Diagnosis Treatment of Pediatric Epilepsy Joseph E Sullivan



 36%")












? Diagnose an underlying condition that requires")







 Not")


=37% Remote symptomatic (ie neonatal HIE,")





 Abortive medications Specialized diets Surgery Resective Devices, ie")

 available in U. S. Many used “off-label” Very few")
 Phenytoin (Dilantin) Lamotrigine")
-infantile spasms, seizures in setting of tuberous sclerosis ACTH/steroids-infantile spasms")




 ** carbamazepine (Tegretol) Ethosuximide")










 No relationship with epilepsy")

 JRA patients (%) Odds ratio (CI) No high school")


































- Slides: 92
Diagnosis & Treatment of Pediatric Epilepsy Joseph E. Sullivan, M. D. Assistant Professor of Clinical Neurology & Pediatrics Director, UCSF Pediatric Epilepsy Center
Outline Proper seizure/epilepsy classification Why treat? When to treat? Treatment options Outcomes
Epilepsy Classification History, history Tests are ancillary and rarely confirmatory Describe what the observer saw FIRST! Behavior arrest Staring Eye deviation Myoclonic jerk
“New-onset” seizure clinic History, history from the WITNESS 74% were diagnosed epileptic (94/127) 36% had previous ambiguous event 41% had abnormal EEG 64% were imaged and 18% were abnormal Hamiwaka, LD, et. al. Epilepsia, 48(6): 1062 -66, 2007
Infantile Spasm
Head drop/atonic
Atonic-myoclonic
Eyelid Myoclonia
Focal Seizures Focal sensory Focal motor Clonic Asymmetric tonic posturing With automatisms Gelastic Secondarily generalized seizures
Focal clonic
Frontal
Supplementary Motor
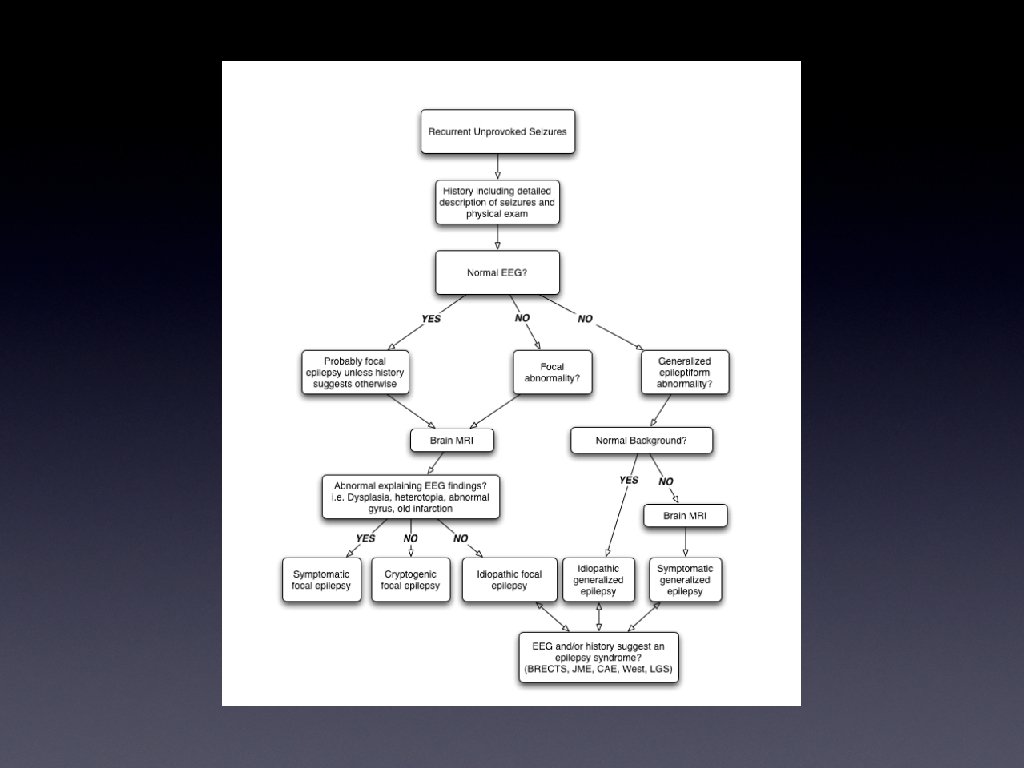
EEG Evaluate background Screen for inter-ictal discharges or focal slowing Rarely capture an event/seizure Video EEG
EEG 2 -5% of normal children may have abnormal EEG 50% of children with epilepsy may have normal single EEG 3 EEG’s including sleep 90% abnormal Treat patients NOT EEG abnormalities
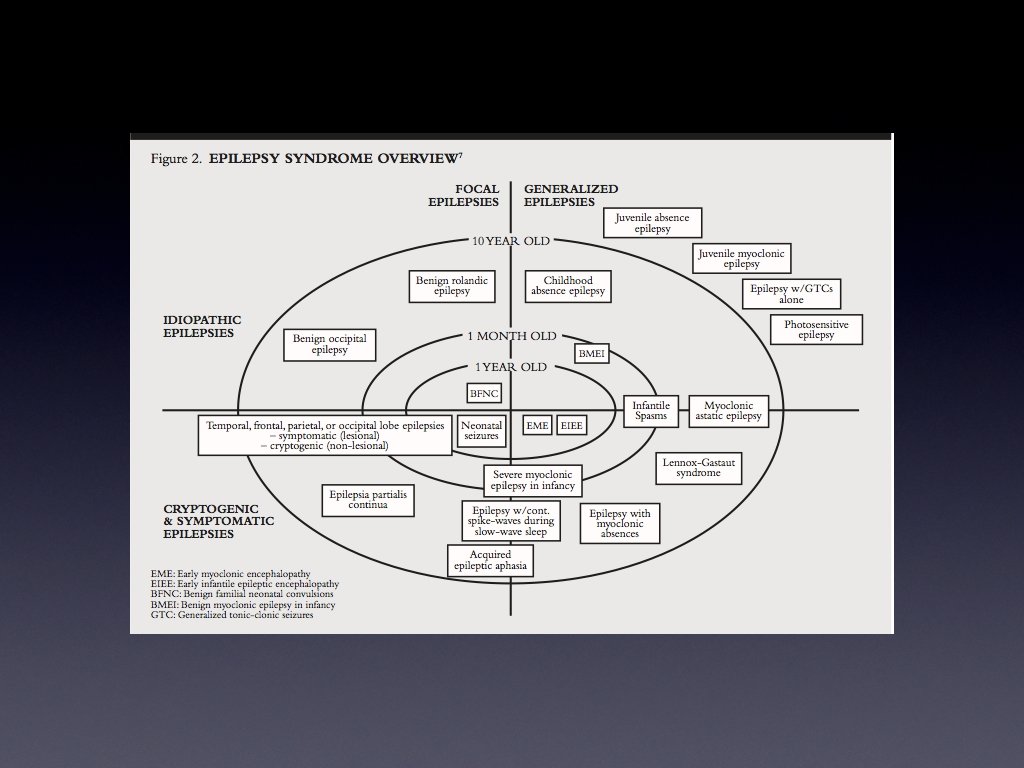
Classification 59% of newly diagnosed children have focal epilepsy 20% may have specific epilepsy syndrome diagnosis 12% unable to be classified at diagnosis
Neuroimaging
Reasons to order urgent neuroimaging (usually in ED)? Diagnose an underlying condition that requires immediate intervention. Hemorrhage Stroke Cerebral Abscess Tumor with resultant hydrocephalus
Abnormal Imaging Scenarios Must know prior to d/c from ED New bleed, abscess Good to know within 2 -4 weeks Tumor Whenever Malformation of cortical development, remote encephalomalacia
Evidence based? 500 children with a first non-febrile seizure 475 imaged in the ER 8% with “clinically significant” abnormalities 3/475 had findings needed immediate intervention 1 shunt failure 1 increased intra-cranial pressure after head trauma 1 with new-onset infantile spasms and a neoplasm Sharma et al. Pediatrics 2003; 111: 1 -5
High risk groups High-risk groups to image in the ER Known bleeding or clotting disorders Known hx of malignancy HIV infection Closed head injury Less than 33 months with a focal seizure Sharma et al. Pediatrics 2003; 111: 1 -5
Who was missed Age History 2 mos 6 min seizure 3 y Status epilepticus Abnl mental status 9 y 4 min seizure Normal 10 y 10 min seizure New Right hemiparesis 12 y 5 min seizure Normal 16 y 4 seizures Physical Exam Hypertension Diagnosis Management Subdural Child abuse hematoma eval, no surgery Anoxic brain ICU admit, pt injury died 5 mm arachnoid AED started cyst Benign frontal Resection 6 wk lobe tumor later Grey matter AED started heterotopia Hypertensive Anti-HTN and encephalopathy AED started Sharma et al. Pediatrics 2003; 111: 1 -5
But what about a brain tumor! 200 consecutive children with new diagnosis of brain tumor 30/200 (9%) presented with a seizure 19/30 had focal seizures 11/30 had generalized seizures Wilne et al. AJDC 2006; 91: 502 -506
Of the 30 patients presenting with seizures 17 had no other symptoms and a normal exam 14/17 focal seizures 3/17 generalized seizures 2/3 had focal slowing on EEG 1/3 atypical absence seizures Wilne et al. AJDC 2006; 91: 502 -506
AAN Practice Parameter Recommendation “Evaluating a first nonfebrile seizure in children” If a neuroimaging study is obtained, MRI is the preferred modality. Emergent neuroimaging should be performed if there is a post-ictal focal deficit not quickly resolving, or who has not returned to baseline within several hours after the seizure. Hirtz, D Neurology 2000; 55: 616 -623
Who to admit Children less than 1 year old Prolonged seizure (>15 minutes) Not back to baseline after 4 hours
What to tell parents Back to some key components in the history Child neurologically normal? Did the seizure occur while awake or asleep? Simple questions but very important
Overall Recurrence Risk 42% recurrence Mean time to recurrence 11. 3 months 36% in first month 53% in 6 months 88% in 2 years
Normal Child vs Abnormal Child Cryptogenic (ie otherwise normal)=37% Remote symptomatic (ie neonatal HIE, history of stroke, autism, etc)=68%
But the seizure was 1 hour long! First time seizure as status does NOT affect recurrence risk 12% of Shinnar cohort presented with status Recurrence risk at 2 years is still 38% for cryptogenic kids Of those with status 21% of those who had a recurrence had recurrence of status. Don’t be afraid to give Diastat in these cases
Why do we treat? Reduce recurrence risk Prevent prolonged seizures Minimize impact on development/academic achievement Does NOT affect natural history if you are going to outgrow it, you will regardless of treatment
The Normal Child Awake, and normal EEG=19% Asleep, normal EEG-37% Awake, abnormal EEG=42% Asleep, abnormal EEG=63% Shinnar, S Pediatrics 1996 ; 98: 216 -225
When to treat? Depends on the patient/family and seizure frequency Daily, weekly, monthly seizures Every 6 months Yearly Prolonged seizures/convulsions
Treatment? Every child/family is different Treatment may reduce recurrence risk by as much as 50%. AED’s are toxic medications! For the most part we do not treat after a first time seizure. The one exception- Remote symptomatic presenting in status. Shinnar, S Pediatrics 1996 ; 98: 216 -225
Treatment options Daily anti-epileptic drugs (AED’s) Abortive medications Specialized diets Surgery Resective Devices, ie Vagal nerve stimulator
No seizures and No side effects!
Medications 16 anti-epileptic drugs (AED’s) available in U. S. Many used “off-label” Very few studies in children
First vs Second generation First generation Second generation Phenobarbital Ox-carbazepine (Trileptal) Phenytoin (Dilantin) Lamotrigine (Lamictal) Carbamazepine (Tegretol) Gabapentin (Neurontin) Ethosuxamide (Zarontin) Valproate (Depakote, Depakene) Benzodiazepines Lorazepam (Ativan) Midazolam (Versed) Diazepam (Valium) Clonazepam (Klonipin) Chlorazepate (Tranxene) Topiramate (Topamax) Levetiracetam (Keppra) Zonisamide (Zonegran) Pregabalin (Lyrica) Lacosamide (Vimpat)
Special siutation AED’s Vigabatrin (Sabril)-infantile spasms, seizures in setting of tuberous sclerosis ACTH/steroids-infantile spasms Felbatol-medically resistant atonic/drop seizures
What is the difference? 2 nd generation AED’s have wider therapeutic windows No need to follow levels Can increase based on side effects Less interactions with other drugs Most have similar efficacy
Just pick a drug from a hat? Some AED’s are better for specific seizure types/syndromes Absence-Ethosuxamide (carbamazpine is contraindicated) Juvenile myoclonic epilepsy-valproate, lamotrigine, levetiracetam Co-morbidities Avoid AED’s that could worsen co-morbidities Favor AED’s that may help co-morbidities Formulation (liquid, sprinkle, tablet, capsule)
Common Co-morbidities Weight gain-ox-carbazepine, valproate, gabapentin, pregabalin Weight loss-topiramate, zonisamide Altered blood counts- carbamazepine, valproate Headaches-topiramate, carbamazepine, valproate, levetiracetam
Side Effects Phenobarbital-sedation Valproate-weight gain, liver toxicity, decreased platelets, pancreatitis Sodium abnormalities-ox-carbazepine Lamotrigine-Steven’s Johnson syndrome Topiramate-weight loss, language dysfunction, kidney stones, glaucoma Levetiracetam-irritability, agitation
Pediatric formulations Liquid Sprinkle Chewable tab Phenobarbital ** Divalproate (Depakote) ** carbamazepine (Tegretol) Ethosuximide (Zarontin) Topiramate (Topamax) Lamotrigine (Lamictal) ** carbamazepine (Tegretol) Zonisamide (Zonegran) valproic acid (Depakene) Vigabatrin (Sabril) sachet powder Ox-carbazepine (Trileptal) Levetiracetam (Keppra) Felbatol (Felbamate) ** 3 -4 times per day
Treatment Goal Single medication at a dose with NO side effects If first medication does not work-trial of another single medication If second medication alone is not effective, trial of polytherapy (2 or more drugs) Rarely are 3 medications better than 2 Side effects increase
Outcomes Most children with epilepsy do VERY well One study 83% required a single AED in first year of treatment 61% of these were seizure free off meds at end of study---REMISSION Only 4% with favorable response in first year developed intractable epilepsy 17% with inadequate control 42% still achieved remission 29% develop intractable epilepsy Camfield, PR et. al. , J Pediatr, 1997: 131: 821 -24
Long Term Follow-up 37 year f/u of 144 patients 31% enter remission in first year of Rx 19% are resistant from the beginning Overall 67% achieve terminal remission 14% on AED’s 86% off AED’s Sillanpaa, M & Schmidt, D Brain 2006, 129, 671 -624
When to wean? Seizure free for 2 years Single seizure type Normal EEG on AED’s Normal IQ Normal neurologic examination
Less “favorable” factors Age greater than 12 years Family history of epilepsy Frequency of seizures at onset (>21) Slowing on EEG Remote etiology
“At-risk” population Remission rates are much less than those with developmental disabilities Should still consider if sz free>2 years Recurrence risks: Spastic hemiplegic CP-61% DD only 52% The “nightmare”-relatively rare 2/41 children with DD Camfield, C, et. al. , J Pediatr 1993; 122: 861 -8 Delgado, MR, et. al. Pedaitrics 1996; 97: 192 -197
Neuropsychological Status in children Distinct neuropsychological profiles in different epilepsy syndromes Often confounded by seizure burden and medication side effects What about children with “new-onset epilepsy”
New-onset Epilepsy Prospective study of 53 children with recent -onset idiopathic epilepsy Diagnosis of epilepsy within the past 12 months No other developmental or neurologic disorder Normal MRI Neuropsychological assessment performed & compared to age/gender matched firstdegree cousins. Hermann, B, Children with new-onset epilelpsy: neuropsychological status and brain structure, Brain: 129, 2609 -2619
Results Epilepsy patients exhibited poorer performance across all measures Hermann, B, Children with new-onset epilelpsy: neuropsychological status and brain structure, Brain: 129, 2609 -2619
LRE vs PGE LRE but NOT PGE differ from controls in language and memory Hermann, B, Children with new-onset epilelpsy: neuropsychological sstatus and brain structure, Brain: 129, 2609 -2619
Academic Achievement 26% presented with history of academic problems (AP) No relationship with epilepsy syndrome, age, number of medications MR volumetrics reveal no differences in white matter volume when compared to controls In those with AP-significant volume reductions in left parietal and left occipital grey matter. Hermann, B, Children with new-onset epilelpsy: neuropsychological sstatus and brain structure, Brain: 129, 2609 -2619
Social Consequences Nova Scotia population-based cohort 56 patients with CAE 61 patients with JRA Inteviewed at mean age of 23 years Terminal remission CAE=57% JRA=28% Wirrell et al, Long-term psychosocial outcome in typical absence epilepsy. Sometimes a wolf in sheeps’ clothing, Arch Pediatr Adoles Med, 1997 151(2); 152 -8
Social Outcomes CAE patients (%) JRA patients (%) Odds ratio (CI) No high school graduation 36 14 3. 7 (1. 3 -10. 4) Special classes 16 3 5. 7 (1. 1 -40. 5) Repeated a grade before diagnosis 20 3 7. 6 (1. 4 -52. 8) Ever considered a behavior problem 41 10 6. 4 (2. 2 -19. 9) Unplanned pregnancy 34 3 19. 3 (2. 3 -426. 1) Psychiatric or emotional problems 54 31 2. 6 (1. 1 -5. 9) Unskilled laborer 53 16 5. 9 (1. 6 -24. 0) Manager or professional 0 36 undefined Not employed in area of training 50 14 5. 7 (1. 2 -33. 9)
Autism and Epilepsy 75% of children with autism will have abnormal EEG 25 -30% will have epilepsy Absence of MR- 2 -8% Presence of MR- 7 -27% Remission rates low- 16% Tuchman, RF, et. al. Pediatrics 1991; 88: 1219 -1225
14% of 155 children with autistic regression had abnormal EEG vs 6% without regression No difference in incidence of AR between those with and without epilepsy Significance is unclear and very controversial Treat patients NOT EEG abnormalities
Abortive medications A medication that is given for a prolonged seizure or seizures that cluster Rectal vs. buccal Diastat is studied and approved for rectal administration Buccal/nasal delivery of midazolam Intermittant diazepam or lorazepam for children who cluster in setting of fever/illness
Beyond Medications 5% of patients per year will become seizure free with additional AED trials Consider alternative measures Ketogenic/Atkin’s Diet Surgery
Ketogenic Diet Described in New Testament and by Hippocrates Starvation was noted to improve “fits” High fat, low carbohydrate diet mimics starvation Very effective Reports of between 20 -45% seizure free 67% have >50% reduction in seizures Very restrictive
Modified Atkin’s Diet Less restrictive but still only 10 -20 g carbs/day Liberalize protein and fat 5 -15% may become seizure free 60% may have >50% reduction If some effect, can always transition to classic ketogenic diet
Pre-surgical evaluation First tier Video EEG for ictal recording High-resolution MRI Second tier Magnetoencephalography (MEG) Positron emission tomography (PET) Single photon emission computed tomography (SPECT)
Lesional epilepsy Complete resection of lesion AND electrographically abnormal region 92% have good outcome sz free or >90% reduction Electrographically abnormal region Electrocortiography Chronic subdural grid recordings Palocchi, JM, et. al, Neurology 2000 54(3): 642 -47
Non-lesional epilepsy Subdural grid/strip recordings are mandatory At 2 year follow-up 44% seizure free 15% >90% reduction 17% >50% reduction 10 year follow-up 33% seizure free Jayakar, P et. al. , Epilepsia 2008 49(5) 758 -64
VNS Implanted under chest wall and wire wrapped around left vagus nerve Unclear mechanism of action Vagus nerve projects widely throughout cerebrum Higher incidence of cardiac related side effects if implanted on right side
VNS complications Hoarseness Cough Reflux <1% symptomatic bradycardia
VNS efficacy <5% seizure free 50% experience 50% reduction of seizures magnet swipes may shorten/abort prolonged seizures
Comprehensive Epilepsy Center Team approach Pediatric epileptologist High-quality neuroimaging High field MRI, f. MRI, MEG, PET Experienced neuroradiologists Pediatric neuropsychologist Pediatric epilepsy surgeon Experienced EEG technologists Nursing
Questions?
Febrile Seizures An event in infancy or childhood, usually occuring between 3 months and 5 years, associated with fever but without evidence of intracranial infection or other definable cause.
Febrile Seizures Simple-primarily generalized seizure lasting <15 mins and not recurring in 24 hours Complex-focal, prolonged, or more than 1 seizure in 24 hours Epilepsy-recurrent, non-febrile/unprovoked seizures
Febrile Seizures 2 -5% of children Epilepsy 0. 5 -1%
Clinical Characteristics 16 -35% of initial FS are complex Risk factors for 1 st FS-FHx of FS, delayed development, daycare attendance
Laboratory Evaluation “The workup of a child who has had a febrile seizure and has recovered consists solely of the work-up of the fever (Vining & Freeman, 1985)
Lumbar Puncture How many children with meningitis present with seizure and fever 503 cases of meningitis 115(23%) had seizures 105 were obtunded or comatose other 10 had nuchal rigidity (6), prolonged seizure(1), petechial rash (1), viral meinigities (2)
Lumbar Puncture Mental status is highly predictive 79% of meningitis cases had complex FS Pretreatment with Abx may be a concern Recent FEBSTAT study 80% of 102 pts had LP 8% had more than 5 WBC’s All traumatic
Lumbar Puncture FEBSTAT study 80% of 102 pts had LP 30%-0, 40%-1, 15%-2, 5%-3, 1%-4 8% had more than 5 WBC’s All traumatic Normal protein and glucose Finding of >5 WBC’s in a non-traumatic LP should be a concern
Imaging No good studies FEBSTAT-some hippocampal signal abnormalties in first 72 hours, in those with febrile status Also finding hippocampal malrotation (17% >30 mins, 9% <30 mins, 1% simple FS)
EEG Hypothesized reasons for obtaining EEG Help with estimating risk of recurrence Help stratifying those that will go on to develop epilepsy 3 -4% will show spikes or spike-wave activity close to the 1 -9% incidence of focal sharp activity in normal young children
Factors affecting recurrence risk Age at onset Simple vs. Complex Neurodevelopmental exam Duration of fever Height of Temperature Family History of Febrile Seizures
Age at onset Less than 12 mos of age has increased risk of developing recurrence of febrile seizure 48. 4% vs. 29. 6% in older group Different or longer period of time at risk
Laboratory Evaluation Does not affect risk of recurrence for febrile seizures 30% vs. 37% Does affect risk of developing epilepsy Overall risk of developing epilepsy with a simple febrile seizure is approx 2% If initial seizure is complex this is increased
Combining Risk Factors
Epilepsy risk & complex features per/1000
Duration of fever
Height of fever
Treatment? Phenobarb will decreased recurrence to as low at 5% Side effects including irritability, agression, neurodevelopmental effects Antipyretics? Ibuprofen 5 mg/kg, not effective Acetominophen 10 mg/kg also not effective Did reduce mean temp, but not max van Stuijvenberg et al 1998 Uhari et al, 1995
What to do? Seizure often first sign of fever Difficult to argue against, but warn parents that it still may not work!
Conclusions Most FS are benign events Stratification allows identification of high risk groups Work-up need not be extensive Very few treatment options Treatment should be reserved for special situations