Promoting Medication Assisted Treatment for Opioid Use Disorders












 • Medical, mental health")














 formulations with improved bioavailability • Ex: Zubsolv")











 is surveying osteopathic")































 • Cooperative partnerships with")

















 for Opioids Lee. JD, The Lancet 2017")



- Slides: 95
Promoting Medication Assisted Treatment for Opioid Use Disorders Jason Fields, MD FASAM Associate Medical Director, DACCO
Scope of the Problem • 90 Americans die of an opioid overdose daily • In 2016, overdose deaths exceeded 59, 000 -- the largest annual increase ever recorded in the United States • Opioids thus have become the leading cause of death among Americans under age 50, and two-thirds of the deaths involve a prescription opioid
Current Treatment Gap Along Opioid Use Disorder Cascade of Care
Review of Medications
Overview of the Problem • 2. 1 million people in the U. S. , ages 12 and older, had opioid use disorder (OUD) involving prescription opioids, heroin, or both in 2016 • Opioid-related emergency department (ED) visits nearly doubled from 2005 to 2014 • Opioid-related inpatient hospital stays increased 64% nationally from 2005 to 2014 • Opioid addiction is linked with high rates of illegal activity and incarceration.
Introduction to TIP 63, Medications for OUD • Reviews the three FDA-approved medications used to treat OUD — methadone, naltrexone, and buprenorphine — along with strategies and services to support recovery for people with OUD • OUD medications are more effective than treatment with placebo or no medication in: • Reducing illicit opioid use • Retaining people in treatment • OUD medication can be taken on a short- or long-term basis, including as part of medically supervised withdrawal or maintenance treatment
Purpose of TIP 63 • Provides guidance for healthcare professionals and addiction treatment providers on: • Appropriate prescribing practices for the three FDA-approved medications used to treat OUD. • Effective strategies for supporting patients using medication for the treatment of OUD. • Educates patients, families, and the general public about the benefits of OUD medications and how they work.
Purpose of TIP 63 • The TIP series supports SAMHSA’s mission by providing science-based best-practice guidance to the behavioral health field. This TIP reflects relevant clinical and health service research and addresses experience and implementation requirements for delivery of OUD medication • Science demonstrates the effectiveness of medication treatment for OUD. Randomized control trials have shown that methadone, extended -release naltrexone (XR-NTX), and buprenorphine were more effective in reducing illicit opioid use than no medication • Methadone and buprenorphine treatment also have been associated with reduced risk of overdose death
Introduction to Pharmacotherapy • Overview of FDA-approved medications used to treat OUD. • How they work • Efficacy • Expanding access to pharmacotherapy is an important clinical and public health strategy • Specialty drug treatment programs should integrate pharmacotherapy. • Requirements and regulations. • Opioid treatment programs (OTPs) • Waiver for buprenorphine • Risk Evaluation and Mitigation Strategy (REMS) for buprenorphine implants and extended release buprenorphine
Introduction to Pharmacotherapy • Medically supervised withdrawal: • Often followed by relapse (Gruber et al. , 2008; Weiss et al. , 2011). • Psychosocial strategies (e. g. , contingency management) can reduce risk of relapse (Amato et al. , 2011). • Necessary prior to naltrexone treatment. • Continue medication as long as benefits outweigh risks: • Discontinuing medication is associated with relapse (Lee et al. , 2016; Sees et al. , 2000). • Inform patients of risks of discontinuing medication.
Assessment of OUD Assess patients for OUD using DSM-5 criteria if they: • spontaneously disclose opioid misuse. • screen positive for opioid misuse. • show signs or symptoms of opioid misuse. The extent of further assessment depends on the provider’s ability to treat patients directly.
Providers Not Offering Pharmacotherapy • Focus on medical assessment. • Diagnose OUD. • Discuss treatment options. • Make a treatment referral. • Provide overdose prevention information, naloxone prescription, and information on accessing sterile injection equipment. • Make a follow-up appointment.
Providers Offering Pharmacotherapy • Check Prescription Drug Monitoring Program (PDMP) • Medical, mental health and substance use history • Current medications • Physical exam • Assess opioid withdrawal, intoxication, & injection sites • Drug testing • Laboratory tests (e. g. , pregnancy, liver function, HIV, hepatitis) • Make diagnosis (DSM-5)
Treatment Planning • Share the OUD diagnose and obtain patient feedback • Use shared decision-making strategies • Medication: Yes or No • Which medication? • Where to receive medication? • Primary care. • Specialty drug treatment program. • Outpatient, OTP, residential. • Which additional services are needed and wanted? • Behavioral health. • Self-help meetings.
Patients Not Ready to Engage in Treatment • Provide information on: • Reducing injection drug risk. • Overdose prevention. • Provide naloxone prescription. • Make a follow-up appointment to mental health, medical, addiction treatment, & recovery support services as needed. • Provide resource list
Methadone • Methadone treatment is the most studied OUD treatment. • World Health Organization considers methadone an essential medication (WHO, 2015). • Clinical trials and meta-analyses show that methadone treatment is superior to treatment with placebo and to no treatment (e. g. , waiting list or supervised withdrawal with methadone) in reducing illicit opioid use (Mattick et al. , 2009).
Regulatory Issues • In the US, methadone treatment must be delivered through licensed and accredited Opioid Treatment Programs (OTPs). • Federal regulations stipulate admission criteria & services that must be provided (42 CFR 8. 12). Admission criteria: >1 year of opioid addiction prior to admission. • Can be waived for pregnant women; patients within 6 months of release from incarceration; former patients within 2 years of discharge. • Youth < 18 years of age must have: • parental consent. • >2 unsuccessful prior treatments.
Pharmacology • Review methadone’s pharmacology: • Full mu-opioid agonist. • Wide individual variability in half-life (8 to 59 hours). • 5 half-lives to reach steady state (average is about 5 days). • • metabolized largely by CYP 450 3 A 4 enzymes. • Clinical implications: • Dosing must be individualized. • Start at low dose and increase slowly. • Adequate dose: • No withdrawal symptoms for 24 hours. • Reduces or eliminates craving. • Blunts or blocks euphoria from illicit opioids.
Review of Medication Managment • Precautions: • Including QTc prolongation • Respiratory depression • Drug interactions, especially benzodiazepines and alcohol • Side effects • Assessment • Dosing considerations • Patient education
Comparative Effectiveness • Cochrane Review of RCTs comparing methadone v. buprenorphine (Mattick et al. , 2014): • Methadone patients retained longer in treatment • Methadone and buprenorphine equally effective in reducing illicit opioid use • No RCTs comparing methadone with long-acting buprenorphine formulations • No RCTs comparing methadone with XR-NTX
Methadone Dose Induction Considerations • First methadone dose: • Opioid tolerant patients: between 10 and 30 mg • Use lower dose range (10 -20 mg) for patients: • >60 years old • with lower levels of opioid tolerance based on recent history of use • treated with medications that: • are sedating • increase methadone serum levels (or stop taking ones that decrease levels) • Disorders that cause: • hypoxia • hypercapnia • cardiac arrhythmia
Methadone Dosing Considerations • Weeks 1 -2: • Avoid sedation at peak serum levels (2 -4 hours after dose). • Gradually extend the time without opioid withdrawal and craving • Individualize dosing based on careful assessment of patient response • ASAM panel recommended: 5 mg increase about every 5 days (Baxter et al. , 2013) • American Pain Society/CPDD panel recommended: 5 -10 mg increase about every 3 -4 days (Chou et al. , 2014) • Weeks 3 -4: • Suppress opioid withdrawal • Reach a dose that will blunt the euphoric effect of illicit opioids • Dose can be increased by 5 mg every 3 -4 days
Special Dosing Considerations • First dose for patients without current opioid tolerance: • An alternative for patients not wanting XR-NTX (or buprenorphine). • Former OTP patients fearing relapse • Incarcerated patients with history of OUD: • prior to release or upon returning to treatment • begin with 5 mg per day. • increase slowly by 5 mg increments every 5 – 7 days (Kinlock et al. , 2008)
Duration of Methadone Treatment • Longer stays are associated with better outcomes (Timko et al. , 2016): • Leaving methadone treatment is associated with increased risk of overdose death (Sordo et al. , 2017) • Patients should continue in treatment as long as they wish to and as long as the benefits outweigh the risks • Dose tapering request should prompt a risk benefit discussion • Plan for dose tapering should be gradual and individualized: • Offer increased psychosocial and recovery supports. • Stop taper if indicated and desired by patient
Buprenorphine • On WHO’s list of essential medications • DATA 2000 –applies only to buprenorphine formulations FDA – approved for OUD treatment • Physicians, nurse practitioners and physician assistants • 6 -month implant (Probuphine®): additional training required per FDA REMS for ordering and inserting/removing, not dispensed directly to patient • Monthly injection (Sublocade®): special certification required persuant to FDA -approved REMS, not dispensed directly to patient
Duration of Treatment • Continued medication treatment associated with better outcomes compared to medically supervised withdrawal • Expert TIP panel: • “. . . supports maintaining patients on medication for years, decades and even a lifetime if patients are benefiting. ” • Does not recommend medically supervised short-term withdrawal alone because of high rates of return to illicit opioid use • Recommends discontinuing dose reductions and allowing for dose increases if patient destabilizing, prompt re-entry to treatment, encouraging psychosocial adjuncts
Pharmacology • Review of buprenorphine pharmacology • High affinity, partial opioid agonist, improved safety profile vs. full agonists • Wide individual variability in pharmacokinetics: • Peak plasma concentrations after a first dose of transmucosal (TM) product occur between 40 min-3. 5 hours after dosing (Elkader et al. , 2005) • Long and variable elimination half-life from 24 -69 hours (Kuhlman et al. , 1998) • TM products: long half-life and partial agonist properties allow for less than daily dosing (e. g. , doubling the daily dose once stable and giving on alternate days, 12 mg daily = 24 mg every other day; Marsh et al. , 2005)
New Transmucosal Formulations • New transmucosal (TM) formulations with improved bioavailability • Ex: Zubsolv 5. 7/1. 4, Bunavail 4. 2/0. 7, Suboxone film 8/2, generic 8/2 Suboxone tablets all with bioequivalent buprenorphine exposures compared to 8/2 mg Suboxone tablet (that is no longer available) • Goals of dosing of all TM formulations: • Eliminate withdrawal • Reduce or eliminate opioid craving. • Provide effective blockade when there is illicit opioids use (patient reports diminished positive effects from the use of illicit opioid) • Be well-tolerated
Review of Transmucosal Dosing • Induction: In-office or at home. Home induction can be safe and effective (Gunderson et al, 2010; Lee et al. , 2014) • Individualize dosing –several factors to consider including level of physical dependence • For those with current physical dependence, initiate when in withdrawal with an initial 2 -4 mg dose of bup/nx. FDA label recommends a maximum dose of 8 mg on day 1 and 16 mg on Day 2. Remember some patients stabilize on lower doses. Scant data to support more than 24 mg daily • For those not currently physically dependent, initiate at lower doses (e. g. , 1 mg with slow incremental increases, holding for sedation; Vocci et al. 2015)
New Long-Acting Formulations • 6 -month implant: approved in 2016 for clinically stable patients on buprenorphine(bup)/naloxone (nx) <8 mg / day for at least 90 days • Monthly injection: recently approved for moderate-severe OUD after initiation with TM bup/nx with at least 7 days of dose adjustment
New Long Acting Formulations: Implant • 6 month subdermal implants: • Dose is 4 implants (each containing 80 mg buprenorphine), inserted in upper arm • Peak plasma concentration 12 hours after insertion • Removed & replaced after 6 months, wound care check within 1 week of implant and removal, office visits at least monthly to assess continued stability • Consider TM supplementation if destabilize – 17. 9% required in Phase 3 RCT but low dose (2/0. 5) and for short periods (Rosenthal et al. 2016) • In a non-inferiority trial, improved abstinence rates compared to SL bup/nx (Rosenthal et al. , 2016) • Approved for two rounds of implants • Serious adverse events: uncommon but possible including migration and nerve damage, potential for extraction and misuse. USE ONLY IN STABLE PATIENTS • Limited data in pregnancy
New Long Acting Formulations: Injection • Monthly subcutaneous abdominal injection: • Refrigerate, keep at room temperature for at least 15 minutes prior to injection • Dose: Months one and two 300 mg, month 3 and thereafter 100 mg (may increase if clinically indicated) • Do NOT rub or massage or let belts/waistbands rub against • Obtain baseline liver function tests(LFTs) and monitor monthly, particularly with 300 mg dose • Most common side effects were: nausea, vomiting, headache, constipation, increased LFTs, tiredness, injection site itching and pain. Uncommon: need for surgical removal of injection • Limited data in pregnancy. Contains excipient, N-Methyl-2 pyrrolindone, that has reported adverse fetal effects in animal studies
Regulatory Considerations • Waiver for physicians: • 30, 100, 275 patients. • Additional proactive reporting requirements for medical doctors (MDs) with approval to treat 275 patients. • Requires on-call service and documented diversion control plan. • Waiver for nurse practitioners (NPs) and physician assistants (PAs): • 30 and 100 patients. • 24 hours of training. • Unique requirements for new long-acting formulations.
Sample Forms • Buprenorphine treatment agreement • Patient urine drug screen and medication count monitoring form: • to assist with conduct of random urine and medication counts • Pharmacy medication count form: • sample of how to collaborate with pharmacies, particularly when patients may live closer to pharmacy than clinic. • Sample goal-setting and coping strategy forms • Checklist for induction and maintenance when using TM buprenorphine
Naltrexone • Oral naltrexone not widely used: low acceptance and poor adherence • Extended release naltrexone (XR-NTX, Vivitrol®): efficacy for preventing return to illicit opioid use after period of illicit opioid abstinence (Krupitskyet al. , 2011; Lee et al. , 2016): • Prior to release from incarceration or residential treatment • Following medically supervised withdrawal • No special regulatory requirements.
Pharmacology • Oral: peak concentrations within 1 -2 hrs, half-life ~4 hrs • XR-NTX: transient peak concentration 2 hrs after injection & then another at 2 -3 days after injection. • Concentrations gradually diminish after 14 days • Elimination half-life is 5 -10 days • Can precipitate opioid withdrawal: • Typically patients must wait ~7 -10 days after a short-acting or 10 -14 days after a long-acting opioid to initiate XR-NTX • Active area of research to effectively and expeditiously facilitate initiation of naltrexone
Comparative Effectiveness • None comparing XR-NTX to methadone or to new long-acting buprenorphine formulations • Compared to sublingual buprenorphine/naloxone: • Among inpatients undergoing medically supervised withdrawal in USA (n=580) • XR-NTX had higher return to illicit opioid use over 24 weeks outpatient study due to difficulty initiating XR-NTX (Lee et al. , 2018) • Among the groups that were able to start the two medications, there were no significant differences in relapse • 12 -week outpatient non-inferiority trial in Norway (n=159), XRNTX noninferior to buprenorphine/naloxone (Tanum et al. , 2018)
XR-NTX • Must have no signs of opioid withdrawal before administration, negative opioid test, consider naloxone challenge prior to initiating naltrexone • Dose: intramuscular 380 mg monthly (or every 4 weeks) injection into upper outer quadrant of buttock. Alternate sides every month. Proper technique critical to avoid serious injection site reactions. Follow package insert/visual aids provided • Refrigerated, keep at room temp for ~45 min before administration • Assess baseline LFTs and periodically (e. g. , 6 and 12 months intervals)
Sample Forms & Further Discussions • Patient counseling tool for XR-NTX. • Sample treatment agreement for XR-NTX. • Goal setting and coping strategies forms also applicable. • Discontinuation –discussion question and points for patient and provider.
COPE • Coalition On Physician Education in Substance Use Disorders (COPE) is surveying osteopathic and allopathic medical schools across the U. S. • Urgent need to increase attention to opioid prescribing practices, as well as the identification and management of patients who are at risk for or experiencing opioid use disorders • 55% of medical schools report that their curricula include instruction in safe and appropriate prescribing of opioids and other drugs with abuse potential • 26% of schools say their curricula address identification of older adults who are engaged in risky or non-medical use of prescription or illicit opioids and other drugs • 64% of curricula address similar issues in the care of adolescents and 49% do so with regard to pregnant women
Efficacy of MAT and Relapse Rates
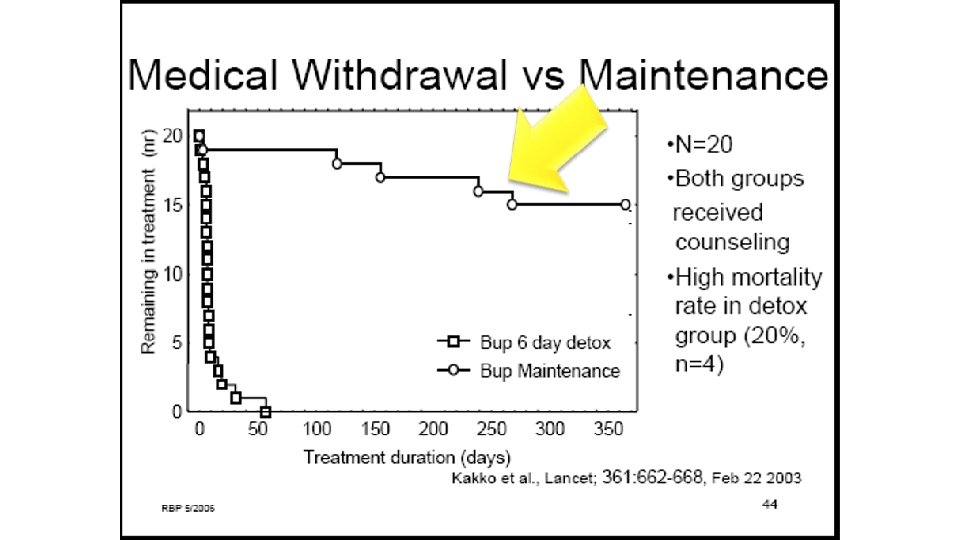
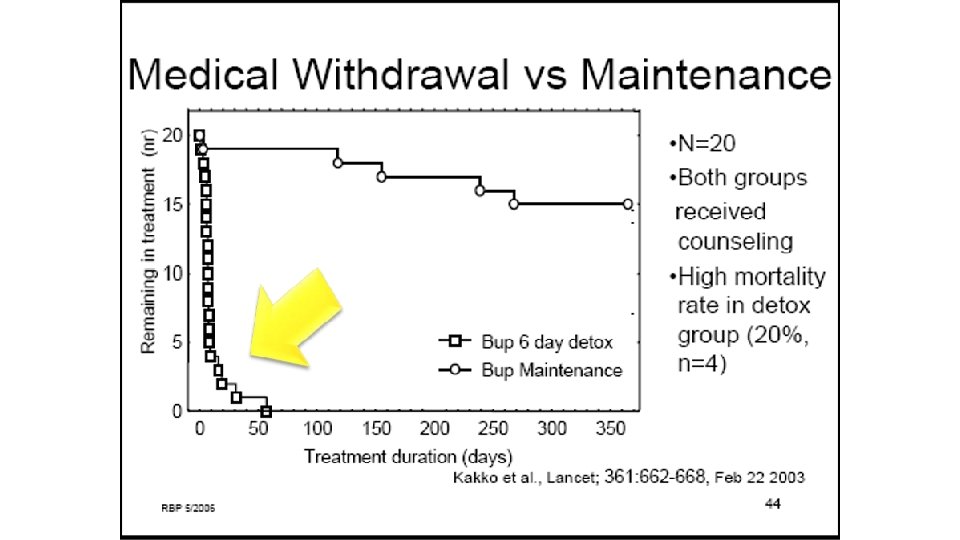
Bottom Line! • In both controlled and retrospective studies, the success rate for most medications is between 40 and 60 % (one or two years, Connery 2015) • When patients come off the medications, they relapse (Weiss 2011, Fiellin 2014) • Relapse may be associated with an increased chance of overdose and death (Kakko 2003)
Ball 1988: Reduction in IVDU with Methadone
Ball 1988: Reduction in IVDU with Methadone
Buprenorphine Long-Term Follow Up: Fiellin, 2008
No XRNTX: Abstinence 40%
XRNTX: Abstinence 50%
Ball 1988: Resumption of IVDU After Tapering Off Methadone
Ball 1988: Resumption of IVDU After Tapering Off Methadone
Buprenorphine Taper VS. Maintenance • 40 heroin addicts were started on buprenorphine/naloxone. • 20 were “detoxed” off and offered counseling. • 20 were kept on buprenorphine/naloxone and offered counseling. • A year later…….
Luty 2003: Opioid Detox During Pregnancy • 101 women underwent detox during pregnancy • 40 successfully detoxed. • No adverse fetal effects documented • BUT:
Luty 2003: Opioid Detox During Pregnancy • 101 women underwent detox during pregnancy • 40 successfully detoxed. • No adverse fetal effects documented • BUT: only 1 of 101 abstinent at delivery!
Can You Taper of Buprenorphine Without Relapse?
Can You Taper of Buprenorphine Without Relapse? • 654 patients enroll on buprenorphine for 2 weeks. • 50%stay abstinent. • They are tapered off and over 90% relapse. • 360 remain, they go back on buprenorphine for 12 weeks, • 50% stay abstinent. • They taper off and 90+% relapse. • Moral of the story: medications work as long as you take them. Weiss, 2011
42 Months Later….
Outcomes? • About half were reached by phone • No urine drug screens were done; interviews only • 32% were abstinent without M. A. T. • 29% were abstinent WITH M. A. T. • 8% were using while on M. A. T. • 31% were using without M. A. T. • Conclusion: M. A. T. was twice as successful
Other Concerns about Buprenorphine • It can be abused • (mostly for withdrawal; Kenney 2017) • It is unsafe when combined with sedatives & alcohol. • Adding naloxone (Suboxone/Zubsolv) doesn’t help (Cohier 2014) • It is an opioid. • Relapse rates after detox exceed 90%. (Weiss, 2011)
“Opioid use prevention effects weaned after treatment discontinuation”: Lee 2017 NEJM
Conclusions • “MAT” is effective-at decreasing opioid use. • Stopping MAT will usually (? ) result in relapse & potentially increased chance of death. (Sordo, 2017) • Why would you expect otherwise? • Methadone is better at keeping you in treatment. Buprenorphine has a superior safety profile. (Mattick 2014) • Vivitrol® (injectable naltrexone) is effective at reducing opioid use. (Kruptisky 2011); it doesn’t work when you don’t take it (Lee 2016)
Successful Efforts!
Successful Rhode Island Project!
CDC Recommends Use of MAT for Patients with OUD
Science = Solutions: Improving Addiction Treatment
CDC’s New Study Enrolling Through January 2019
Benzos and MAT!
AATOD Recommendations • Patients with a history of addiction are at much higher risk for benzodiazepine misuse and dependence; therefore, benzodiazepines are not the ideal treatment for insomnia or anxiety in most cases • Tolerance to benzodiazepine-induced euphoria and sedation develops quickly, and withdrawal can be life threatening • Abuse liability of specific benzodiazepines varies depending on pharmacokinetic properties, rate of absorption, metabolism, intrinsic activity and elimination half-life
AATOD Recommendations • Worldwide, 18 -50% of patients receiving methadone in Opioid Treatment programs (OTPs) are dependent on benzodiazepines • Benzodiazepine use among patients in opioid agonist medication assisted therapy is linked to poorer outcomes; the combination with opioid agonists poses significant risks for morbidity and mortality • There are few published articles that offer useful guidance for management of benzodiazepines in OTPs • As a result, treatment protocols and clinical practice vary. In spite of the gap in the literature, care should be taken with patients admitted to opioid agonist treatment with either licit or illicit benzodiazepine use
AATOD Recommendations • OTPs should be diligent and use caution when admitting patients taking benzodiazepines or any other sedating medications. • CNS depressant use is not an absolute contraindication and such use should be addressed in treatment • Adjustments in induction procedures and additional monitoring may be required • Therefore, benzodiazepine using individuals should not be categorically denied admission to OTPs • Education and the provision of educational materials of the combined risks of benzodiazepine, prescribed or illicit sedatives, opioid analgesics and alcohol use should be a routine part of orientation to opioid agonist treatment. Documentation that this was reviewed with the patient and should be entered in the record.
AATOD Recommendations • Benzodiazepines are associated with significant risk for patients in opioid agonist treatment therefore, not the treatment of choice for anxiety • Treatment plans should be developed on admission, or when indicated during treatment to address benzodiazepine use. In the great majority of cases, cessation of benzodiazepines is preferred • In some cases, admission to an OTP may be delayed until a taper/detox is completed, often requiring more monitoring in a higher level of care • In others, gradually tapering off a prescribed benzodiazepine or decreasing to the lowest effective dose is appropriate • A gradual taper from opioid agonist treatment can be therapeutic, combined with continued attempts to help patients address benzodiazepine use and decrease risks, with a goal of keeping them in treatment if possible • Continued refusal to address benzodiazepine use on the part of the patient may be grounds for discharge from an OTP
AATOD Recommendations • Patients who are prescribed or illicitly use benzodiazepines should be considered at risk for adverse reactions including overdose and death, therefore may require additional safety monitoring • Prohibiting admission or creating excessive access barriers can pose even greater threats to morbidity and mortality • A balance of providing care, medications and appropriate oversight and monitoring is necessary to successfully achieve desired clinical outcomes
AATOD Recommendations • Check the Prescription Monitoring Drug Program (PDMP) • Cooperative partnerships with prescribers allow for the exchange of information about medication use concerns and the development of a cohesive treatment plan • Program medical providers should collaborate with the prescribers improve safety and minimize risks, prescribers should be advised to decrease the benzodiazepine dose to the lowest effective dose, and consider alternative medications and non-pharmacologic treatments to address anxiety or insomnia. • If a patient is sedated, holding or decreasing the methadone or buprenorphine dose is appropriate until further evaluation is completed. • Taking steps towards further integration of opioid treatment with mental health treatment either in specialty or primary care
AATOD Recommendations • Toxicology screening should test for prescribed and illicit benzodiazepines • Toxicology screening varies and some benzodiazepines are not reliably detected. Confirming whether the benzodiazepine is taken daily or on an as needed basis is important for evaluating accuracy of unexpected negative toxicology results. • Confirmatory testing should be considered for suspicion of misuse or substitution. • Routine PMDP checks should be done for suspicion of doctor shopping.
AATOD Recommendations • There is strong evidence that the use of benzodiazepines and other sedating medications combined with methadone or buprenorphine pose safety risks • OTPs should work to ensure that patients considering controlled substances have had quality diagnostic evaluations to optimize diagnostic accuracy, and ensure that safer medication options have been considered • Careful monitoring and coordination of care that is respectful but not capricious or punitive is essential to ensure access to safe, effective and individualized care for patients in OTPs
Comorbid Benzodiazepine Use • Not an absolute contraindication to buprenorphine (www. fda. gov/Drugs/Drug. Safety/ucm 575307. htm). • Walks through considerations: • Route of use? • Prescribed or not prescribed? • If prescribed, taking as directed or evidence of doctor shopping on PDMP? • For person injecting or binging on benzodiazepines, the TIP panel recommends a higher level of care than OBOT
FDA Position on Benzos and MAT • In a September 20 th, 2017 drug safety communication, the FDA states that “buprenorphine and methadone should not be withheld from patients taking benzodiazepines or other drugs that depress the central nervous system (CNS). ” While it is true that combining these drugs can cause serious side effects, “the harm caused by untreated opioid addiction can outweigh these risks. ”
FDA Recommendations • Educating patients about the serious risks of combined use, including overdose and death, that can occur with CNS depressants • Developing strategies to manage concurrent administration of benzodiazepines or other CNS depressants—used as prescribed, or illicitly—when starting MAT • Tapering the benzodiazepine or CNS depressant to discontinuation, if possible • Verifying the diagnosis, if a patient is receiving prescribed benzodiazepines or other CNS depressants for anxiety or insomnia, and considering other treatment options for these conditions • Recognizing that patients may require MAT medications indefinitely, and their use should continue as long as patients are benefiting and their use contributes to the intended treatment goals • Coordinating care, to ensure other prescribers are aware of the patient’s buprenorphine or methadone treatment • Monitoring for illicit drug use, including urine or blood screening
MAT and Pain Issues!
MMT and Pain • Multiple studies show those in MMT report a high incidence of pain: – 39% report moderate to severe pain – 61% report a current pain condition – Up to 88% of patients enrolled in or seeking entry to MMT reported having experienced pain in the preceding week • Compared to individuals in the general population: – 31% of those surveyed having a current chronic pain condition – 26% reported pain in the preceding month
MMT, Pain, Health and Quality of Life • Over-utilization of health care due to physical illnesses leading to surgery; and other MH illness (depression, anxiety, somatization • Lower than average social and physical functioning • Disruption of relationships, employment, and normal activities of daily living • Increase in non-opioid drug use during and after treatment • Reduced satisfaction with treatment • Lower likelihood of reporting that an adequate dose of methadone was received
Finding Appropriate Dose of Methadone for MMT in Patients with Pain • Increased pain sensitivity (hyperalgesia) caused by chronic opioid use • Increased opioid tolerance • Increased licit and illicit use of opioids by patients to manage pain • Inappropriate attitudes toward pain and addiction on the part of patients and health care professionals
Pain Management in MMT • Clinicians misunderstanding of pharmacology of methadone is a barrier to adequate analgesia • Common misperception is dose of methadone taken is, in and of itself, adequate to provide relief of pain (6 hours of analgesia) • Need a different dosing strategy with different analgesic to obtain relief of pain
High Impact Publications
EPI: CDC Overdose DATA FOR 2016
Fentanyl in the US Heroin Supply O’Donnell, MMWR 2017:
Fentanyl Analogs Cause Spike in Overdose Deaths Prekupec, Journal of Addiction Medicine 2017
Opioid Deaths Decrease US Life Expectancy Dowell, JAMA 2017
Prevalence of Prescription Opioid Use and Misuse Han, Annals of Internal Medicine 2017
Diagnosis, Assessment, Early Intervention: Pathways to OUD Stumbo, Journal of Substance Abuse 2017
Pharmacological Interventions: XRNaltrexone v BUP-NX (film) for Opioids Lee. JD, The Lancet 2017
Pharmacological Interventions: XR-NTX vs Daily BUP Tanum. L, JAMA Psychiatry, 2017
Ethical & Policy Considerations: Overdoses & MAT in CJS Green, JAMA Psychiatry 2018
Questions? ! jasonf@dacco. org