Examination and Assessment of the Neonatal and of















 §Respiratory function §Rate (40 – 60/min) §Rhythm – periodic breathing")

 §Auscultation §Chest radiography")



 §Chest and cardiovascular system §Heart rate §Cardiac sounds §Pulses §Blood")




 §Head and neck § Nares § Mouth §Lips §Oral cavity")
 §Musculoskeletal system, spine, and extremities §Dysmorphic §Number of digits §Abnormal")





 §Infection §Leukopenia (< 3, 500/mm 3) §Leukocytosis (> 25, 000/mm")


 §Chief complaint §Current signs and symptoms")







 and tactile fremitus §Position of trachea")








- Slides: 55
Examination and Assessment of the Neonatal and of the Pediatric Patient Module D Walsh: Chapter 4
Objectives § Describe the factors that most influence neonatal outcome. § List criteria for determining whether an infant is large for gestational age, appropriate for gestational age, or small for gestational age. § List critical vital signs with normal values to be evaluated as part of the newborn's initial physical examination. § Describe criteria for determining whether an infant is displaying apneic spells. § Identify signs and symptoms of respiratory distress in the newborn. § Describe the technique for rapid identification of a pneumothorax in a newborn. § List the possible cardiovascular anomalies associated with different patterns of abnormal pulses. § List the elements of a normal abdominal examination and the significance of abnormal findings. § List the three types of scalp swelling observed in newborns and the characteristics and significance of each type. § List the most common structural abnormalities observed in the nose, lips, mouth, and oral cavity. § Describe the signs and symptoms of the most common types of birth injuries. § List the elements of a basic neurologic examination in the newborn. § Describe the signs and symptoms suggesting the presence of sepsis in the newborn. § List the laboratory tests most commonly done on the newborn and the range of normal values for each. § Identify and use historical and physical findings to develop a differential diagnosis of a child's respiratory condition. § Determine the severity of a child's respiratory condition. § Communicate important historical and physical findings concerning a child's respiratory condition to the health care team in a timely manner. § Assist in planning and executing evaluation and management of the pediatric patient.
Apnea of Prematurity § Defined as a cessation of breathing effort greater than 20 seconds in duration or any pause that is long enough for signs of bradycardia or cyanosis, or both, to appear in an infant younger than 37 weeks gestation. § Different than “periodic breathing”. § The most common form of infant apnea. § Not a disease, per se. Rather it is an immaturity of respiratory control system. § Significant cause of neonatal mortality & morbidity. § Associated with bradycardia and oxygen desaturation § Related to the degree of immaturity and often is a response to hypoxia and asphyxia. § Treatment includes methylxanthines, CPAP, and possibly CNS stimulants (doxapram)
Apnea of Prematurity § Two Types: § Primary Apnea § Occurs as an initial response to hypoxia. § Reduction in heart rate and, to a lesser extent, blood pressure. § Responds well to stimulation. § Secondary Apnea § Occurs as a result of continued hypoxia. § Weak, gasping respirations. § Positive-pressure ventilation MUST be initiated. § Heart rate and blood pressure will fall and death will ensue if not treated quickly. § Apnea may occur in utero, and baby may be born in secondary apnea. ASSUME if apneic at birth.
Primary and Secondary Apnea
Examination of the Neonatal Patient
Gestational Age Assessment
Gestational Age Assessment §Most reliable when done within first 12 hours. §Weight based estimates of age are unreliable as all children don’t “grow” at the same rate in utero. §Dubowitz (1970) § 11 physical signs and 10 neurological signs. § Each assessed and given a score of 1 to 5. § Accurate within 2 weeks. §Ballard (1979) § Modification of Dubowitz. § Accurate between 22 and 44 weeks.
Ballard Scale • Fig. 4 -1, p. 44
Birth Size • Gestational age, weight, length, and head circumference can be plotted on a grid. • Less than 10 th percentile – SGA • Greater than 90 th percentile - LGA • Fig. 4 -4, p. 45
Physical Examination §Vital Signs determined by both the gestational age and by the activity of the child. • Table 4 -2, p. 45 • MBP= Gestational Age (weeks) +5
Common Dermal Findings §Vernix caseosa: § White cream cheese-like material that covers fetus. § Appears at 20 -24 weeks § Remains thick until 36 weeks § Disappears by 41 -42 weeks §Lanugo § Fine, downy hair that covers the fetal body § Appears at 26 weeks. § Thins and disappears by week 32.
Common Dermal Findings §Skin Maturity § 25 to 26 weeks – gelatinous and transparent (visible vessels)
Jaundice § Definition: Yellowish-orange skin color that accompanies increased levels of bilirubin in the blood. § aka hyperbilirubinemia. § Occurs due to the breakdown of old erythrocytes. § Eliminated by the intestinal tract or kidneys. § Bilirubin levels greater than 4 -6 mg/d. L will cause jaundice. § 25 to 50% of all term neonates have jaundice. § Quicker breakdown of erythrocytes in neonates. § Liver can’t handle the load.
Jaundice: Complications & Treatment §Kernicterus: Hyperbilirubinemia related encephalopathy. §Can lead to neurological deficits. §Treatment §Phototherapy lights (“bili lights”) §Exchange Transfusion
Physical Examination (cont. ) §Respiratory function §Rate (40 – 60/min) §Rhythm – periodic breathing §Silverman score §Respiratory Distress § Nasal flaring § Expiratory grunting § Retractions
Silverman Score • Fig. 4 -7, p. 48
Physical Examination (cont. ) §Auscultation §Chest radiography
Physical Examination §Chest and cardiovascular system §Chest configuration §Pectus carinatum & pectus excavatum §Point of maximal cardiac impulse (PMI) §Transillumination (pneumothorax)
Physical Examination (cont. ) §Chest and cardiovascular system §Heart rate §Cardiac sounds §Pulses §Blood pressure §Pulse oximetry §Pre- and postductal
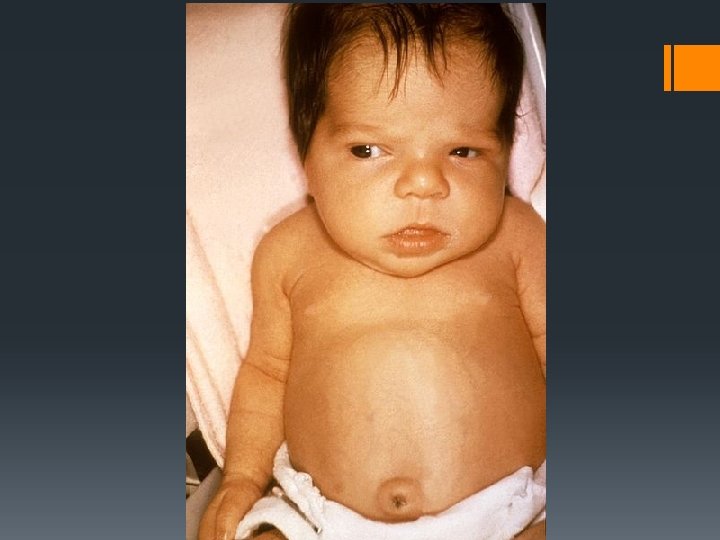
Physical Assessment §Abdomen §Contour §Obvious abdominal wall anomalies §Scaphoid §Auscultation and palpation §More than stomach §Cord §Anatomy §Gastroschisis vs. Omphalocele
Physical Examination §Head and neck §Shape of head §Fontanelles §Scalp edema §Face §Dysmorphic §Edema §Ears
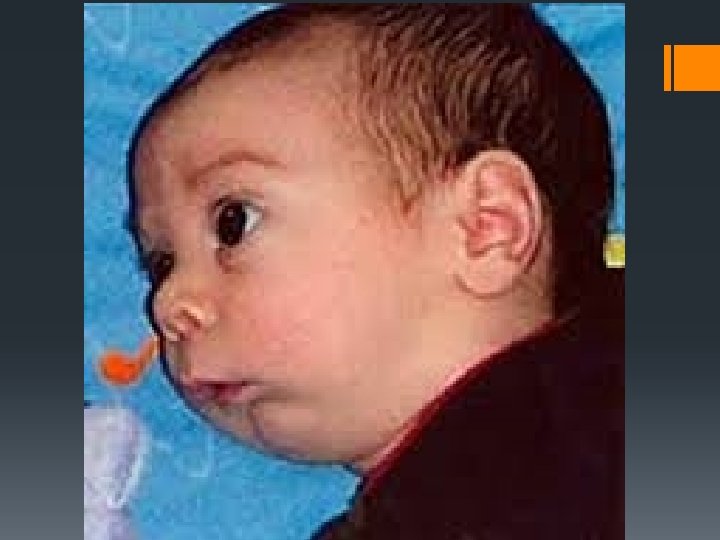
Physical Examination (cont. ) §Head and neck § Nares § Mouth §Lips §Oral cavity § Tongue size (Pierre-Robin Syndrome – micrognathia) § Neck § Clavicles
Physical Examination (cont. ) §Musculoskeletal system, spine, and extremities §Dysmorphic §Number of digits §Abnormal positioning of joints §Spine §Dimple
Spine • Figure 4 -9 • Open Spinal Defect • Figure 4 -10 • Myelomeningocele
Physical Examination §Cry §Strength §Sound
Neurologic Examination §Response to environment §Movement §Neonatal reflexes §Rooting §Grasp §Moro §Hearing
Moro Reflex
Laboratory Assessment
Laboratory Examination (cont. ) §Infection §Leukopenia (< 3, 500/mm 3) §Leukocytosis (> 25, 000/mm 3) §Platelets (<150, 000/mm 3) §Hemoglobin abnormalities §RBC (Rh) Isoimmunization §Hypoglycemia
Examination of the Pediatric Patient
Patient History §The history for a new patient can be divided into: §Chief complaint or primary concern §History of the present illness (HPI) §Past medical history (PMH) §Review of symptoms (ROS) §Family history (FH) §Social and environmental histories
Patient History (cont. ) §Chief complaint §Current signs and symptoms
History of Present Illness Box 4 -2, p. 53
Past Medical History § Components of the PMH that may contribute to establishing a diagnosis: § History of prematurity § Birthweight § Need for and duration of oxygen therapy and/or assisted ventilation in the neonatal period § Previous emergency room visits or hospitalizations for respiratory disturbances (including ICU admissions and any need for assisted ventilation) § Previous surgeries § Immunization history
Family History §Important conditions §Biological parents §Siblings §Other close relatives
Social and Environmental History §Home life §Caregivers §School §Social participation §Exposures §Travel
Review of Symptoms §Symptoms not recognized with history. §Multiple body systems. §Pulmonary Examination §Non-pulmonary Examination §Laboratory Testing
Pulmonary Examination Inspection §Child in respiratory distress § Pulmonary: Tachypnea, breathlessness, head bobbing, grunting, nasal flaring, retractions. § Non-Pulmonary: Anxiety, fussiness, irritability and not able to recognize parents. §Crying child §Vital Signs § Respiratory rate assessment while sleeping §Chest abnormalities § Pectus carinatum and pectues excavatum §Abdominal paradox
Pulmonary Examination Palpation §Bronchial (rhonchal) and tactile fremitus §Position of trachea
Pulmonary Examination Percussion §More beneficial with older children than infants or neonates.
Pulmonary Examination Auscultation §Grunting §Stridor §Stertor §Wheezing §Monophonic vs Polyphonic
Non-Pulmonary Examination §General §Growth and developmental delay §Neurological abnormalities or cerebral palsy §Muscle weakness or atrophy §EENT §Signs of allergic disorders § Otitis media § Allergic shiners § Morgan-Denie Lines
Allergic Shiners
Morgan-Dennie lines
Non-Pulmonary Examination §Heart §Abnormal rhythms §Murmurs & gallops §Prominent 2 nd heart sound §Abdominal distention §Skin abnormalities §Extremities §Digital Clubbing
Digital Clubbing
• Box 4 -6 • p. 59