Medication Assisted Treatment For Opioid Use Disorders Shannon





















 2000 – Schedule")




 -- daily --4: 1 buprenorphine to naloxone")
 --buprenorphine mono-product --8 mg equivalent --Remove and reinsert")
 --Buprenorphine mono-product --Repeat injections every 4 weeks 2")
 • Dosing range from 232 mg SL daily – FDA does")









- Slides: 48
Medication Assisted Treatment For Opioid Use Disorders Shannon Allen, MD Jade Wellness Center July 19, 2018
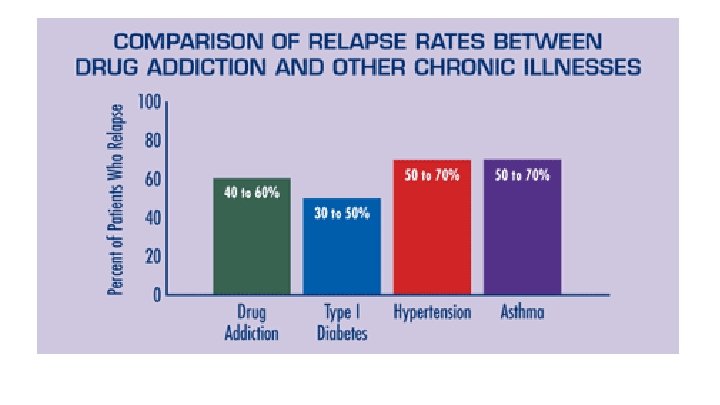
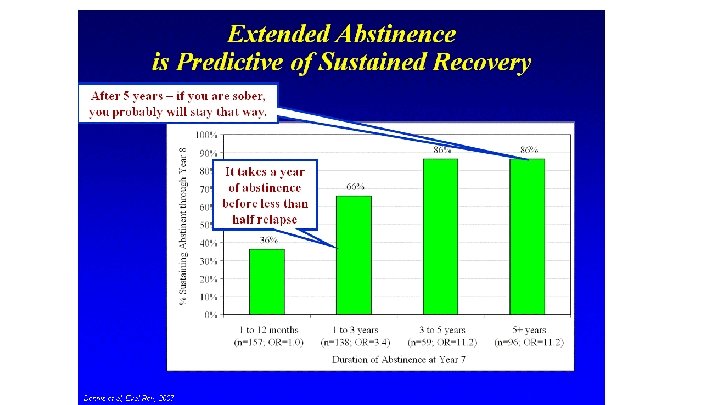
Rates of Relapse in Opioid Use Disorders are High
Benefits of Medication Assisted Treatments • Reduce risk of overdose and death • Improve social functioning • Reduce risk of infectious disease transmission • Reduce engagement in criminal activities • Improved maternal and fetal outcomes • Increased retention in treatment • Safe
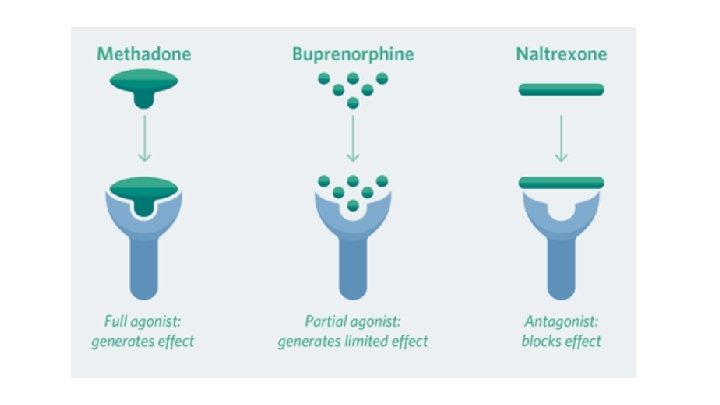
MAT Formulation Receptor Pharmacology DEA FDA Treatment Schedule Setting Approval in Pregnancy Naltrexone PO tablet Full mu opioid antagonist Not FDA approved, Not standard of care Long acting intramuscular injection Implant (not FDA approved) Nonnarcotic Not schedul ed Physician’s office, Opioid Treatment program, other health care setting
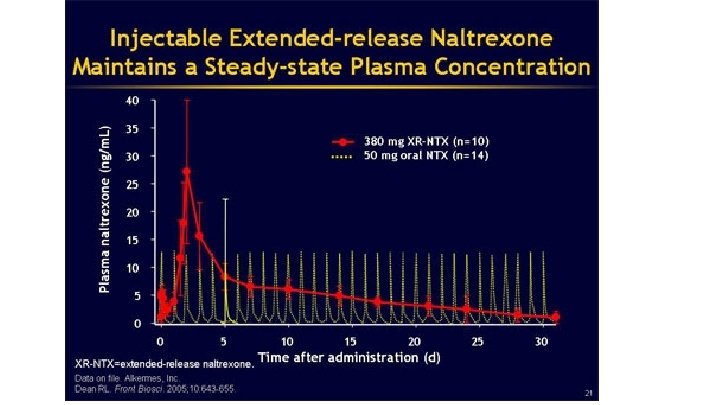
PO Naltrexone: Revia – Range 25 mg – 150 mg /day – FDA recommends 50 mg /day IM Naltrexone: Vivitrol -380 mg dose, Q 4 weeks -IM in the buttocks -Compliance is a huge barrier to treatment success
Benefits of Naltrexone • • • Reduces cravings Prevents effects of opiates Reduces rates of relapse to opiates Any physician can prescribe No physiologic dependence Promoted by abstinence based models of treatment
Lee, J. D. , Friedmann, P. D. , Kinlock, T. W. , Nunes, E. V. , Boney, T. Y. , Hoskinson Jr, R. A. , … & Gordon, M. (2016). Extended-release naltrexone to prevent opioid relapse in criminal justice offenders. New England Journal of Medicine, 374(13), 1232 -1242. Improved Opioid Outcomes with XR-NTX: Lower relapse rates Greater percentage of opioid-negative UDS Longer time to relapse Zero overdoses
Adverse Side Effects of Naltrexone • • • Nausea, Vomiting Headache Appetite decreased Insomnia Dizziness Diarrhea Arthralgias Anxiety Depression, suicidal thoughts CPK increased • Black Box warning for hepatoxicity – Monitor LFTs – Contraindicated in acute liver disease – Decreased risk with Vivitrol
Injection Site Reaction with Vivitrol • Increased risk if injection occurs in SC adipose layer • Redness, induration, swelling, tenderness • Can lead to cellulitis, abscess, necrosis
Precipitated Opioid Withdrawal with Naltrexone • Recommendation is to be opioid free for minimum 710 days • Naloxone Challenge • Can be a barrier to starting antagonist treatment
Risk of Opioid Overdose with Naltrexone Accidental overdoses occur: • After detox from opioids, before first dose is administered • With attempts to overcome the opioid receptor blockade • Using opioids after discontinuation of treatment • Using opioids after missing a dose
Barriers to Naltrexone • • • Lack of insurance or finances to pay for it Patient lack of awareness Physician lack of knowledge Incarceration Complexity of ordering XR-NTX Complexity of administering
MAT Formulation Receptor Pharmacology Methadone Oral soln, Full mu opioid liquid agonist concentrate, table or diskette, powder FDA Approval in pregnancy DEA Treatment Schedule Setting Never formally approved by FDA, Gold standard II Opioid Treatment Programs
Historical Context of Methadone Maintenance • Dr. Vincent Dole, becomes chair of Narcotics Committee of the Health Research Council of NYC. Joins with Dr. Marie Nyswander, an addiction psychiatrist, and together develop methadone as a maintenance therapy in 1964 – “Methadone maintenance provides a safe and effective way to normalize the function of otherwise intractable opiate addiction” • 1973 – Methadone Control Act Establishes federally funded clinics for prevention and treatment of opioid dependence. Regulates licensing for dispensing methadone.
Methadone Pharmacology • Extensive bioavailability – Up to 80% orally bioavailable • Long elimination half life, ranging from 22 -36 hours – Allows for daily dosing • Peak serum levels in 2 -4 hours – Highest rates of sedation, euphoria, analgesia • Tolerance remains stable – No need to escalate the dose (vs. short acting opioids) • Hepatic metabolism through CYP 450 enzymes – Major substrate of CYP 3 A 4 isozyme
Opioid Treatment Programs SAMHSA-certified program, that engages in supervised assessment and treatment for individuals who are addicted to opioids. • Can include IOP, residential programs, hospital settings • Variety of on-site services – medically supervised withdrawal – maintenance treatment – medical, psychiatric, psychosocial and other types of supportive care. • High level of regulations (federal, state, county, etc. )
Eligibility For Methadone Maintenance – Must be 18 years old • some states make exception for 16 -18 yo – Must have at least 12 months of physiologic dependence to opioids • Exceptions: pregnancy • Exceptions: high risk populations such as HIV positive, recently released from incarceration – Must meet requirements for moderate to severe Opioid use disorder
Methadone Maintenance Goals Of Treatment • • relieve narcotic craving suppress the abstinence syndrome block the euphoric effects associated with opiates Minimize side effect profile Dosing • Doses > 60 mg per day are recommended • Most people stabilize between 60 – 120 mg daily
Methadone Side Effects Constipation, GI upset Excessive sweating Drowsiness, fatigue Decreased libido, hypogonadism QTc prolongation (and Td. P) – Increased risk with high dose methadone (>100 mg) • Respiratory depression • Central sleep apnea • Death – usually due to respiratory arrest (esp with BZD, Et. OH) or fatal arrhythmia • • •
Barriers to Methadone Maintenance Treatment • • • Lack of insurance or finances to pay for treatment Incarceration – Only 55% of prison systems allow for prescription of methadone Logistics of frequent dosing – Transportation, childcare, time off from work, etc Legal involvement Must meet state eligibility
MAT Formulation DEA Receptor FDA Treatment Schedule Setting Pharmacol Approval ogy in Pregnancy Buprenorphine Sublingual tablet or film *mono-product *combinationproduct with Naloxone Partial mu opioid agonist Subdermal implant Subcutaneous injection Not FDA approved III Physician’s office, Opioid Treatment program, other health care setting
History of Buprenorphine Maintenance • Drug and Alcohol Treatment Act (DATA) 2000 – Schedule III, IV, V medications can be prescribed as maintenance treatment for opioid dependence – qualifying physicians can receive a waiver from the special registration requirements in the Controlled Substances Act – Can be office based (vs. OTP) • In 2002, FDA approves buprenorphine as a schedule III medication for treatment of opioid dependence
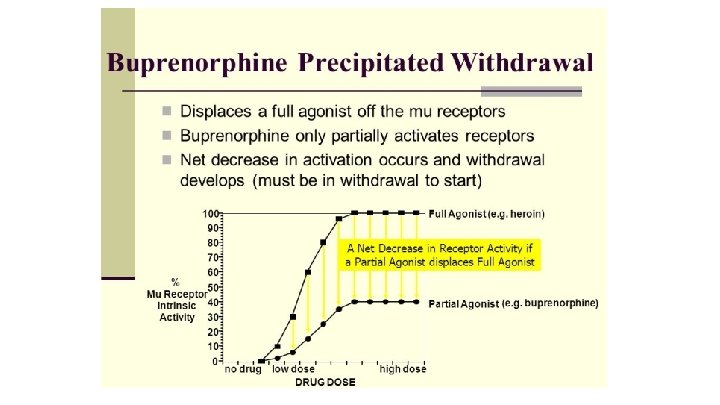
Buprenorphine Properties • High Receptor Affinity – Can precipitate withdrawal • Slow Dissociation (long ½ life) – Elimination half life is 20 -73 hrs (mean 37 hrs) • Low Intrinsic activity (partial agonism)
Buprenorphine Pharmacology • Partial agonist at mu opioid receptor – Low intrinsic activity – Creates ceiling effect – Reduced side effect profile – Reduced risk for respiratory depression and overdose
Buprenorphine Induction • Patients are advised to abstain from short-acting opiates for >24 hours, long acting opiates for >48 -72 hours • Goal: Moderate Withdrawal – COWS >10 – CINA >10 • Buprenorphine is initiated at low dose – 2 -4 mg – If no precipitated withdrawal within 2 hours, can repeat dose (up to 8 mg on day 1)
Buprenorphine Formulations • Poor oral bioavailability • <40% of SL administration • 2 sublingual formulations – Buprenorphine (Subutex) • Preferred formulation in pregnancy and breastfeeding – Buprenorphine with naloxone (Suboxone, Zubsolv) • 4: 1 buprenorphine to naloxone • Naloxone, only active if IV or IM administration • Added to limit diversion
Buprenorphine Formulations • Buccal formulation (Bunavail) -- daily --4: 1 buprenorphine to naloxone
Buprenorphine Formulations • Subdermal implant (Probuphine) --buprenorphine mono-product --8 mg equivalent --Remove and reinsert at 6 months --Must complete training to prescribe and surgically insert/remove
Buprenorphine Formulations • Subcutaneous injection (Sublocade) --Buprenorphine mono-product --Repeat injections every 4 weeks 2 x 300 mg, then 100 mg maintenance dose --corresponds to 100% mu receptor occupancy --Must be REMS certified --Blackbox warning: intravenous administration can result in potentially fatal thrombo-embolic events
Buprenorphine Dosing (sublingual) • Dosing range from 232 mg SL daily – FDA does not support doses above 24 mg – Typically therapeutic dose is 16 mg SL daily – 95% receptor occupancy at 16 mg (Greenwald et al. 2003) – Some managed care will not cover more than 16 mg, or more than 1 year of treatment
Buprenorphine Side Effects • • Constipation, GI upset Excessive sweating Drowsiness, fatigue Decreased libido, hypogonadism QTc prolongation? ? Central sleep apnea Respiratory Depression (especially with BZD) – Children are vulnerable
Diversion of Buprenorphine is Uncommon In 2014, Buprenorphine made up United States Reasons: To manage withdrawal To self treat pain To self treat depression <1% of all reported drugs diverted in the
Barriers to Buprenorphine Maintenance • Lack of insurance or finances to pay for treatment • Fear of legal consequences • Incarceration – Only 14% of prison systems allow for prescription of buprenorphine • Not enough certified or trained prescribers – Patient limits • Of all physicians with waivers, <½ are not treating patients – Lack of support services – Difficult, time consuming – Fear of audits
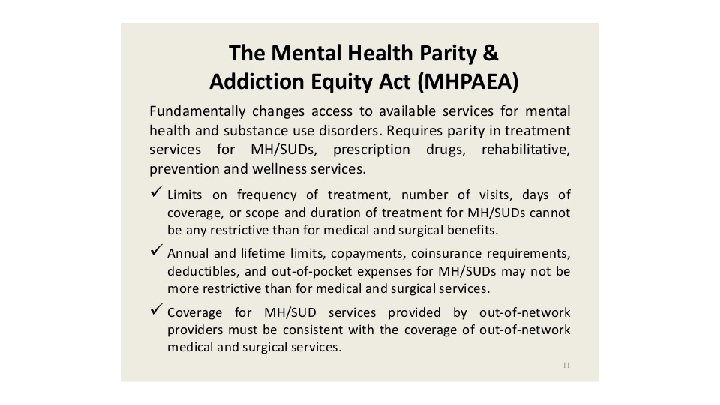
MAT Barriers: Insurance Coverage • • • Initial and Reauthorization Requirements Limits on dosages Limits on quantity “Fail First” criteria Annual or lifetime medication limits Refusal to cover specific MAT
MAT Barriers: Provider • Inadequate Training – Treatment of addiction is limited in medical school and residencies – Therapists are not trained about MAT • • Negative attitude, Stigma Follow Abstinence Base Philosophy Suboptimal Dosing Preference for detox or tapering off
MAT Barriers: Pharmacy • • Refusal to carry MAT Negative attitudes, Stigma Additional Requirements Refusal to fill prescriptions
MAT Barriers: Patients • • • Stigma, negative attitude Confidentiality concerns Inconvenient Lack of information Fear of legal consequences
Which MAT Should I Choose?
Treatment Works! But no single treatment is right for everyone