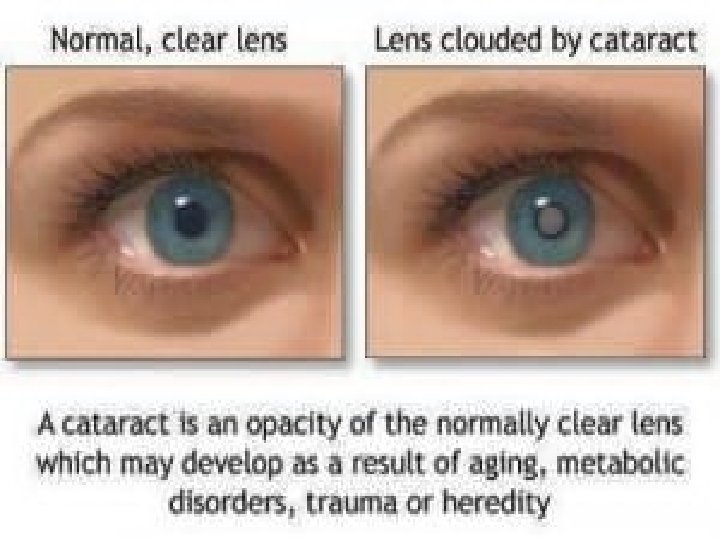
EXAMINATION OF THE RESPIRATORY SYSTEM �A red light reflex should be obtained to look for cataracts, retinoblastoma, retinal detachment, or chorioretinitis. The iris should be examined for a Brushfield spots (a sign often associated with Trisomy 21), a coloboma (a cleft sometimes associated with other syndromes), or Lisch nodules (seen in neurofibromatosis.
nasolacrimal canal duct stenosis
EXAMINATION OF THE RESPIRATORY SYSTEM �Once the child can cooperate (usually around 4 years), a fundoscopic exam should be performed. Increased intracranial pressure is manifest by decreased venous pulsations – blurred disk is a later sign. The macula should also be examined, as abnormalities can be associated with certain neurodegenerative disorders. Corneal clouding can be a sign of glaucoma.
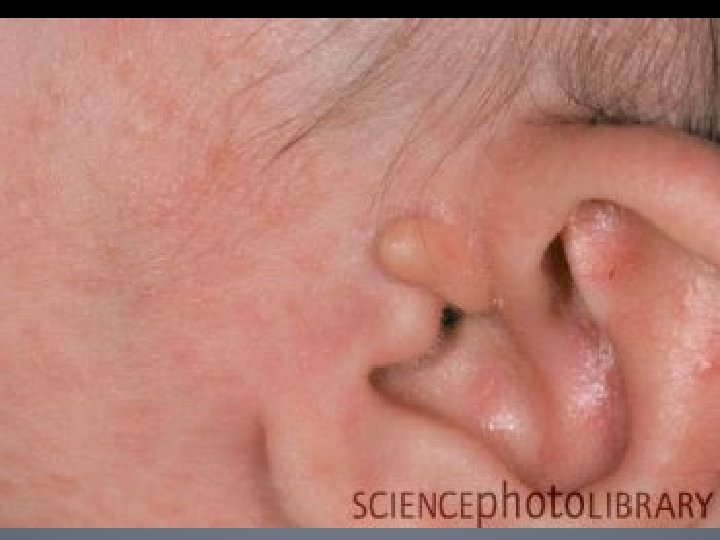
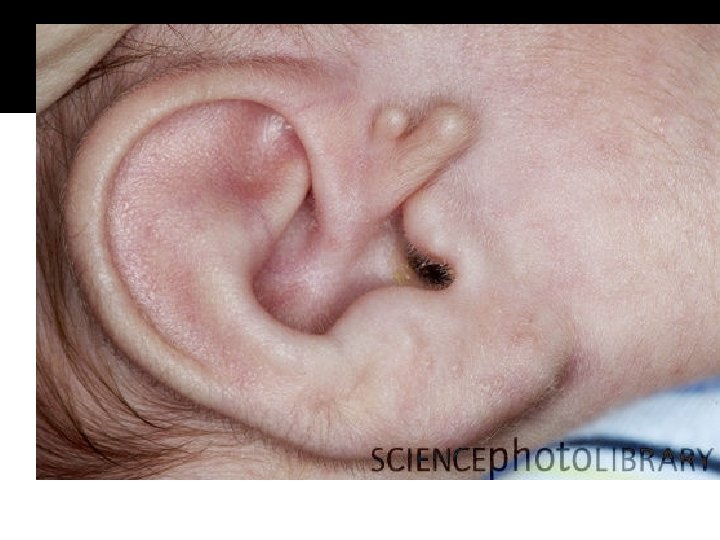
EXAMINATION OF THE RESPIRATORY SYSTEM EARS �The size and any physical aberrations in the shape of the external ear should be noted. Darwin’s tubercles are common. The ears should be set and rotated normally - an abnormality may be an indication of certain syndromes (including Trisomy 21).
EXAMINATION OF THE RESPIRATORY SYSTEM �There are published standards for external ear length ( long external ear is associated with certain syndromes, like Fragile X). Any preauricular pits or skin tags (a remnant of external ear development) should be noted. The pinna may appear to be protruding in the child with mastoditis. The pinna should be manipulated to look for irritation of the skin of the auditory canal, as may be seen with otitis externa.
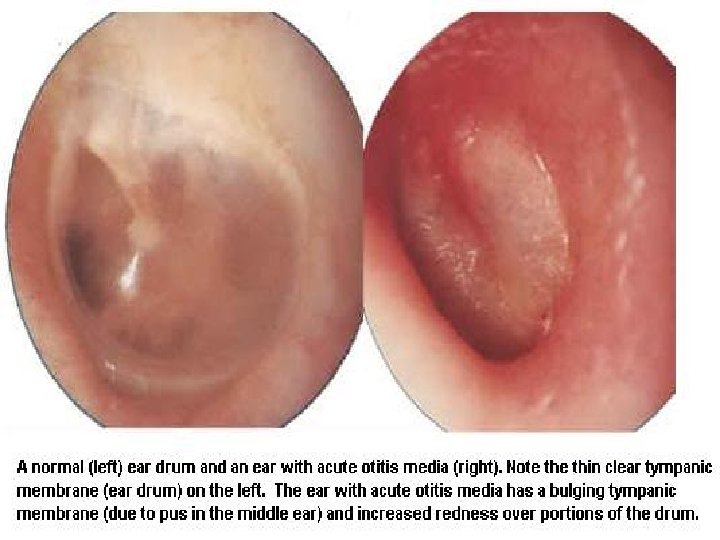
EXAMINATION OF THE RESPIRATORY SYSTEM �The otoscope speculum should be gently inserted into the external auditory canal. The skin in the external auditory canal should resemble normal skin. The tympanic membrane (TM) should be translucent with a normal light reflex and visible landmarks, especially the manubrium of the malleus.
EXAMINATION OF THE RESPIRATORY SYSTEM �Insufflation should be performed. Signs of otitis media include injection of the TM, pus behind the TM, bulging or retraction of the TM, and poor mobility on insufflation. Some fluid behind the TM is commonly seen for weeks to months after episode of otitis media.
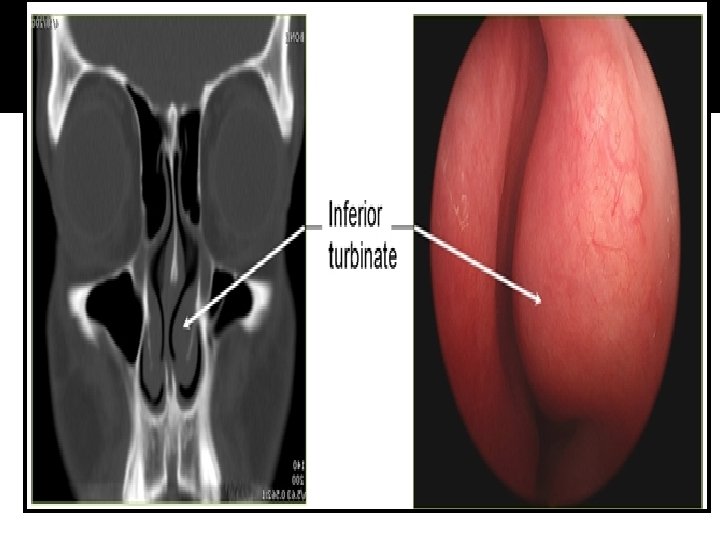
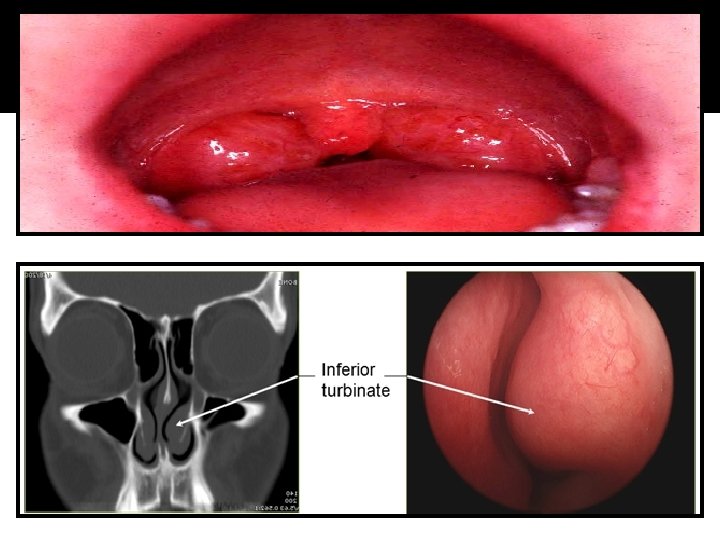
EXAMINATION OF THE RESPIRATORY SYSTEM NOSE: �The shape, size, and symmetry of the nose should be noted. In an older child, the presence of a septal deviation, polyps, injected or boggy mucosa, rhinorrhea or other discharge, and bleeding should be recorded. Nasal polyps can be associated with a variety of etiologies, including allergic rhinitis, cystic fibrosis, and aspirin sensitivity.
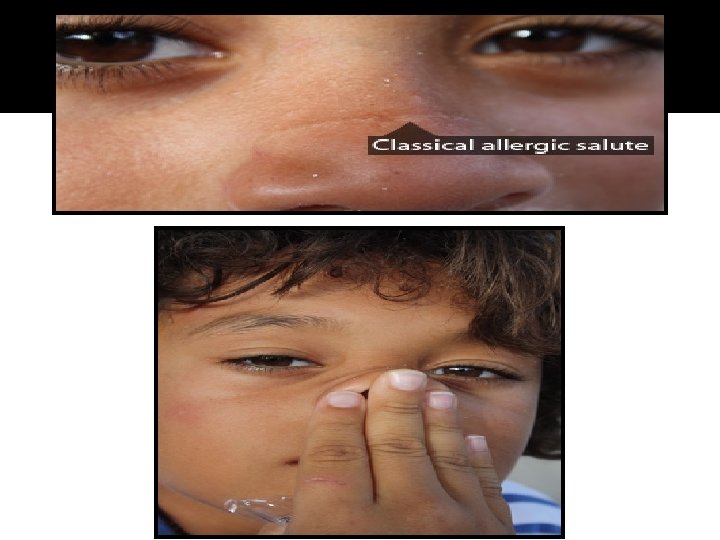
EXAMINATION OF THE RESPIRATORY SYSTEM �Any nasal flaring should be noted in a child with respiratory distress. Tenderness over the sinuses should be noted in patients old enough to have them. �The frontal sinuses do not start development until the middle of childhood. They are not fully pneumatized until adolescence. A horizontal crease may be seen in the skin on the surface of the nose; this signifies repetitive wiping of the nose commonly seen in allergic rhinitis (the “allergic salute”).
EXAMINATION OF THE RESPIRATORY SYSTEM THROAT/MOUTH: �The mouth is usually examined after the ears, since the infant is frequently already crying. The parent can once again restrain the hands or hold an older child facing the examiner while the arms and head are held.
EXAMINATION OF THE RESPIRATORY SYSTEM �Older children (after the age of 3 -4 years) freqeuntly are compliant with this exam. The color of the oropharynx should be noted. Cobblestoning of the posterior pharyngeal wall is a sign of chronic allergic disease. The size of the tonsils and tonsilar pillars and any discharge should be noted.
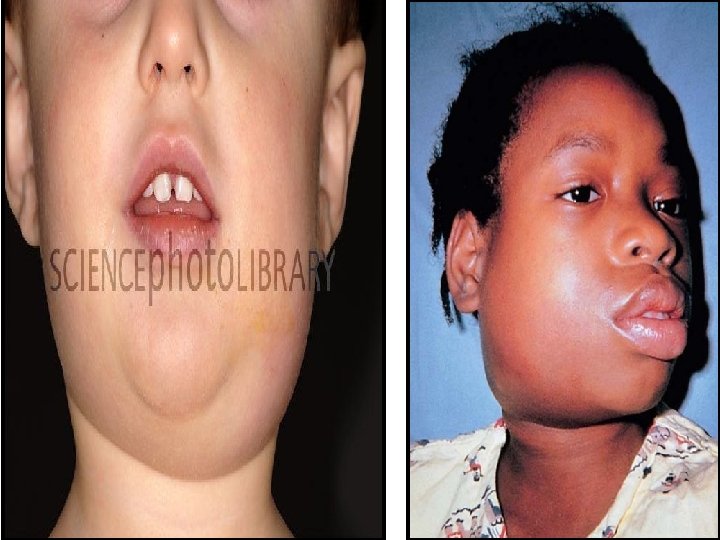
EXAMINATION OF THE RESPIRATORY SYSTEM The soft plate and gingiva in newborns may • have keratin pearls. (also known as Epstein’s pearls). Any cleft palate should be noted. The uvula may be bifid, possibly indicating a submucous cleft. The number of position of teeth should be noted, as delayed or advanced dentition can be caused by some of the same conditions affecting fontanel closure.
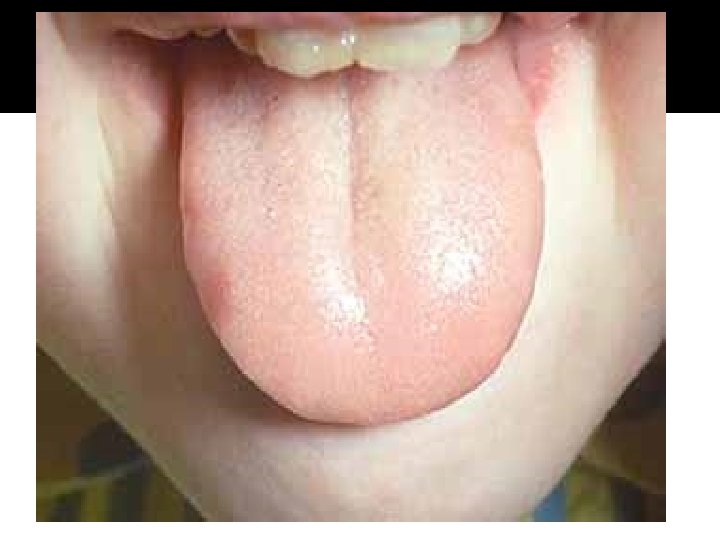
EXAMINATION OF THE RESPIRATORY SYSTEM “Tongue tie” or a shortened • frenulum, is very uncommon. There should be no functional deficits if the infant can protrude the tongue beyond the gingival margin.
EXAMINATION OF THE RESPIRATORY SYSTEM Eruption cysts and mucoceles are not • uncommon in the first 6 months. Any caries should be noted. The teeth should be examined for a malocclusion. Natal teeth may be seen in the newborn period. A single central maxillary incisor can be associated with growth hormone deficiency. Maxillary hyperplasia may be seen with various forms of chronic anemia.
CLINICAL FEATURES These asymptomatic lesions are located along the angle of the mandible if arising from the first branchial cleft and the middle to lower third of the anterior border of the sternocleidomastoid in cases arising from the second branchial cleft. They may present after an upper respiratory infection as a painful mass. These lesions tend to drain internally, but communication with the epidermis can occur. Branchial cysts may become complicated by infection.
EXAMINATION OF THE RESPIRATORY SYSTEM �The quality of the patient’s voice should also be noted. Abnormalities might include a ‘hot potato voice’ seen in a retropharyngeal abscess or hoarseness associated with vocal cord paralysis. The arching of the palate should be noted if abnormal (a high-arched palate may be seen in certain syndromes like Marfan syndrome).
EXAMINATION OF THE RESPIRATORY SYSTEM �Any grunting should be noted for patients in respiratory distress. A large tongue may be seen in certain syndromes (e. g. , Beckwith. Wiedenmann). A geographic tongue is a common finding. A smooth tongue may be seen in vitamin B 12 deficiency. The buccal mucosa may have white reticular plaques commonly seen with thrush.
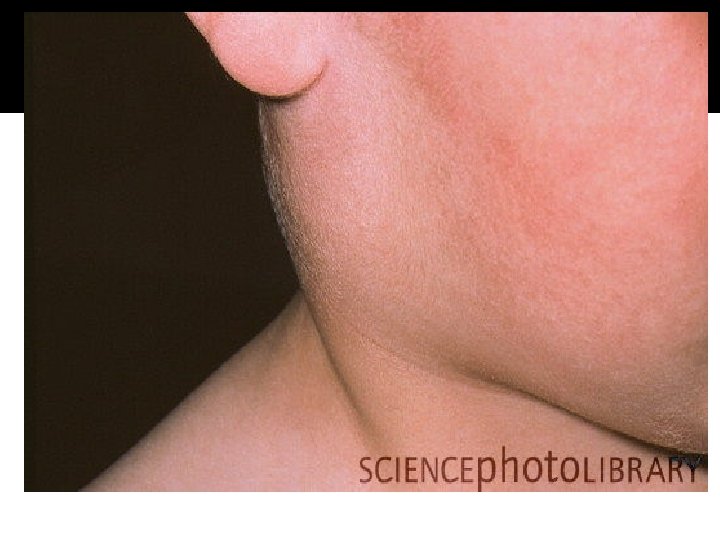
EXAMINATION OF THE RESPIRATORY SYSTEM NECK: �Any masses should be recorded, including their position (anterior vs. lateral) and consistency (firm vs. cystic vs. pulsating). The differential diagnosis of cervical masses is governed, in large part, by these findings.
Accurate diagnosis of neck masses is critical to minimize morbidity and mortality. However, differentials vary greatly and can be challenging for the physician. Neck masses are common presenting complaints, but differential diagnoses vary considerably based on patient age and the location of the neck mass. Most neck masses in the pediatric population have an infectious etiology, whereas an adult neck mass is considered to be a malignancy until proven otherwise. Evaluation of a neck mass depends on the history and physical examination; evaluation may also include observation, antibiotics, fine-needle aspiration, open biopsy, neck dissection, or wide local excision.
Thyroglossal Cyst is an abnormal growth on the neck that looks like a lump. It is the most common type of Nonodontogenic Cyst i. e. it is an oral cyst developing from epithelium which is nested in bony or soft-tissue joints during embryonal development. A Thyroglossal Cyst is also known as a Thyroglossal Duct Cyst or Thyroglossal Tract Cyst.
EXAMINATION OF THE RESPIRATORY SYSTEM �A large cyst in the midline of the Neck is frequently a thyroglossal duct cyst. A tender fluctuant lateral neck mass is frequently an infected anterior cervical lymph noted though a branchial cleft cyst needs to be considered, as well. Cystic hygromas can occur anywhere in the neck but they are usually laterally located.
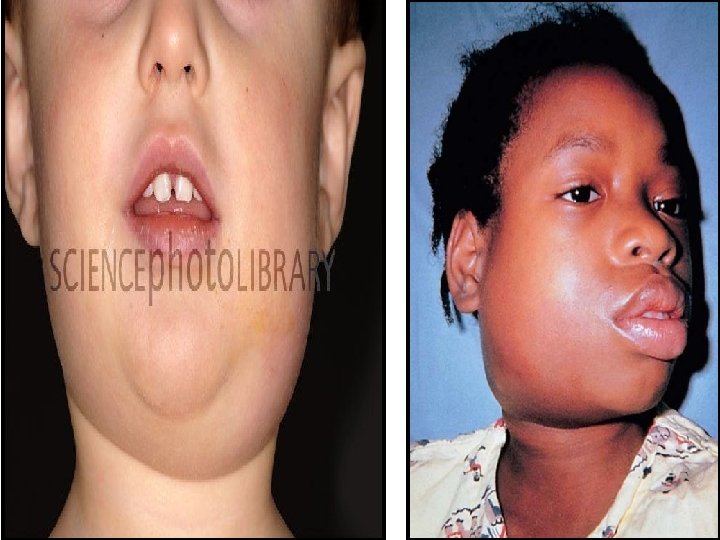
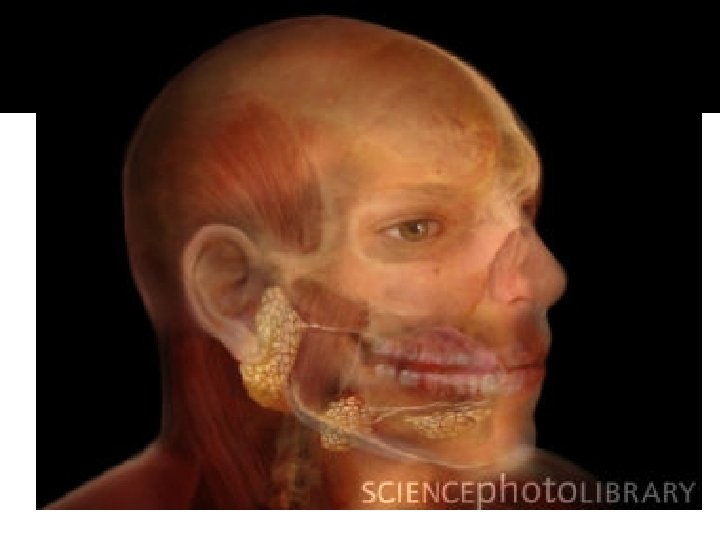
EXAMINATION OF THE RESPIRATORY SYSTEM �An enlarged parotid gland can be differentiated from a cervical node by the fact that the parotid gland is dissected in half by the angle of the mandible while the latter is found below the angle of the mandible. Parotitis, though commonly associated with mumps, is more commonly seen with other common viral infections.
EXAMINATION OF THE RESPIRATORY SYSTEM �The size and nodularity (if any) of the thyroid needs to be noted. A webbed neck may be a sign of turner syndrome. The position of the neck may be important in early infancy, as torticollis has an extensive differential diagnosis. Abnormal neck mobility may be sign of infection (e. g. meningitis or peritonsillar abscess) or trauma. Tracheal tugging or accessory muscle use may be seen with respiratory distress. The salivary glands are rarely enlarged in children.
EXAMINATION OF THE RESPIRATORY SYSTEM CHEST: �The symmetry of the chest should be noted, as should any subcostal/intercostal retractions. Asymmetric expansion may be seen with a pneumothorax or diaphragmatic paralysis. Abnormal shapes (e. g. , pectus excavatum or pectus carinatum) should be noted. Barrelshaped chests are sometimes seen in patients with chronic obstructive pulmonary disease (e. g. , chronic asthma or cystic fibrosis).
EXAMINATION OF THE RESPIRATORY SYSTEM �A rachitic rosary may be seen or palpated in rickets. Widely-spaced nipples may be sign of Turner syndrome. The pubertal development of the breasts (Tanner staging) should be noted in females. Any masses, tenderness, or discharge should be described in detail.
EXAMINATION OF THE RESPIRATORY SYSTEM �Breast buds are commonly seen in neonates. The integrity of the clavicles should be noted in newborns. Males sometimes develop unilateral or bilateral breast hypertrophy during puberty.
EXAMINATION OF THE RESPIRATORY SYSTEM CARDIOVASCULAR: �A bell or diaphragm of the appropriate size should be used. Frequently, an adult stethoscope can be used once the child is out of the immediate newborn period. �The diaphragm should be applied firmly to the chest while the bell should be applied lightly.
EXAMINATION OF THE RESPIRATORY SYSTEM CARDIOVASCULAR: �The PMI (point of maximal impulse) should be noted with respect to location and intensity. A right-sided PMI may be associated with situs inversus (and further imaging of the spleen may be indicated).
EXAMINATION OF THE RESPIRATORY SYSTEM �The difference between a grade III/VI murmur and a Grad IV/VI murmur is palpable thrill felt in Grade IV, radiation to the axillae, neck, or back, and changes with psition. Sinus arrythmia is commonly seen in children, as is a physiologically split S 1. Any rubs, clicks, gallops should be noted.
EXAMINATION OF THE RESPIRATORY SYSTEM �A prominent S 1 is heard with mitral stenosis; a prominent S 2 may be heard with pulmonary hypertension. Innocent heart murmurs are low grade, often heard as a vibratory/musical sound at the apex or left sternal border (Still’s), low grade systolic at the left sternal border (pulmonary flow), or below either clavicle and decreasing with neck movement or supine position (venous hum).
EXAMINATION OF THE RESPIRATORY SYSTEM LUNGS: �A bell or diaphragm of the appropriate size should be used. Frequently, an adult stethoscope can be used once the child is out of the immediate newborn period. The clarity of the breath sounds and the quality of air movement should be noted.
EXAMINATION OF THE RESPIRATORY SYSTEM �Any wheezing, rhonchi, rales, or transmitted upper airway sounds should be recorded. An increased inspiratory: expiratory ratio is an indication of small airways bronchospasm. Since airway sounds are transmitted better through a smaller chest, the exam can be somewhat confusing at times. Fremitus, whispered pectoriloquy, and percussion are more useful in older children and adolescents than in infants and younger children.
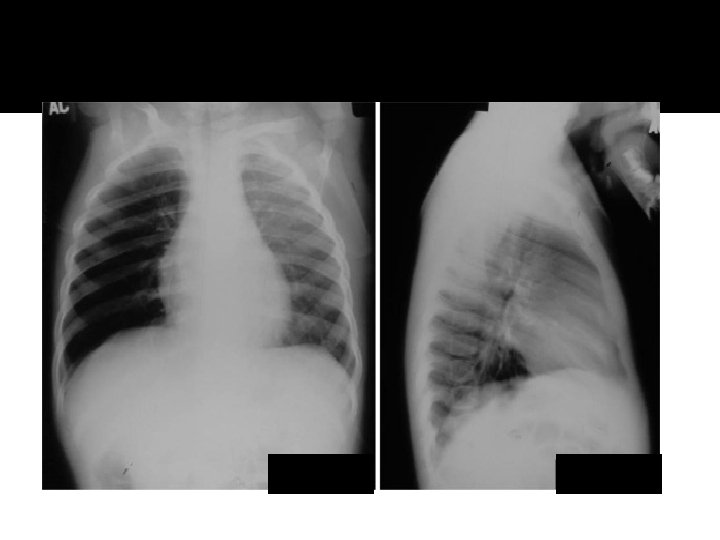
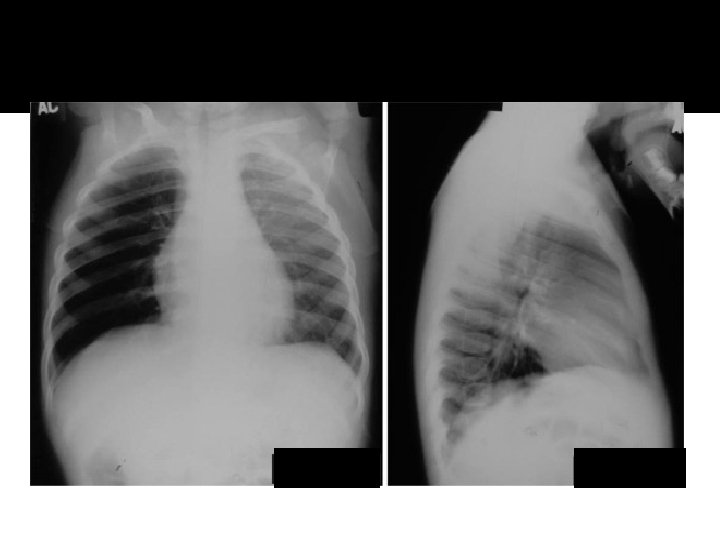
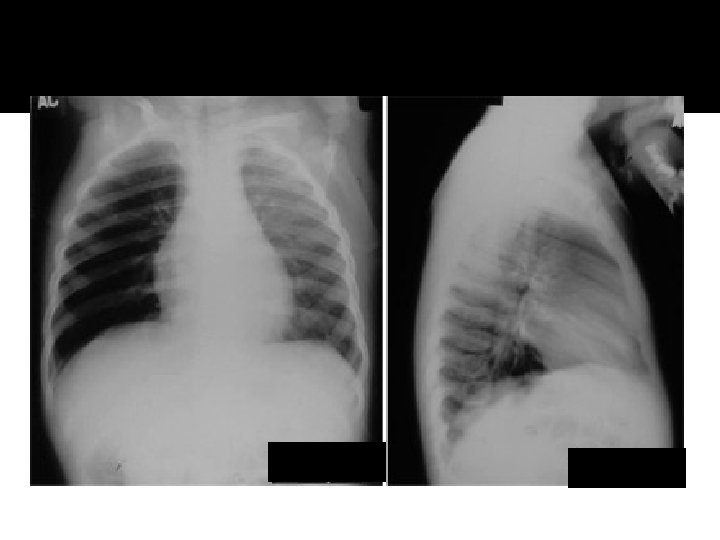
Atelectasis RML
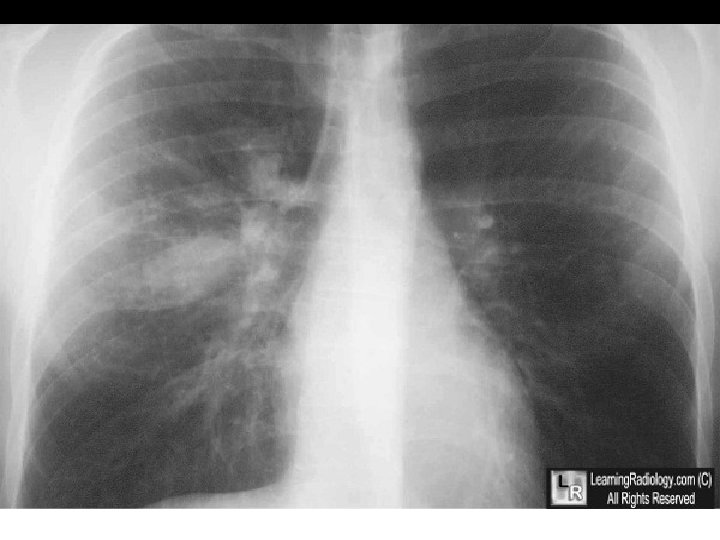
Pneumonia lingula
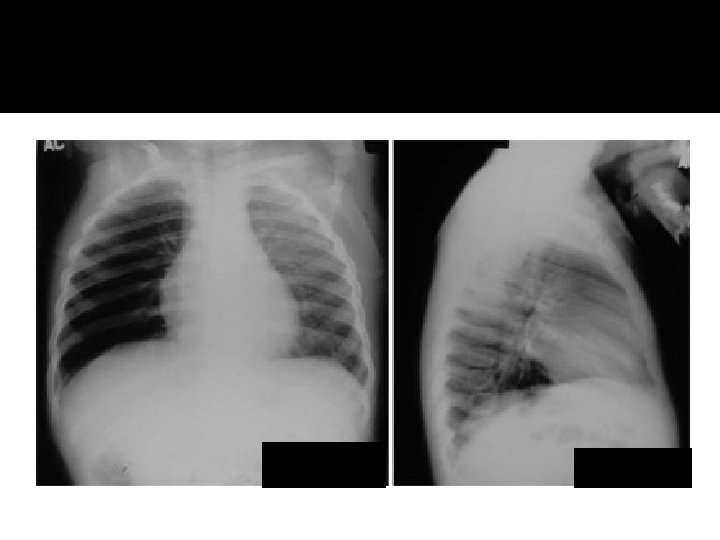
Pneumonia lingula
Atelecasis RML
EXAMINATION OF THE RESPIRATORY SYSTEM SKIN: �Skin lesions should be described using standard dermatologic nomenclature including the size, type, color, and distribution of the lesion, (e. g. , 1 mm red papules in the intertrigenous area of the neck). Primary skin lesions include macules, papules, plaques, nodules, wheals, vesicles, cysts, and pustules.
EXAMINATION OF THE RESPIRATORY SYSTEM �Secondary changes include erosion, oozing, crusting, scaling, atrophy, excoriation, and fissuring. Lesions are arranged in the following manners: discrete, linear, annular, or grouped.
EXAMINATION OF THE RESPIRATORY SYSTEM �Skin turgor and general color should also be noted. Jaundice in a newborn less than 24 hours old and greater than 2 weeks old always needs to be assessed – the possibilities of pathologic jaundice and biliary atresia need to be ruled out respectively.
EXAMINATION OF THE RESPIRATORY SYSTEM �The regularity of the borders of neavi or café au lait spots should be also be noted. The examiner should always be aware of the location of lesions attributed to trauma – the location of these lesions can often aid in determining whether a lesion was accidental. Common findings include hemangiomas and Mongolian spots. As infants usualy do not stand, the skin in dependent areas should be examined for edema.
EXAMINATION OF THE RESPIRATORY SYSTEM IMPRESSION: �A diagnostic impression should be developed. A problem list can be useful for beginners to try to synthesize a patient’s findings into a coherent diagnosis. One useful way to synthesize this information is to first describe the anatomy of each abnormality, then to describe the pathologic process (e. g. , neoplastic, inflammatory, infectious), finally arriving at a coherent diagnosis.
EXAMINATION OF THE RESPIRATORY SYSTEM �The cycle of data collection, hypothesis setting, hypothesis testing, and action is put into place. The selection of a diagnostic pivot, or unique finding, may assist in narrowing down the differential diagnosis.
EXAMINATION OF THE RESPIRATORY SYSTEM �The rules of parsimony, chronology, and plausibility should be remembered. Common diagnostic errors, such as premature closure (i. e. , reaching a conclusion before there is enough data to support it) should be avoided. Common and catastrophic diagnosis are the most important ones to address.
EXAMINATION OF THE RESPIRATORY SYSTEM PLAN: �A diagnostic and therapeutic plan should address each diagnostic impression. Tests should be ordered only if the result will alter the plan. Pediatricians tend to be fairly conservative in prescribing medication, especially for selflimited diseases, such as the common cold. One useful way to delineate a plan is by systems (e. g. , cardiovascular, pulmonary, hematologic, infectious, fluid/electrolytes/nutrition, etc. ).
-----END----PROF. ABDULRAHMAN ALFRAYH