Transradial Access for STEMI CRT 2012 Ramon Quesada


















 were randomized to either")








")








 with the")



 TIMI flow = 0")




- Slides: 46
Transradial Access for STEMI: CRT 2012 Ramon Quesada, MD, FACP, FACC, FSCAI Medical Director, Interventional Cardiology & Cardiac Research Baptist Cardiac & Vascular Institute Clinical Associate Professor of Medicine, Herbert Wertheim College of Medicine at Florida International University Miami, Florida
Ramon Quesada, MD I have no real or apparent conflicts of interest to report.
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Company Grant/Research Support None Consulting Fees/Honoraria Gore, Abbott, Cordis, St. Jude, W. L. NMT Medical, Terumo & Boston Scientific Corporation Major Stock Shareholder/Equity None Royalty Income None Ownership/Founder None Intellectual Property Rights None Other Financial Benefit None
Bleeding is associated with Death and Ischemic Events HR 5. 37 (3. 97 -7. 26) HR 4. 44 (3. 16 -6. 24) N=34, 146 OASIS Registry, OASIS 2, CURE trials HR 6. 46 (3. 54 -11. 79) Eikelboom JW et al. Circulation 2006; 114(8): 774 -82.
Unadjusted Rates of Bleeding and Vascular Complications of r-PCI and f-PCI in Key Subgroups: Indication for PCI Rao SV et al. J Am Coll Cardiol Intv 2008; 1: 379 -386. ) [21 Aug]
Radial access in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty in acute myocardial infarction: the HORIZONS-AMI trial Time-to-event curves for one-year cumulative: Non CABG-related major bleeding Philippe Généreux, MD, et. Al. ; PCR online Europa Edition 2011.
Radial access in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty in acute myocardial infarction: the HORIZONS-AMI trial Time-to-event curves for one-year cumulative: NACE (net adverse clinical events ) Philippe Généreux, MD, et. Al. ; PCR online Europa Edition 2011.
Radial access in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty in acute myocardial infarction: the HORIZONS-AMI trial Time-to-event curves for one-year cumulative: Death or reinfarction Philippe Généreux, MD, et. Al. ; PCR online Europa Edition 2011.
Radial access in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty in acute myocardial infarction: the HORIZONS-AMI trial Clinical outcomes according to access site and randomized antithrombotic regimen at 30 days. Philippe Généreux, MD, et. Al. ; PCR online Europa Edition 2011.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry 1, 501 propensity-matched pairs undergoing PCI at 12 hospitals in Italy, January 2003 to July 2009. Conclusion: Compared with transfemoral access, transradial PCI appears to improve outcomes in STEMI patients. Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Overall Survival P=0. 025 11. 4% 8. 8% Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Outcomes for myocardial infarction; Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Outcomes for stroke Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Outcomes for Death, MI or Stroke Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Hazard ratios for overall survival at 2 years according to selected subgroups Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
Transradial vs. Transfemoral Intervention for AMI: Analysis from the REAL Registry Major bleeding or vascular events; Propensity Score–Adjusted Kaplan-Meier Curves for Outcomes in the Overall Cohort Valgimigli M, et al. J Am Coll Cardiol Intv. 2012; 5: 23 -35.
RIVAL Outcomes stratified by STEMI vs. NSTEACS 2 N Primary Outcome NSTE/ACS 5063 STEMI 1958 % % Radial Femoral Interaction p-value 3. 8 3. 1 3. 5 5. 2 0. 025 3. 4 2. 7 4. 6 0. 011 1. 2 1. 3 0. 8 3. 2 0. 001 Non CABG Major Bleed NSTE/ACS 5063 0. 6 STEMI 1958 0. 8 1. 0 0. 9 0. 56 Death, MI or stroke NSTE/ACS 5063 STEMI 1958 Death NSTE/ACS STEMI 5063 1958 Major Vascular Complications NSTE/ACS 5063 1. 4 3. 8 STEMI 1958 1. 3 3. 5 0. 89 0. 25 1. 00 4. 00 Radial better Femoral better Hazard Ratio(95% CI) Jolly, Lancet 2011
RIVAL Results stratified by High*, Medium* and Low* Volume Radial Centres *High (>146 radial PCI/year/ median operator at centre), Medium (61 -146), Low (≤ 60) Tertiles of Radial PCI Centre Volume/yr p-value Interaction 0. 021 HR (95% CI) Primary Outcome High Medium Low Death, MI or stroke High Medium Low 0. 013 Non CABG Major Bleed High Medium Low 0. 538 Major Vascular Complications 0. 019 High Medium Low Access site Cross-over 0. 003 High Medium Low No significant interaction by Femoral PCI center volume 0. 25 1. 00 4. 00 Radial better Femoral better 16. 00 Jolly, Lancet 2011
RIFLE STEACS Trial design: Patients with ST-elevation myocardial infarction (STEMI) were randomized to either transradial or transfemoral access. Patients were followed for 30 days. Primary endpoint: Net adverse clinical events lower in the transradial arm vs. transfemoral arm: 13. 6% vs. 21. 0%, p = 0. 003 Dr. Enrico Romanagnoli, TCT 2011
RIFLE STEACS 30 -day NACE rate p = 0. 003 21. 0% p = 0. 029 13. 6% p = 0. 026 12. 2% 11. 4% 7. 2% • Net Adverse Clinical Event (NACE) = MACCE + bleeding • Major Adverse Cardiac and Cerebrovascular event (MACCE) = composite of cardiac death, myocardial infarction, target lesion revascularization, stroke Dr. Enrico Romanagnoli, TCT 2011 7. 8%
RIFLE STEACS 30 -day MACCE rate p = 0. 020 9. 2% 5. 2% p = 1. 000 p = 0. 604 p = 0. 725 1. 4% 1. 2% 1. 8% 1. 2% 0. 6% 0. 8% Dr. Enrico Romanagnoli, TCT 2011
RIFLE STEACS 30 -day bleeding rate p = 0. 026 p = 0. 002 p = 1. 000 12. 2% 7. 8% 6. 8% 5. 4% 2. 6% Dr. Enrico Romanagnoli, TCT 2011 5. 2%
RIFLE STEACS 30 -day NACE predictors OR p= 0. 002 Dr. Enrico Romanagnoli, TCT 2011 CI 95% p value Female gender 1. 5 (1. 1 -2. 3) 0. 037 CKD 2. 1 (1. 4 -3. 1) 0. 001 Radial access 0. 6 (0. 4 -0. 9) 0. 012 Killip class 1. 8 (1. 5 -2. 2) 0. 001 LAD culprit 1. 7 (1. 2 -2. 6) 0. 006 TIMI 0 basal 1. 4 (1. 0 -2. 1) 0. 073 LVEF <50% 1. 6 (1. 1 -2. 5) 0. 025 TIMI 0 -1 final 2. 4 (1. 1 -5. 1) 0. 024
Transradial Access for STEMI • Patient selection : Confirm integrity of the palmar arch. • Technical considerations: To achieve DTB time per guidelines requires an experienced transradialist. • All possible interventional scenarios in STEMI patients can be successfully accomplished via TRA.
The Learning Curve: Transradial Pitfalls • • • Access Radial Artery Spasm Anatomical Variations Transversing the Subclavian Catheter Control and Backup
Feasibility of the Radial Artery as a Vascular Access Route in Performing Primary Percutaneous Coronary Intervention (STEMI) Time Frame of Patient Triage and Procedures Cath room to reperfusion (min) Vascular access time (min) Total procedure time (min) Radial Approach Femoral Approach N= 220 N=132 26 + 13 3. 6 + 3. 1 43 + 16 25 + 11 3. 8 + 3. 5 47 + 23 Jang Young Kim et al, Yonsei Med J 2005 August; 46(4): 503 -510
Procedural Data Femoral Radial P Approach Failure 0% 2. 00% 0. 09 96. 10% 94. 30% >0. 2 18± 5 19± 6 >0. 2 Fluoroscopy Time 14± 10 16± 11 >0. 2 Hospital Stay (days) 7. 1± 5. 8 5. 6± 3. 0 0. 07 Angiographic Success Needle-to-balloon Time (mins)
Minutes STEMI: Mean Door-to-Balloon Time Femoral versus Transradial (BCVI)
Time-saving techniques for transradial STEMI • • Obtain radial access while team is prepping the patient Proceed with 1 guiding catheter for cannulation of both coronaries
Complex Transradial Interventions: AMI • Size 6 F introducer used for 95. 6% of cases • Guides: Kimny, XB 3. 0/3. 5, Barbeau • Crossing Wire: Prowater, S’port
Complex Transradial Interventions: AMI 2003 -2007 • N = 102 • Mean age Female = 66. 97 (n = 22) • Mean age Male = 62. 9 (n = 80) • Procedural Success: 97. 1% • Right Radial Access: 92. 3% • Left Radial Access: 7. 7% • Size 6 F introducer used for 95. 6% of cases • Guides: XB 3. 0/3. 5, Barbeau, Kimny • Crossing Wire: S’port BCVI Experience 2003 -2007 R. Quesada, MD, FACC
Case Example of Complex STEMI via TRA Dealing with the Unexpected Presentation
Right Subclavian Angiography • A 6 -French radial guiding catheter was advanced into the right subclavian artery and appeared to go directly into the descending aorta, despite repeated attempts to access the ascending aorta
Is this a case of a bovine arch?
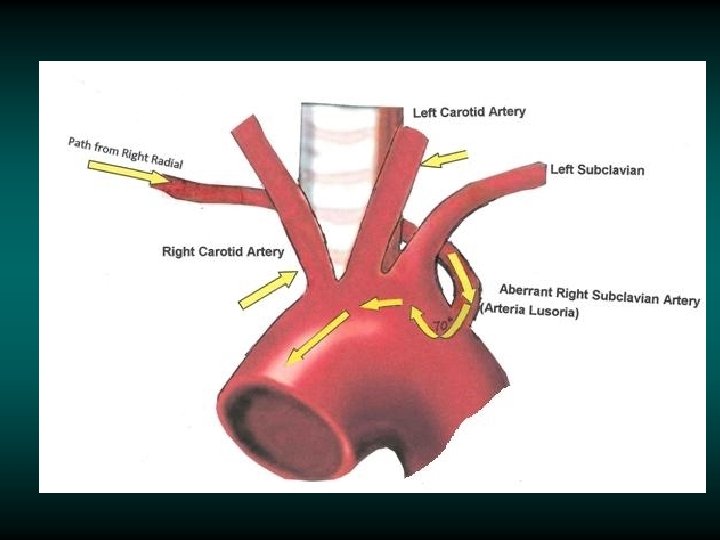
Arteria Lusoria
Technical challenge: Arteria Lusoria.
Dissection as a result of arteria lusoria Forms an acute angle (70°) with the proximal aortic arch aberrant right subclavian artery the false lumen with retained contrast medium Huang, I, J Chin Med Assoc • July 2009 • Vol 72 • No 7
How can this be overcome? • • • In an elective case switching to the left radial or femoral can be considered In this case – the patient was a STEMI and DBT was a factor Are there any technical maneuvers that would permit negotiation of this 70° angle?
No…. • • Attempting to negotiate the angle using the Kimny catheter and stiff wire could cause a dissection and a real MESS! My solution to this challenge was not to switch access but to Switch catheters… I chose an angulated pigtail catheter with a soft Benson wire.
Pre-intervention coronary angiography: note catheter angulation at the entrance of the ascending aorta
Pre-intervention coronary angiography: total occlusion distal RCA (infarct related vessel) TIMI flow = 0 GR 4 guiding catheter
Post aspiration thrombectomy Post PCI & BMS
TR Band used for compression No bleeding/access site complication
Conclusions Radial access for STEMI patients is associated with significant clinical benefits (decreased bleeding, vascular complications and mortality). Transradial access should not be considered a just a possible alternative to femoral access, but should the first choice for STEMI patients. Mastering transradial access technique requires a commitment to ensure success in STEMI patients and to meet door to balloon time requirements.
Thank You! 51