Growth Refers to increase in the physical size



.")







 Later")

: A test for evaluating development")











 development of newborn infant is difficult to")





: About 2 -3 days after delivery, the skin of")



















 Blue pale Body pink but extremities")


- Slides: 56
Growth Refers to increase in the physical size of the body or body part. It is usually assessed in its of measurement, such as kilograms, centimeters, inches or pounds.
Development Refers to a gradual change in function, that results in more complex skills and abilities or it refer to progressive increase in skills and capacity of functions.
Principles of growth and development: Each child has an individual rate and style of growth and development. Both growth and development are a synchronous All areas of growth and development are interrelated. Newly learned skills predominate. Growth and development occur in an orderly sequence.
Principles of growth and development: Growth and development progress from head to toe (cephalocaudally). Growth and development progress from the body midline toward the periphery (proximodistally) e. g. stand; sit before the usage of fine muscles of hands. Development progresses from simple to complex and from general to specific. Children's behavior is directed toward competency. Growth and development are continues process, each stage depends upon the preceding one.
Factors That Affect growth and development Genetic: genetic factors may set limits to biologic potential, but these intimately interact with the environment. Nutritional: decreased proteins, minerals or vitamins quantitatively or qualitatively may cause retarded growth and development. Debilitating diseases interfere with adequate nutrition e. g. chronic diarrhea, parasitic infestation and tuberculosis. Over nutrition may cause obesity. Intrauterine infections: e. g. congenital rubella, toxoplasmosis and cytomegalovirus diseases. Endocrinal disorders: hypothyroidism.
Factors That Affect growth and development Emotional deprivation: children who are securely attached are able to use their parents to reestablish a sense of wellbeing after a stressful experience, such as a physical examination or immunization. Emotional deprivation can lead to impaired growth and development. Socioeconomic: poverty is associated with poor growth. Chromic diseases: if starting early in life may cause retarded growth e. g. chronic asthma, chronic renal failure and liver cirrhosis. Exposure to environmental pollutants: e. g. lead and mercury.
Types of growth physical growth includes Head size: ¼ of the length of the body at birth, where the adult's head size is is ⅛ of his height. Head circumference. Thoracic diameter. Weight. Height or length. Arm circumference. physiological growth includes Temperature, pulse and respiration, and blood pressure
Types of development Motor development e. g. sitting, standing, running, usage of fine muscles. Intellectual development e. g. problem solving. Social development e. g. raising and training a child in the culture of his family group. Emotional/ personality development needs for trust, love. Language development Moral development
Causes of delayed motor development without mental retardation: Familial and emotional disturbances. Protein energy mal nutrition. Rickets. Poliomyelitis. Benign hypotonia Chronic diseases. Muscle, bone and joint diseases.
Causes of delayed motor development with mental retardation: 1 - Cerebral palsy often associated with abnormality 2 - Chromosomal abnormality e. g. , trisomy 21 syndrome 3 - Hypothyroidism 4 - Inborn errors of metabolism such as galactosemia, phenylketonuria and lipid storage diseases 5 - CNS infection 6 - Intrauterine infections
Stages of growth and development I- Prenatal period: Ovum (0 – 14 days after conception) Embryo - (14 days - 8 weeks of gestational phase) Fetus(8 weeks of gestational phase - birth) II- Postnatal period. Infancy: from birth to 12 months Neonate (newborn) (from birth to four weeks of life) Infancy (1 month - 12 months) Early childhood (1 - 6 years) -Toddler(1 - 3 years) - preschool (3 – 6 years)
Stages of growth and development Middle childhood/ school age (6 - 12 years) Later childhood: from 11 to 19 years from puberty to adulthood Early adolescent / late childhood (12 - 14 years) Middle adolescent (14 - 16 years) Late adolescent (16 – 19 years)
Assessment of growth: Measurement of physical growth in children is a key element in evaluating their status. Physical growth parameter include weigh, height (length), skin fold thickness, arm circumference, and head circumference. Values for this growth parameter are plotted on percentile charts and the child's measurements in percentiles are compared with those of the general population.
Assessment of development: Denver Developmental Screening Test (Engel, 2006): A test for evaluating development in children from 1 month to 6 years of age. 4 Main Rated Categories of DDST- Denver development screening test Language communication Personal social-interaction Fine motor adapting- prehensile ability to use hand movement Gross motor skills- large body movement
1. Embryo begins with conception and end with child's birth
The Normal newborn infant Definition: The period from birth to four weeks. It is transitional period for an individual as he transfers from intrauterine life to extrauterine environment, where newborn infant has to adapt to it.
General body-proportion: The head of a newborn represents one fourth of his total length. - The size of face is small when compared with total head size. - The neck is usually short, creased and difficult to clean. - He has relatively short thorax and soft rounded abdomen. - The genitalia are small and may be swollen. - The extremities are short in relation to body length. - The feet are always flat because of the presence of fatty pad. -
Physical growth a. Weight: Most newborn infants weight 2. 700 to 4. 000 gm at birth. They lose 5% to 10 % of weight by 3 to 4 days after birth as result of: Withdrawal of hormones from mother. Loss of excessive extra cellular fluid. Passage of meconium (feces) and urine. Limited food intake. -They gain birth weight by l 0 th days of life. -Gains ¾ kg by the end of the first month.
b. length: Average boy's is 50 cm and 49 cm for girls (normal range for both sexes 48 to 53 cm). Gain 3. 5 cm by the end of the first month
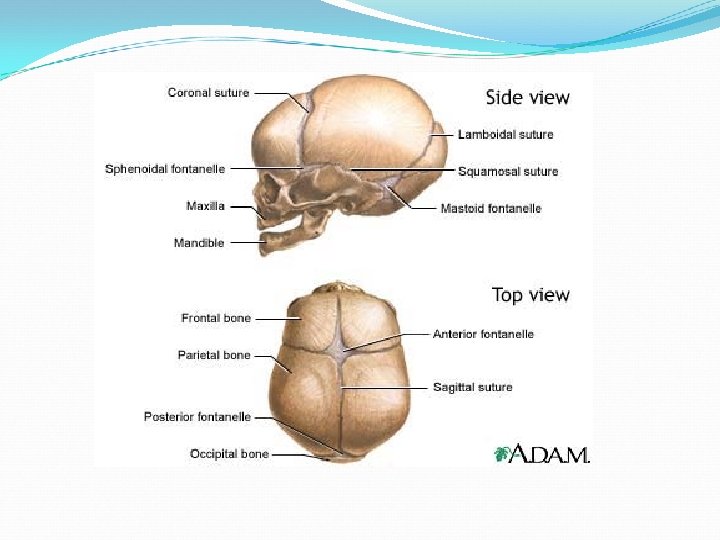
The head: - The new born infant's head circumference equals or exceeds that of his chest and abdomen. The normal limits of head size are 33 – 35 Cm. - The fontanels are soft spots (when they are open) they consist of openings at the point of union of the skull bones. - The anterior fontanel is diamond shape and located at the junction of two parietal and two frontal bones. It is 2 -3 Cm in width and 3 -4 Cm in length. It closes between 12 -18 months of age. - The posterior fontanel is triangular and located between the occipital and parietal bones. It closes by 2 nd months. - The fontanels bulge when the baby cries or strains or if there is an increased intra-cranial pressure.
d. Chest circumference: 30. 5 to 33 cm (usually 2 -3 cm less than head circumference). Physiological Growth Vital signs: a. Temperature: At birth, newborn infant's temperature is slightly higher than mother. It will drop immediately after birth in adjustment to delivery room temperature unless the newborn infant is kept warm immediately after birth. Temperature rises to normal within about 8 hours. Temperature of newborn Infant is usually 36. 5 to 37. 6 Co
b. Pulse: 120 -150 b/min. it is usually rapid and irregular c. Respiration: 35 to 50 c/min. It is usually irregular in depth, rate, and rhythm. Senses: Touch - It is the most highly developed sense. It is mostly at lips, tongue, ears, and forehead. - The newborn usually is comfort with touch.
b. Vision: - Pupils react to light. - Bright lights appear to be unpleasant to newborn infant. - Follow objects in line of vision. c. Hearing - The newborn infant usually makes some response to sound from birth. - Ordinary sounds are heard well before 10 days of life. The newborn infant responds to sounds with cry or eye movement, cessation of activity and I or startle reaction.
d. Taste: - Well developed as bitter and sour fluids are resisted while sweet fluids are accepted. e- Smell - Only evidence in newborn infant's search for the nipple, as he smell breast milk
Development A. Motor Development His movements are random, diffuse, and uncoordinated. Lack muscular strength to hold head steady and erect (his head sink down). Reflexes carry out bodily functions and responses to external stimuli. Gross: May lift head if prone. Alerts to high-pitched voices. Fine: Holds hand in fist. When crying, he draws arms and legs to body.
B. Cognitive Development The cognitive (intellectual) development of newborn infant is difficult to understand or observe it. C. Emotional Development Newborn infant expresses his emotional just through cry for 'hunger, pain, or discomfort sensation. D. Social Development - Cry is his contact with environment to communicate his physiologic needs as hunger
Systematic physical examination: General Appearance: Posture: Flexion of head and extremities while rest on chest and abdomen. Skin: At birth, bright red, puffy smooth. Second to third day dark pink and dry. It is soft and has good elasticity or tissue turgor due to hydrated subcutaneous tissue. It is evident when a skin fold is grasped and then released, it will promptly go back to normal smooth state. Edema is seen around eye, face, legs and scrotum or labia. Cyanosis of hands and feet.
Vernix caseosa: It is a soft, yellowish cream which covers the neonates skin to protect it from sebaceous gland mixed with old epithelial cells. It may thickly cover the baby at birth or it may be found only in the baby creases and between the labia. It dries off within 24 – 48 hours and fades spontaneously and rubs off on the infant's clothes. Some nursery units still believe that vernix is a good culture medium for bacterial growth and remove it all. Others consider that it protect, the baby against skin infection and keep it.
Lanugo: It is a relatively long soft growth of fine- hair. Observed on the shoulders, back extremities, forehead and temples of the neonate. The more premature baby is, the heavier the presence of lanugo is. It disappears during the first weeks of life.
Mongolian spots: Mediterranean and Negro, Indian and mongolian babies often manifest black colorations on the lower backs –buttocks, anterior trunks and rarely on fingers and feet They are not bruise marks or a sign of ill treatment and are not associated with mental retardation. They disappear during preschool years without treatment.
Desquamation: Pealing of the skin occurs within 2 -4 weeks of life. There are denoted areas where the delicate skin has been rubbed off the nose, knees and elbows, because of pressure and erosion of sheets. The skin of buttocks is particularly sensitive and should not be left wet and / or soiled.
Physiologic jaundice (or Ictrus neonatorum): About 2 -3 days after delivery, the skin of many infants begin to take on a yellow coloration. This jaundice is not pathological. It is thought to be with the expected excessive destruction of erythrocytes (R. B. Cs) that are no longer needed after birth. It increases for a few days and usually disappears by the seventh day.
Milia: These are small pinpoint white or yellow spots, common on the nose, forehead, cheeks and chin of the newborn infants they can be felt with the finger they consists of accumulation of secretions from the sweat and Sebaceous gland that have not yet began to function normally- They will disappear within a few weeks (One to two weeks). They should not be expressed.
Head: The fontanels are soft spots. Consist of openings at the point of union of the skill bones. The anterior fontanel; is diamond in shape and located at the junction of two parietal and frontal bones. It is 2 -3 cm in width and 3 -4 cm in length. It closes between 12 -18 months of age. The posterior fontanel; is triangular and located between the occipital and parietal bones. It closes by the 2 nd month of age.
Two conditions may appear in the head. These are caput succidaneum and cephalhematoma. Caput Succidaneum; is edema of the scalp resulting from pressure during labor. Cephalhematoma; is a hemorrhage under the periostieum of one of the cranial bones (usually parietal) resulting from trauma of labor.
Comparison of Caput Succedaneum and Cephalhematoma: Characteristics Caput Succedaneum Cephalhematoma Appears At birth no increase in size. Several hours after birth increase in size for 2 -3 ow. Disappears Several days after birth. Approximately 6 weeks after birth. Border Vague, poorly defined. Marked, well defined. Cross suture line Sometimes. Never. Cause Diffuse, edematous swelling. Subperiosteal hemorrhage. Complications Rarely anemia. Jaundice, underlying skull fracture, intra-cranial
Eyes: Lids: Usually edematous. Color: Gary, dark blue, brown. True eyes color is not determined until the age of 3 -6 months. Pupil: React to light. Absence of tears. Blinking reflex in response to light or touch Ears: Position: Top of pinna on horizontal line with outer canthus of eye. Startle reflex elicited by a loud sudden noise. Pinna flexible, cartilage present.
Nose: Nasal patency. Nasal discharge – thin white mucous. Mouth and throat: Intact, high-arched palate. Uvula in midline. Sucking reflex- strong and coordination. Rooting reflex. Gag reflex. Minimal salivation. Neck: Short, thick, usually surrounded by skin folds. Tonic neck reflex present.
Systematic assessment of the Neonate: 1 - Gastrointestinal System: Mouth: Should be carefully examined for gross abnormalities such as cleft lip and cleft palate. Epstein pearls are: Little, white, shine spots near the center of the hard palate. They mark the fusion of the 2 hollows of the palate. It will disappear in time. It should be differentiated from thrush (oral Moniliasis).
Gum: May appear with a quite irregular edge sometimes back of gums may be whitish deciduous teeth are semi-formed burnet erupted. Cheeks: Have a chubby appearance due to development of fatty sucking pads that helps to create negative pressure inside mouth and facilitate sucking.
Stomach and Intestines The capacity of infant’s stomach varies after birth from 3060 cc and increase rapidly. Many infants swallow air during feeding so eructation is necessary. Abdomen: Cylindrical in shape. Liver: Palpable 2 -3 cm below costal margin. Spleen: Tip palpable at end of first week of age. Umbilical cord: Bluish white at birth with two arteries and one vein. It is formed of gelatinous connective tissue called Wharton’s jelly. The cord shrinks, dries and drops off its place of attachment heals in about 7 -10 days.
Circulatory system: Heart: Apex- fourth to fifth intercostal space, lateral to left sternal border. S 2 sharper and higher in pitch than S 1. In fetal life, the circulatory system severs as modified respiratory system since O 2 isn’t obtained through breathing but through umbilical cord. Respiratory system: Slight sternal retraction evident during inspiration. Respiratory chiefly abdominal. Cough reflex absent at birth, present by 1 -2 days.
Possible signs of respiratory distress to be aware of are: 1 - Cyanosis of other than hands and feet. 2 - Costal or substernal retractions. 3 - Flarring Nostril. 4 - Expiratory grunt-heard with or without stethoscope.
Urinary system: 1 - Normally, the Newborn has urine in his bladder and voids at birth or some hours later. Newborns pass urine within 24 hours after birth. If delayed it should be reported. Female genitalia: Labia and clitoris usually edematous. Urethral meatus behind clitoris. Vernix caseosa between labia. Male genitalia: Urethral opening is at tip of glans pens. Testes palpable in each scrotum. Scrotum usually large edematous, pendulous and covered with rugae and pigmented.
Endocrine system and genital area: Swollen Breasts: This appears on the 3 rd day in both males and females. It lasts for 2 -3 weeks and gradually disappears without treatment. The breasts should not be expressed as it may result in infection or injury to tissues. Sometimes there is also a breast secretion called "Witch's Milk".
2 - Infantile Menstruation: Maternal hormones in uterus cause the endometrial lining of female fetus to thicken. When it is withdrawn after birth, this thickening is no more maintained. Tiny menstrual flow is observed. This consists of few spots of blood for 12 days can be seen in the diaper.
The nervous system: Reflexes: Certain reflexes are absolutely essential to the infants life as protective reflexes: Blinking reflex – It is aroused when the infants is subjected to light. Coughing and sneezing – to clear the respiratory tract. Gagging to prevent choking.
A number of reflex actions are involved in feeding: The rooting reflex- causes the infant to turn his head towards anything which touches his cheek and is his way of reaching for food. Sucking reflex-provide sucking movements when any thing touches the lips. Swallowing reflex – it follows sucking reflex. The gagging reflex – comes into play when he has taken more into his mouth then he can successfully swallow can also cough if a little of the fluid is swallowed the wrong way and enters the trachea.
Other reflexes: The grasp reflex – An infant will grasp any object put into his hands, hold on briefly and then drop it. Moro reflex (Startle reflex) – this reflex is aroused by a sudden loud noise or loss of support. The reaction is aimless muscular activity. It demonstrates an awareness of equilibrium. In its absence the possibility of brain damage must be considered. The tonic-neck reflex: , It is a postural reflex in which the infant, when lying on his back turns his head to one side and extend the leg on the side to which the head is turned
Extremities: Ten fingers and toes. Full range of motion. Nail beds pink, with transient cyanosis immediately after birth. Creases on anterior two thirds of sole Symmetry of extremities. Equal bilateral brachial pulse.
Apply nursing care plan for a child with new born (Refers to Wong DL (2010). (Fig. 2): Apgar Scoring Chart The Apgar Scoring Chart is a simple test done by looking at the baby: After 1 minute. After 5 minute.
Item 0 1 2 1 - Appearance (color) Blue pale Body pink but extremities blue Completely pink 2 - Pulse. Absent. Less than 100/rn More than 100/m. 3 - Grimace reflex irritability to catheter in nose. No response. Cry, some motion and sluggish. Cough or sneeze, vigorous, cry. 4 - Activity muscle tone. Flaccid. Some flexion of Well flexion of extremities. 5 - Respiration. None. Slow-irregular. Good-strong cry.
If the Apgar score is 4 or below i. e. there is cyanosis, heart rate below 100 beats / minutes and inadequate or difficult respiration, he will need oxygen and possibility other methods of resuscitation. If he has a score of 510, he usually needs no treatment.