Pediatric Chest Physical Diagnosis Dr Khalid AlMobaireek Pediatric

Pediatric Chest: Physical Diagnosis Dr. Khalid Al-Mobaireek Pediatric Pulmonologist King Khalid University Hospital

What are the basic clinical skills? Communications History taking Explaining the diagnosis to a patient Presenting the case n Medical interviewing n Physical examination n

Goal: To establish a favorable context for the interview Welcome the patient n Wash your hand n Know and use the patient's name n Introduce and identify yourself to the patient and to the care giver. n Ensure comfort and privacy (ask) n

Goal: To establish the agenda for the interview Obtain list of all issues - avoid detail if not needed n Chief Complaint n Other complaints or symptoms n Open-ended questions initially n

History: Chief Complaints, HPI n n Main Respiratory symptoms: u Cough u Noisy breathing u SOB If problem is chronic: u Course u Variability u Describe exacerbation u Describe the patient between the attacks u Previous therapies and investigation u Effect of the problem on the child and family

History: n n n n n Systemic review Perinatal and delivery History Past Medical and surgical Hx. Past Drug and allergy Hx. Vaccination Hx. Nutritional Hx. Developmental Hx Family Hx. Social and environmental Hx.

Do Not ignore the Child

Do not scare the child. Do not be rough

Remember One complaint at a time n Start with open ended question n Move from general to specific n

Examination of the chest Equipment Needed n A Stethoscope n A Blood Pressure Cuff n A Watch Displaying Seconds n A Thermometer n PEF n

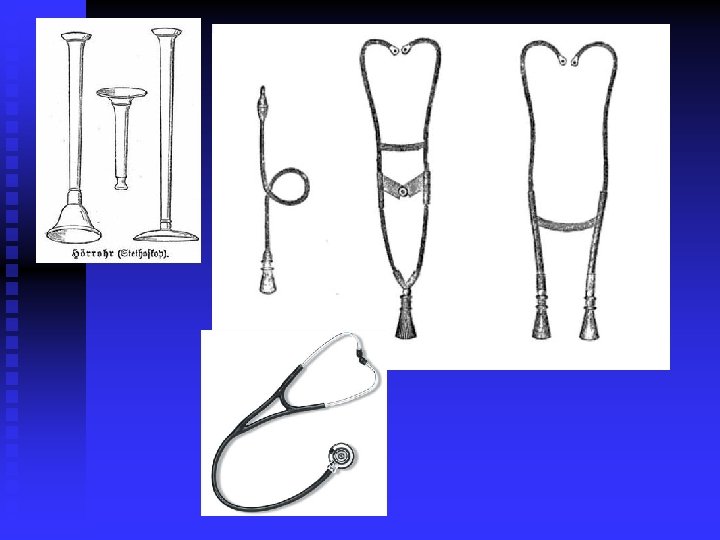
Stethoscope most widely used in clinical medicine since its introduction almost 200 years ago. n symbolic value for the health care profession n Every child knows that doctors have stethoscopes. n

n n invented in France in 1816 by René Laennec at the Necker. Enfants Malades Hospital in Paris Laennec called his device the "stethoscope" (stetho + -scope, "chest scope").

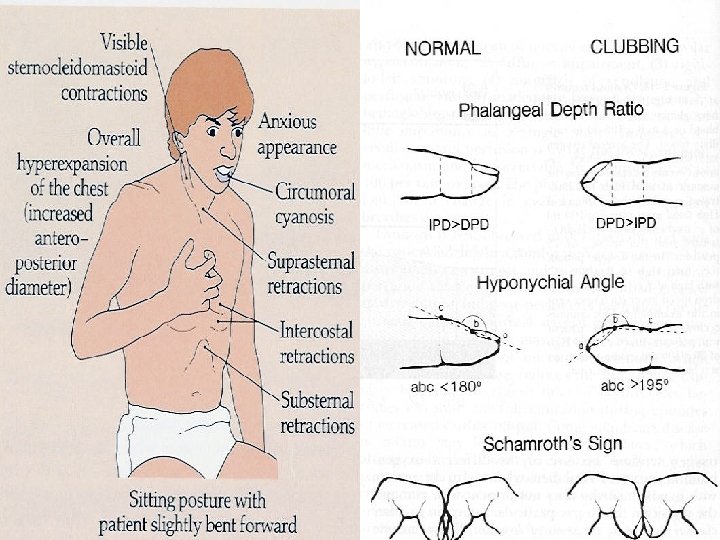
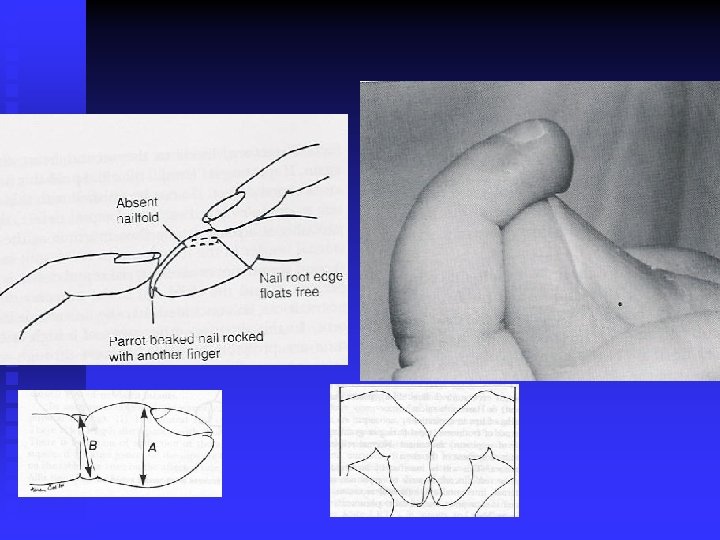
General: Respiratory rate, rhythm n BCG scar n Ears, sinus tenderness, tonsils, nose. n Retractions, head bobbing, ala nasi, hunched shoulders n Cyanosis n Clubbing n

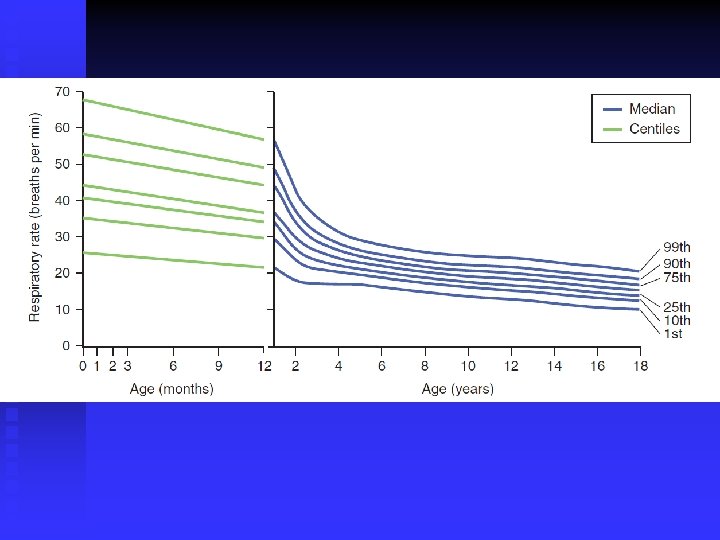
Respiratory Rate n n Best done immediately after taking the patient's pulse. Do not announce that you are measuring respirations. Count breaths for 1 minute. Take in account the patient behavior, temprature

Pulse Rates at Rest Age Lower Limits of Normal Average Upper Limits of Normal Newborn 70/min 125/min 190/min 1– 11 mo 80 120 160 2 yr 80 110 130 4 yr 80 100 120 6 yr 75 100 115 8 yr 70 90 110 10 yr 70 90 110 Girls Boys 12 yr 70 65 90 85 110 105 14 yr 65 60 85 80 105 100 16 yr 60 55 80 75 100 95 18 yr 55 50 75 70 95 90 Girls Boys
 measurements in boys from birth to 12")
A, Age-specific percentiles of blood pressure (BP) measurements in boys from birth to 12 mo of age. B, Age-specific percentiles of BP measurements in girls from birth to 12 mo of age. C, Age-specific percentiles of BP measurements in boys 1– 13 yr D, Age-specific percentiles of BP measurements in girls 1– 13 yr of age
 measurements in boys 13– 18 yr of")
A, Age-specific percentiles of blood pressure (BP) measurements in boys 13– 18 yr of age. B, Age-specific percentiles of BP measurements in girls 13– 18 yr of age
 Blood Pressure (mm Hg)")
Vital Signs at Various Ages Age Heart Rate (beats/min) Blood Pressure (mm Hg) Respiratory Rate (breaths/min) Premature 120– 170 * 55– 75/35– 45 40– 70 0– 3 mo 100– 150 * 65– 85/45– 55 3– 6 mo 90– 120 70– 90/50– 65 30– 45 6– 12 mo 80– 120 80– 100/55– 65 25– 40 1– 3 yr 70– 110 90– 105/55– 70 20– 30 3– 6 yr 65– 110 95– 110/60– 75 20– 25 6– 12 yr 60– 95 100– 120/60– 75 14– 22 12 * yr 55– 85 110– 135/65– 85 12– 18


Certain pattern? Inspection n Palpation n Percussion n Auscultation n Special test n

Chest Exam n n The patient must be properly undressed & gowned for this exam Ideally the patient should be setting on the end of a table but in pediatric it depend on the age of the patients. The examination room must be quite to do adequate percussion and auscultation notes. Try to visualize the underlying anatomy during the examination.

Inspection Observe the chest for any asymmetry or deformity n Note any scar , lesions or rash n Observe the rate , rhythm , depth & effort of breathing n Observe the apex beat n

Tachypnea n n n n decreased compliance of the respiratory apparatus metabolic acidosis. fever (approximately 5 to 7 breaths per minute increase per degree above 37° C). Anemia Exertion intoxication (salicylates Anxiety psychogenic hyperventilation.

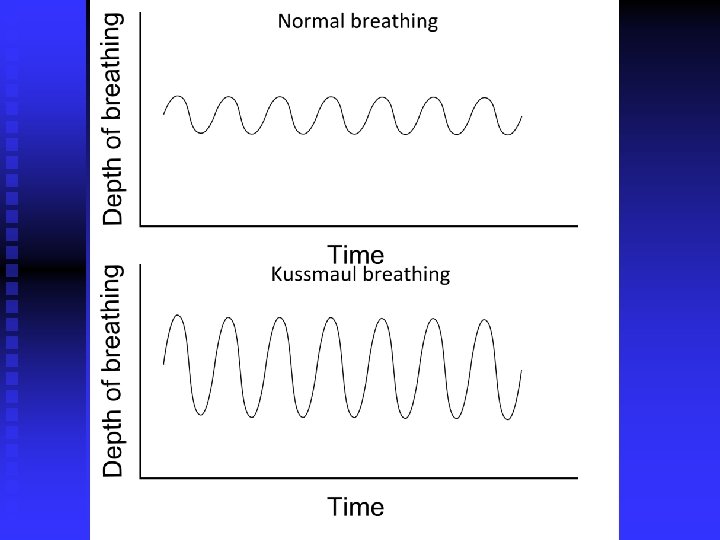
Bradypnea metabolic alkalosis n central nervous system depression. n hyperpnea and hypopnea refer to abnormally deep or shallow respirations. n

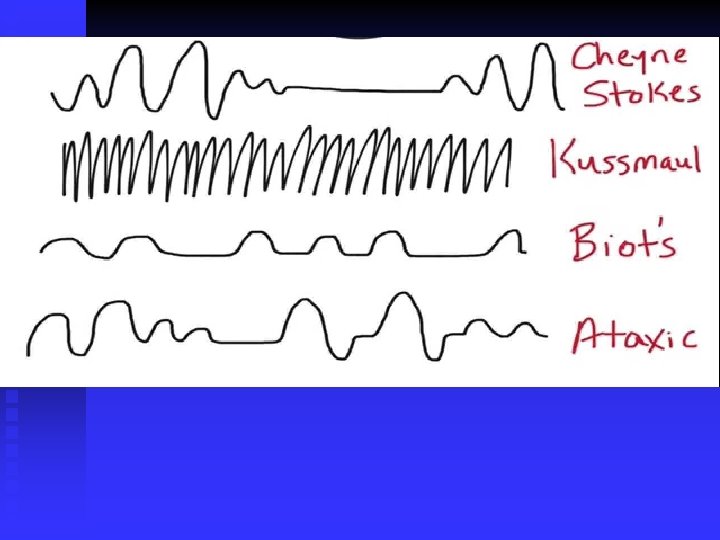
Rhythm of breathing n n • periodic breathing: u Occur during the first 3 months of life. u Respiratory pauses of less than 6 seconds u pauses occur in groups of three or more that are separated by less than 20 seconds of respiration. Apnea with cessation of air flow lasting more than 15 seconds is uncommon and may be accompanied by bradycardia and cyanosis. Kussmaul breathing in diabetic ketoacidosis.

n Biot breathing consists of irregular cycles of respiration at variable tidal volumes interrupted by apnea and is an ominous finding in patients with severe brain damage.

CHEST WALL STRUCTURE n n Contour Symmetry Hyperinflation Spinial deformity: u Kyphosis u Gibbus u Lordosis u Scoliosis

Sternal deformity: Pectus Carinatum, Pectus Excavatum

clinical signs of respiratory distress n n n Retractions: intercostal and subcostal tissues and the supraclavicular and suprasternal fossae. alae nasi. Visible contraction of the sternocleidomastoid muscles and indrawing of supraclavicular fossae during inspiration In young infants, these muscular contractions may lead to head bobbing. Older patients with chronic airway obstruction and extensive use of accessory muscles may appear to have a short neck because of hunched shoulders.

Palpation Identify any area of tenderness or deformity n Assess expansion and symmetry of the chest n Assess the size and position of apex beats n make sure that the patient is in a straight position, and deformities (e. g. , scoliosis) should be taken into account. n

Percussion

Percussion n n Hyper extended the middle finger of hand place the distal interphalangeal joint FIRMY against the patients chest. With the end(note the pad) of the opposite of middle finger and use a quick flick of the wrist to strike first finger. Categorize what you hear (Compare) as normal, Dull and hyper resonant. Lung percussion is usually dull in restrictive lung disease and tympanitic in obstructive disease limited value in small infants because it cannot discriminate between noises originating from tissues that are close to each other

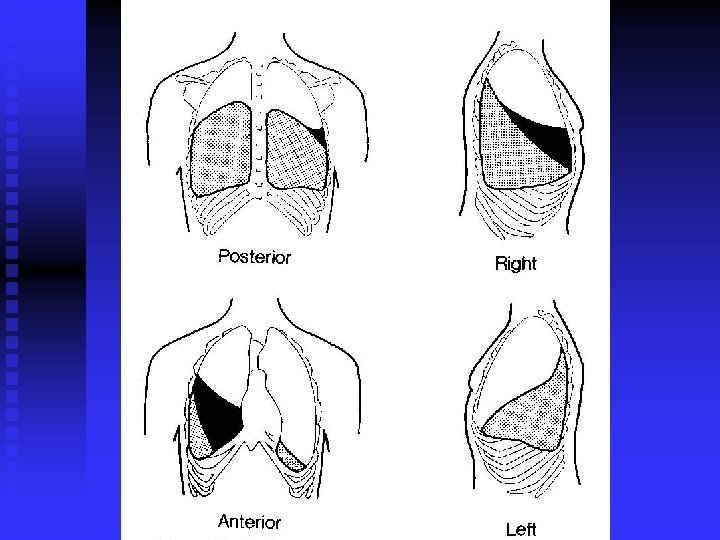
Percussion of the posterior chest n n n Percuss from side to side and top to bottom using the pattern showing in the picture. Omitting the area covered by the scapula. Compare one side to the other looking for asymmetry. Note the location of any abnormal percussion sound you hear.

Percuss. Anterior Chest n n n Percuss from side to side and top to bottom using the pattern showing in the picture Compare one side to the other looking for asymmetry. Note the location of any abnormal percussion sound you hear.

Percussion Notes and Their Meaning Flat or Dull Pleural Effusion or Lobar Pneumonia n Normal Healthy Lung or Bronchitis n Hyperresonant Emphysema or Pneumothorax n
 n n n Auscultate from side to side and top to bottom")
Auscultation(Post. view) n n n Auscultate from side to side and top to bottom using the pattern showing in the picture. Compare one side to the other looking for asymmetry. Note the location of any abnormal auscultation you hear.
 n n n Auscultate from side to side and top to bottom")
Auscultation(anterior view) n n n Auscultate from side to side and top to bottom using the pattern showing in the picture. Compare one side to the other looking for asymmetry. Note the location of any abnormal auscultation you hear.

Vesicular Bronchial
 Lung Sounds n Crackles These are high pitched, discontinuous sounds similar to")
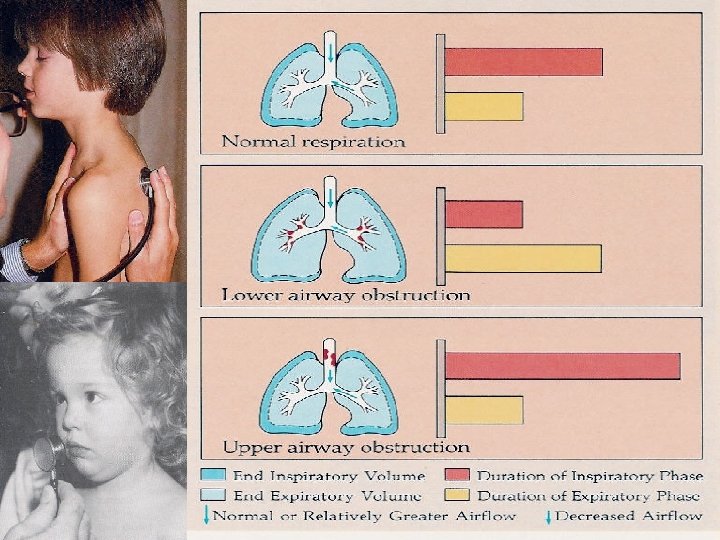
Adventitious (Extra) Lung Sounds n Crackles These are high pitched, discontinuous sounds similar to the sound produced by rubbing your hair between your fingers. (Also known as Rales) n Wheezes These are generally high pitched and "musical" in quality. Stridor is an inspiratory wheeze associated with upper airway obstruction (croup).

Diaphragmatic Excursion 1. 2. 3. Find the level of the diaphragmatic dullness on both sides. Ask the patient to inspire deeply. The level of dullness (diaphragmatic excursion) should go down 3 -5 cm symmetrically.

Don’t forget to listen to the heart n n n Listen at the right 2 nd interspace near the sternum (aortic area). Listen at the left 2 nd interspace near the sternum (pulmonic area). Listen at the left 3 rd, 4 th, and 5 th interspaces near the sternum (tricuspid area). Listen at the apex (mitral area). Record the rate, rhythm, and any extra sounds you hear.

Voice Transmission Tests n n These tests are only used in special situations. All these tests become abnormal when the lungs become filled with fluid Tactile Fremitus u Ask the patient to say "ninety-nine" several times in a normal voice u Palpate using the ball of your hand. u You should feel the vibrations transmitted through the airways to the lung. u Increased tactile fremitus suggests consolidation of the underlying lung tissues. Bronchophony u Ask the patient to say "ninety-nine" several times in a normal voice. u u Auscultate several symmetrical areas over each lung. The sounds you hear should be muffled and indistinct. Louder, clearer sounds are called bronchophony.

n n Whispered Pectoriloquy u Ask the patient to whisper "ninety-nine" several times. Auscultate several symmetrical areas over each lung. u You should hear only faint sounds or nothing at all. If you hear the sounds clearly this is referred to as whispered pectoriloquy. Egophony u Ask the patient to say "ee" continuously. u Auscultate several symmetrical areas over each lung. u You should hear a muffled "ee" sound. If you hear an "ay" sound this is referred to as "E -> A" or egophony.

The Problem List At the end of the history and physical examination make a problem list n Each problem may need differential diagnosis, investigation and/or therapy. n
- Slides: 52