The Respiratory SCE Specialty Certificate Examination Dr Chris
 Dr Chris Atkins – Respiratory Registrar Norfolk and")











 website (SCE")











 Wells AU et al. Interstitial lung disease guideline: The British")






























)-(2. 6/0. 8)) – 12. 4 = (19.")








: S 63–S")








- Slides: 77
The Respiratory SCE (Specialty Certificate Examination) Dr Chris Atkins – Respiratory Registrar Norfolk and Norwich University NHS Foundation Trust August 2016
Overview • Background to the SCE and their remit • Structure of the examination • Examination standards • Pass rates • Resources • Example questions
Background • Introduced in 2008 as a formal test of specialty knowledge • “Rigorous national assessment to establish public confidence” • Developed in partnership with the relevant specialist society in the UK • British Thoracic Society for respiratory medicine • Prerequisite for attainment of CCT – • Represents the breadth and depth of knowledge required of a newly qualified specialist in the chosen discipline • Set as a similar challenge to sub-specialty certification examination in North America • Recommended to be sat in penultimate year of training (ST 6) • Delivered once a year
Dates – 2016 & 2017 Date Registration Period Test centre Results Release Booking Window 26 October 2016 6 July – 28 September 2016 3 August – 29 September 2016 31 May – 23 August 2017 28 June – 24 August 2017 20 September 2017 4 weeks after exam Cost £ 665
Claiming back some of the money Write a letter to HMRC stating that: • you are employed under a training contract (provide a letter from your Deanery/ LETB or your employment contract to support this); • you took (specify) mandatory examination/s run by MRCP(UK) to meet the requirements of your training programme and believe that the cost of the examination/s is now tax deductible; • reference the case of Revenue & Customs Commissioners v Dr Piu Banerjee ([2010] EWCA Civ 843); and HMRC guidance EIM 32546 which states that: ‘Failure to…obtain the qualification will mean that he cannot proceed to the next stage of his chosen profession’. HMRC will require proof of payment for examination fees paid (eg credit card or bank statement).
Exam Structure • 2 x 3 hour papers, 100 questions each • Single best answer format – five options per question • 1 hour break at the mid-point • Undertaken at Pearson VUE • “Driving theory test” centres • Delivery by computer • You will be staring at a computer screen for 6 hours on the day
Question Format • A 30 -year-old man presented to the chest clinic with a chronic productive cough and increasing breathlessness. He gave a history of recurrent chest infections since childhood. He and his partner had recently been referred for fertility treatment. • On examination, he had finger clubbing and scattered crackles throughout both lung fields. • What is the most likely diagnosis? 1. Bronchiectasis 2. Cystic Fibrosis 3. Primary Ciliary Dyskinesia 4. Pulmonary Fibrosis 5. Pulmonary Tuberculosis
Blueprint • Airways disease • Diffuse parenchymal lung disease • Pleural and mediastinal diseases • Pulmonary infections • Pulmonary vascular disease • Sleep-related breathing disorders • Thoracic oncology • Other No. Questions 35 25 25 35 20 • Includes: Critical care, Genetic diseases, Lung transplantation, pharmacology, practical procedures and statistics
Setting standards • Determined by the standard setting group • Review the paper set by the examination board; the board agree on the correct answer • The board estimate what percentage of the “borderline” candidates will pass each question • This creates a calculated mean pass mark pre-examination • This pass mark can be adjusted up or down within the standard deviation of the calculated pass mark taking into account the performance of UK trainees • BTS states they are aiming for >80% pass mark
Resources • Guidelines • Question banks • Meetings/Courses • Books
Resources • Guidelines • Question banks • Meetings/Courses • Books • BTS • NICE • ERS • ATS • ESTS
Resources • Guidelines • Question banks • Meetings/Courses • Books • MRCP(UK) website (SCE page) • BTS e. Learning • Previous questions and mock exams • www. lunglead. com/sce/
Resources • Guidelines • Question banks • Meetings/Courses • Books • Conferences • “Preparing for the Respiratory SCE” • Training days • BTS short courses and e. Learning modules • Includes CPEX slides
Resources • Guidelines • Question banks • Meetings/Courses • Books • Oxford Handbook of Respiratory Medicine • Oxford Desk Reference: Respiratory Medicine • Case Histories in Respiratory Medicine / Sleep Medicine • Revision notes for the Respiratory Medicine SCE
Practice Questions
Question 1 • A 28 year old man presented with episodic cough, dyspnoea and wheeze 18 months after starting work soldering. There was inadequate extraction equipment but he had been provided with a paper mask. He had no prior history of respiratory problems but suffered from seasonal hay fever. • On examination there was generalised expiratory wheeze but no crackles. • What is the most appropriate investigation to confirm a diagnosis of occupational asthma? • • • Analysis of 2 -hourly peak flow readings taken at home and at work Analysis of changes in pre- and post-shift FEV 1 values Baseline spirometry and acute bronchodilator response Bronchial hyper-responsiveness testing Skin-prick tests and specific Ig. E tests
Question 1 • A 28 year old man presented with episodic cough, dyspnoea and wheeze 18 months after starting work soldering. There was inadequate extraction equipment but he had been provided with a paper mask. He had no prior history of respiratory problems but suffered from seasonal hay fever. • On examination there was generalised expiratory wheeze but no crackles. • What is the most appropriate investigation to confirm a diagnosis of occupational asthma? • • • Analysis of 2 -hourly peak flow readings taken at home and at work Analysis of changes in pre- and post-shift FEV 1 values Baseline spirometry and acute bronchodilator response Bronchial hyper-responsiveness testing Skin-prick tests and specific Ig. E tests
Standards of care for occupational asthma: an update. Thorax 2012; 67: 278 -280
Question 2 • A 34 year old male, born in Afghanistan, presents with cough, sputum production, weight loss, and night sweats. CXR shows bilateral upper zone cavitation and consolidation. Sputum is AAFB+++ and initial gene probes show that the organism is M. tuberculosis with mutations consistent with the presence of rifampicin and isoniazid resistance. • What should you do? • Start standard quadruple anti-TB therapy and await culture and antibiotic sensitivities before changing treatment • Await culture and sensitivities before starting treatment • Start standard quadruple TB treatment and add moxifloxacin • Presume this is MDR-TB and start a WHO 6 drug regimen • Start pyrazinamide and ethambutol with two additional second-line anti-TB drugs
Question 2 • A 34 year old male, born in Afghanistan, presents with cough, sputum production, weight loss, and night sweats. CXR shows bilateral upper zone cavitation and consolidation. Sputum is AAFB+++ and initial gene probes show that the organism is M. tuberculosis with mutations consistent with the presence of rifampicin and isoniazid resistance. • What should you do? • Start standard quadruple anti-TB therapy and await culture and antibiotic sensitivities before changing treatment • Await culture and sensitivities before starting treatment • Start standard quadruple TB treatment and add moxifloxacin • Presume this is MDR-TB and start a WHO 6 drug regimen • Start pyrazinamide and ethambutol with two additional second-line anti-TB drugs
MDR-TB TB that is resistant to at least Isoniazid and Rifampicin Tuberculosis – NICE Guideline, January 2016
Question 3 • A 55 year old female with a 1 -year history of cough and breathlessness has investigations which reveal ILD. A thoracoscopic lung biopsy shows lymphoid interstitial pneumonia. • What is the most likely cause of her lung disease? • • • HIV Idiopathic Smoking Occult neoplasia Sjogren’s syndrome
Question 3 • A 55 year old female with a 1 -year history of cough and breathlessness has investigations which reveal ILD. A thoracoscopic lung biopsy shows lymphoid interstitial pneumonia. • What is the most likely cause of her lung disease? • • • HIV Idiopathic Smoking Occult neoplasia Sjogren’s syndrome
Lymphoid Interstitial Pneumonia (LIP) Wells AU et al. Interstitial lung disease guideline: The British Thoracic Sciety in collaboration with the Thoracic Society of Australia and New Zealand the Irish Thoracic Society. Thorax 2008; 63: v 1 -v 58
Question 4 • A 52 -year old man presented with recent onset vomiting and a CXR was performed to look for evidence of perforation. • What is the most likely cause of this CXR appearance? • • • Pneumonia Metastatic carcinoma Perforated duodenal ulcer Hamartoma Pulmonary contusion
Question 4 • A 52 -year old man presented with recent onset vomiting and a CXR was performed to look for evidence of perforation. • What is the most likely cause of this CXR appearance? • • • Pneumonia Metastatic carcinoma Perforated duodenal ulcer Hamartoma Pulmonary contusion
Rib metastasis
Question 5 • 32 F, keen athlete and personal trainer. Referred as she finds herself more out of breath when training than previously. History of mild asthma during childhood. A CPET is organised • • • Max ventilation Max HR RR before exercise Resp pattern during exercise VO 2 max O 2 pulse 75% predicted max. 119% predicted max. 18 BPM Steady rise 70% predicted 75% predicted • What is the most likely cause of her symptoms? • • • Asthma Obesity Anxiety Age related decline Heart disease
Question 5 • 32 F, keen athlete and personal trainer. Referred as she finds herself more out of breath when training than previously. History of mild asthma during childhood. A CPET is organised • • • Max ventilation Max HR RR before exercise Resp pattern during exercise VO 2 max O 2 pulse 75% predicted max. 119% predicted max. 18 BPM Steady rise 70% predicted 75% predicted • What is the most likely cause of her symptoms? • • • Asthma Obesity Anxiety Age related decline Heart disease
Introduction to cardiopulmonary exercise testing 2 nd Edition – Luks, Glenny, Robinson
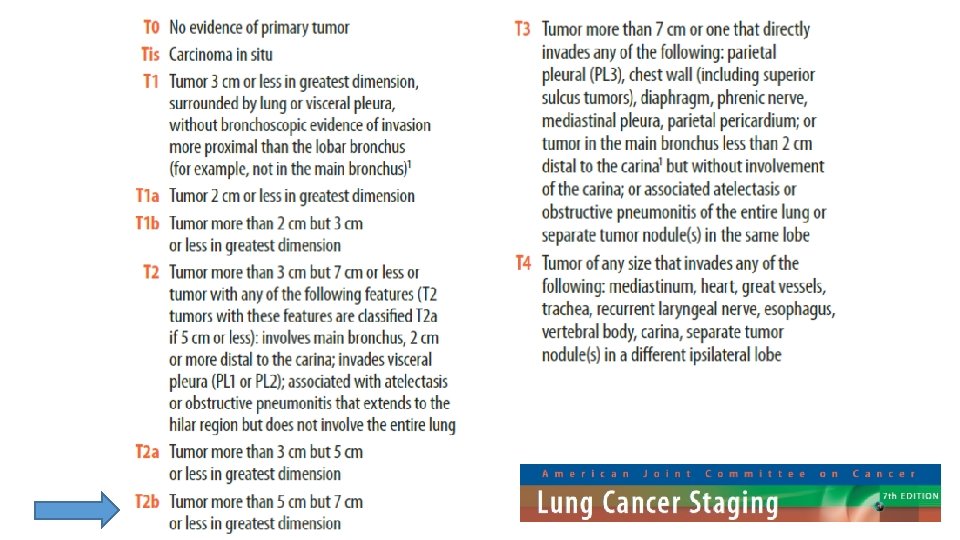
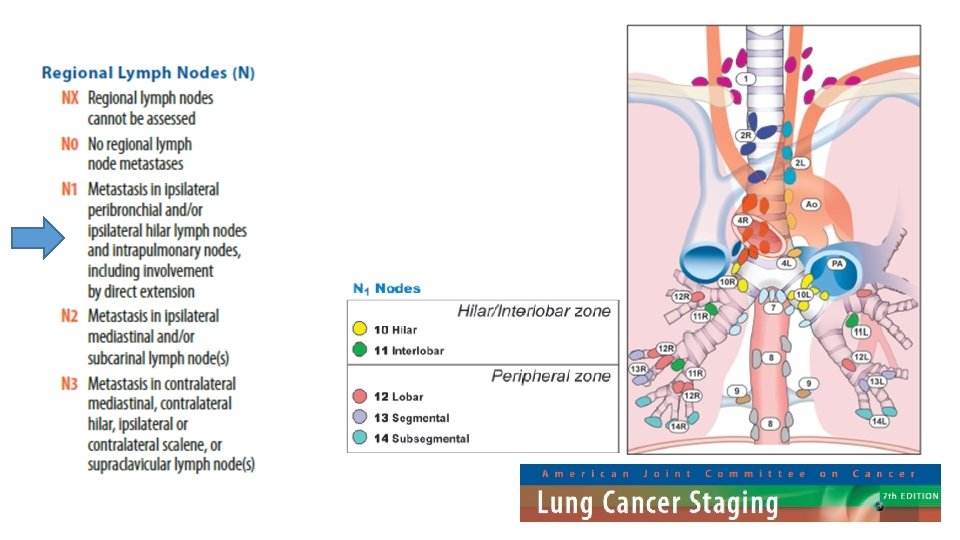
Question 6 • A 72 year old man with a 3 month history of cough is investigated in clinic for suspected lung cancer. He undergoes a CT scan which reveals a 7 cm mass in the right upper lobe (not invading other structures) with enlarged station 10 and 11 lymph nodes. No pleural effusion or distant metastases are seen. • What is his TNM staging based on this CT? • • • T 3 N 2 M 0 T 3 N 1 M 0 T 2 b N 2 M 0 T 2 a N 1 M 0
Question 6 • A 72 year old man with a 3 month history of cough is investigated in clinic for suspected lung cancer. He undergoes a CT scan which reveals a 7 cm mass in the right upper lobe (no pleural involvement) with enlarged ipsilateral station 10 and 11 lymph nodes. No pleural effusion or distant metastases are seen. • What is his TNM staging based on this CT? • • • T 3 N 2 M 0 T 3 N 1 M 0 T 2 b N 2 M 0 T 2 a N 1 M 0
Question 7 • A 68 year old man with known emphysema attends clinic for worsening dyspnoea despite maximal medical therapy. • Which of the following features precludes him from receiving lung volume reduction surgery? • • • Pulmonary hypertension FEV 1 25% predicted Transfer factor 25% predicted Upper lobe predominant emphysema Pa. C 02 7. 1 k. Pa on air
Question 7 • A 68 year old man with known emphysema attends clinic for worsening dyspnoea despite maximal medical therapy. • Which of the following features precludes him from receiving lung volume reduction surgery? • • • Pulmonary hypertension FEV 1 25% predicted Transfer factor 25% predicted Upper lobe predominant emphysema Pa. C 02 7. 1 k. Pa on air
Managing Stable COPD: Chronic Obstructive Pulmonary Disease pathway. NICE 2016
Question 8 • A 70 year old man with a 50 pack-year smoking history is diagnosed with T 1 b. N 0 M 0 lung cancer (squamous) following CT, CT-PET and percutaneous biopsy. He also has mild centrilobular emphysema. He is considered suitable for radical treatment. His lung function tests show: • • FEV 1 92% predicted DLCO 70% predicted TLC 105% predicted RV 118% predicted • Regarding thoracic surgery, which of the following are true? • He is fit for resection up to pneumonectomy without further investigation • He is fit for resection up to lobectomy without further investigation • He requires exercise testing to confirm suitability; if his VO 2 max is >20 ml/kg/min he will require split function to determine suitability • He requires exercise testing to confirm suitability; if his VO 2 max is >20 ml/min/kg he is fit for resection up to pneumonectomy • He is not fit for thoracic surgery and should be referred for alternative therapy
Question 8 • A 70 year old man with a 50 pack-year smoking history is diagnosed with T 1 b. N 0 M 0 lung cancer (squamous) following CT, CT-PET and percutaneous biopsy. He also has mild centrilobular emphysema. He is considered suitable for radical treatment. His lung function tests show: • • FEV 1 92% predicted DLCO 70% predicted TLC 105% predicted RV 118% predicted • Regarding thoracic surgery, which of the following are true? • He is fit for resection up to pneumonectomy without further investigation • He is fit for resection up to lobectomy without further investigation • He requires exercise testing to confirm suitability; if his VO 2 max is >20 ml/kg/min he will require split function to determine suitability • He requires exercise testing to confirm suitability; if his VO 2 max is >20 ml/min/kg he is fit for resection up to pneumonectomy • He is not fit for thoracic surgery and should be referred for alternative therapy
FEV 1 92% predicted DLCO 70% predicted TLC 105% predicted RV 118% predicted ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients. ERS 2009.
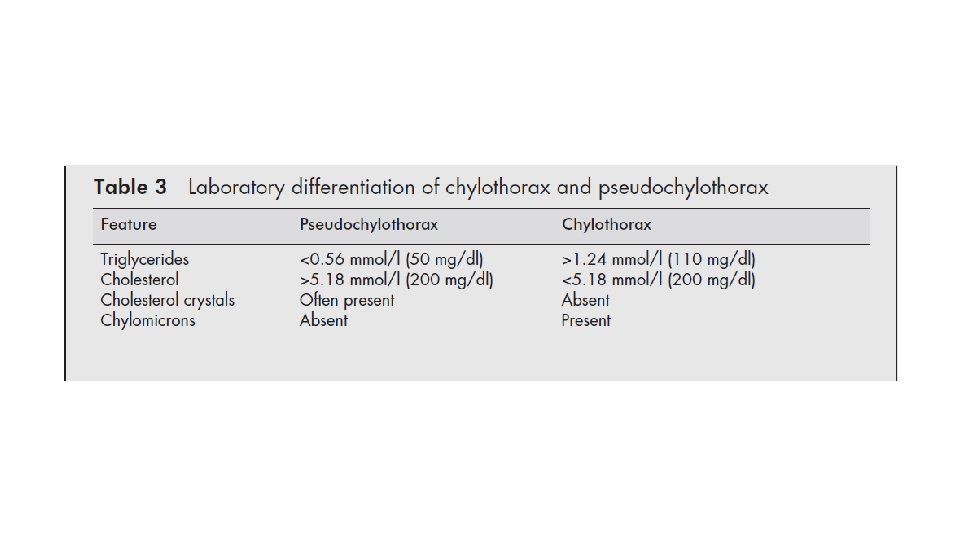
Question 9 • 47 year old female, referred with increasing dyspnoea. She has moderately severe RA and takes methotrexate. She has a moderate right side effusion. The effusion and tapped and confirms a pseudochylous effusion. • Which substance, present in pleural fluid in high levels, is most likely to denote a pseudochylothorax? • • • Amylase Cholesterol Chylomicrons HDL Triglyceride
Question 9 • 47 year old female, referred with increasing dyspnoea. She has moderately severe RA and takes methotrexate. She has a moderate right side effusion. The effusion and tapped and confirms a pseudochylous effusion. • Which substance, present in pleural fluid in high levels, is most likely to denote a pseudochylothorax? • • • Amylase Cholesterol Chylomicrons HDL Triglyceride
Question 10 • Pulmonary hypertension is defined as a mean pulmonary artery pressure of: • • • At least 15 mm. Hg At least 20 mm. Hg Greater than 20 mm. Hg At least 25 mm. Hg Greater than 25 mm. Hg
Question 10 • Pulmonary hypertension is defined as a mean pulmonary artery pressure of: • • • At least 15 mm. Hg At least 20 mm. Hg Greater than 20 mm. Hg At least 25 mm. Hg Greater than 25 mm. Hg
Pulmonary Hypertension ESC/ERS PAH Guidelines
Question 11 • A 47 -year old woman has 9 month history of exertional dyspnoea and blackouts. She is WHO FC IV. She has a loud P 2 and peripheral oedema to the knees. • CT scan – no PE, hypertrophied RV. • • • RHC Mean arterial pressure Mean RAP Mean Pulmonary art. Pressure Mean PCWP Mean CO Rest 85 mm. Hg 18 mm. Hg 51 mm. Hg 10 mm. Hg 2. 9 L/min • What is the most appropriate initial treatment? • • • Calcium channel blocker Endothelin receptor antagonist Guanylate Cyclase Inhibitor Phosphodiesterase inhibitor Prostanoid Inhaled NO 83 mm. Hg 19 mm. Hg 48 mm. Hg 11 mm. Hg 3. 0 L/min (96) (3) (15) (9) (5)
Question 11 • A 47 -year old woman has 9 month history of exertional dyspnoea and blackouts. She is WHO FC IV. She has a loud P 2 and peripheral oedema to the knees. • CT scan – no PE, hypertrophied RV. • • • RHC Mean arterial pressure Mean RAP Mean Pulmonary art. Pressure Mean PCWP Mean CO Rest 85 mm. Hg 18 mm. Hg 51 mm. Hg 10 mm. Hg 2. 9 L/min • What is the most appropriate initial treatment? • • • Calcium channel blocker Endothelin receptor antagonist Guanylate Cyclase Inhibitor Phosphodiesterase inhibitor Prostanoid Inhaled NO 83 mm. Hg 19 mm. Hg 48 mm. Hg 11 mm. Hg 3. 0 L/min (96) (3) (15) (9) (5)
ESC/ERS PAH Guidelines
Question 13 • Which of the following medical conditions has the highest prevalence of pulmonary arterial hypertension? • • • HIV infection Systemic sclerosis Portal hypertension Systemic Lupus Erythematosis Sarcoidosis
Question 13 • Which of the following medical conditions has the highest prevalence of pulmonary arterial hypertension? • • • HIV infection Systemic sclerosis Portal hypertension Systemic Lupus Erythematosis Sarcoidosis
CTD and PAH • Prevalence of PAH within conditions: • • • SSc – 7 -29% of sufferers HIV – 0. 5% Portal hypertension – 2 -5% Sarcoidosis – unclear, <5% SLE – 0. 005 -14%
Question 14 • During normal ventilation at rest in a healthy individual, which of the following statements is correct? • • • V/Q is lower in the lower zones than the upper zones Perfusion (Q) is lower in the lower zones than in the upper zones Ventilation (V) is essentially even throughout the lungs V/Q is optimal where V is greatest V/Q is the same in the upper and lower zones
Question 14 • During normal ventilation at rest in a healthy individual, which of the following statements is correct? • • • V/Q is lower in the lower zones than the upper zones Perfusion (Q) is lower in the lower zones than in the upper zones Ventilation (V) is essentially even throughout the lungs V/Q is optimal where V is greatest V/Q is the same in the upper and lower zones
V/Q
Question 15 • A 35 -year old nurse who works in your hospital is admitted with a 4 hour history of breathlessness. She does not smoke. On examination she appears anxious. • Pulse 110 bpm, BP 131/85, RR 36 breaths/min • ABG: • p. H 7. 53 Pa. CO 2 2. 6 • The most likely diagnosis is: • • • Pa. O 2 12. 4 Asthma Anxiety leading to hyperventilation Pulmonary Embolism Salicylate overdose Amphetamine use HCO 3 19
Question 15 • A 35 -year old nurse who works in your hospital is admitted with a 4 hour history of breathlessness. She does not smoke. On examination she appears anxious. • Pulse 110 bpm, BP 131/85, RR 36 breaths/min • ABG: • p. H 7. 53 Pa. CO 2 2. 6 • The most likely diagnosis is: • • • Pa. O 2 12. 4 Asthma Anxiety leading to hyperventilation Pulmonary Embolism Salicylate overdose Amphetamine use HCO 3 19
A-a gradient = ((0. 21*(101 -6. 25))-(2. 6/0. 8)) – 12. 4 = (19. 9 3. 25) – 12. 4 = 16. 65 – 12. 4 = 4. 25 k. Pa (A-a gradient) Expected A-a gradient: Young person = 5 -10 mm. Hg (= 0. 66 k. Pa – 1. 33 k. Pa) Add 1 mm. Hg (0. 13 k. Pa) for each decade of life = 1. 73 k. Pa expected gradient
Question 16 • A 19 -year old student, born in India, presented with a 3 -week headache. He was missing college and sleeping more than usual. A lumbar puncture showed lymphocytes but was negative for TB. • What is the most appropriate treatment plan? • • • 2 RHZE 4 RH and Prednisolone 60 mg 2 RHZE 10 RH and Prednisolone 60 mg 2 RHZ 4 RH 2 RHZE 16 RH
Question 16 • A 19 -year old student, born in India, presented with a 3 -week headache. He was missing college and sleeping more than usual. A lumbar puncture showed lymphocytes but was negative for TB. • What is the most appropriate treatment plan? • • • 2 RHZE 4 RH and Prednisolone 60 mg 2 RHZE 10 RH and Prednisolone 60 mg 2 RHZ 4 RH 2 RHZE 16 RH
CNS TB Tuberculosis – NICE Guideline, January 2016
Question 17 • A 65 year old man is admitted with community-acquired pneumonia. Admission features include: • • Normal mental state BP 100/60 RR 30 Blood urea 7 mmol/L • What is his CURB-65 score? • • • 0 1 2 3 4
Question 17 • A 65 year old man is admitted with community-acquired pneumonia. Admission features include: • • Normal mental state BP 100/60 RR 30 Blood urea 7 mmol/L • What is his CURB-65 score? • • • 0 1 2 3 4
CURB-65 • CURB 65 score is calculated by giving 1 point for each of the following prognostic features: • confusion (abbreviated Mental Test score 8 or less, or new disorientation in person, place or time) • raised blood urea nitrogen (over 7 mmol/litre) • raised respiratory rate (30 breaths per minute or more) • low blood pressure (diastolic 60 mm. Hg or less, or systolic less than 90 mm. Hg) • age 65 years or more. • Patients are stratified for risk of death as follows: • 0 or 1: low risk (<3% mortality risk) • 2: intermediate risk (3‑ 15% mortality risk) • 3 to 5: high risk (>15% mortality risk). Lim WS, van der Eerden MM, Laing R, et al. (2003) Defining community‑acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 58: 377– 82
Question 18 • Following a standard treatment duration of anticoagulation for a first venous thromboembolism the risk of recurrence in the first 2 years following an unprovoked or idiopathic PE is estimated at: • • • <5% 5 -10% 15 -20% 30 -40% >50%
Question 18 • Following a standard treatment duration of anticoagulation for a first venous thromboembolism the risk of recurrence in the first 2 years following an unprovoked or idiopathic PE is estimated at: • • • <5% 5 -10% 15 -20% 30 -40% >50%
Cumulative risk of recurrent VTE Am J Hematol. 2012 May; 87(Suppl 1): S 63–S 67.
Question 19 • A 68 year old with emphysema asks about fitness to fly to the Canary islands on a commercial flight. He has emphysema (FEV 1 28%) but can walk 250 yards at his own pace, has no home oxygen and does not have pulmonary hypertension. Resting Pa. O 2 on room air in clinic is 7. 8 k. Pa. • He undergoes a hypoxic challenge test - after Fi. O 2 0. 15 for 20 minutes his Pa. O 2 is 6. 9 k. Pa (87%) • Regarding fitness to fly: • • • He is safe to fly without oxygen but only if the flight is less than 4 hours He is safe to fly with oxygen at 1 L/min He is safe to fly with oxygen at 2 L/min He is not safe to fly, even with oxygen
Question 19 • A 68 year old with emphysema asks about fitness to fly to the Canary islands on a commercial flight. He has emphysema (FEV 1 28%) but can walk 250 yards at his own pace, has no home oxygen and does not have pulmonary hypertension. Resting Pa. O 2 on room air in clinic is 7. 8 k. Pa. • He undergoes a hypoxic challenge test - after Fi. O 2 0. 15 for 20 minutes his Pa. O 2 is 6. 9 k. Pa (87%) • Regarding fitness to fly: • • • He is safe to fly without oxygen but only if the flight is less than 4 hours He is safe to fly with oxygen at 1 L/min He is safe to fly with oxygen at 2 L/min He is not safe to fly, even with oxygen
Fitness to Fly Managing passengers with stable respiratory disease planning air travel: British Thoracic Society recommendations, 2011
Question 20 • A 45 -year old man recently moved to the area comes to clinic with persistent non-productive cough. There is no previous imaging or notes. • What is the most likely diagnosis? • • • Cystic fibrosis Sarcoidosis Previous treated lymphoma Extrinsic allergic alveolitis Silicosis
Question 20 • A 45 -year old man recently moved to the area comes to clinic with persistent non-productive cough. There is no previous imaging or notes. • What is the most likely diagnosis? • • • Cystic fibrosis Sarcoidosis Previous treated lymphoma Extrinsic allergic alveolitis Silicosis
Question 21 • A 40 year old man presents with increasing breathlessness over 1 year. • What is the most likely diagnosis? • • • Alpha-1 antitrypsin deficiency Histiocytosis X Cystic bronchiectasis Centrilobular emphysema Pulmonary sequestration
Question 21 • A 38 year old man presents with increasing breathlessness over 1 year. • What is the most likely diagnosis? • • • Alpha-1 antitrypsin deficiency Histiocytosis X Cystic bronchiectasis Centrilobular emphysema Pulmonary sequestration
Suggestions • Familiarise yourself with the guidelines – don’t leave it until the last minute • If you can, take some study leave before the exam • Study with others • Try questions, visit the BTS e. Learning resources • Claim back the money!