Epilepsy comorbidities ges in epilepsy management By Gharib

Epilepsy co-morbidities ges in epilepsy management By Gharib Fawi Mohamed Professor Of Neurology Sohag Faculty Of Medicine Egypt

Agenda 1 - Epilepsy co-morbidities Cognitive impairment Mood & psychiatric disorders Cardiovascular, respiratory, metabolic Endocrinal changes Poor physical fitness Drug related weight gain Higher risk of bone fracture & decreased BMD Sleep disorders Migraine

How important is the problem? * Epilepsy is a chronic disorder that may need life time treatment in special situations * Epilepsy is more than seizures, an ongoing epileptogenic process can irreversible damage the brain →Mental health problems which may persist even with seizure freedom * Epilepsy interacts with many aspects of health, can cause both morphological and functional changes within the brain as well as cognitive and neuropsychological alterations

How important is the problem? * Most cases of epilepsy begin in childhood → time that is essential to development of basic cognitive skills * Uncontrolled seizures impair cognitive functions with effects being most sever in infancy & early childhood → need for early aggressive treatment & siezure control in those pts * Deficits in cognition are identified by epileptics & their familes as a significant and one of the most important comorbidities * As for the diagnosis of cognitive impairment at epilepsy onset, it is not sufficient to ask the patients, because they tend to underreport problems, which become evident with testing.

How important is the problem? - Tolerability of AED is more important to pts than seizures reduction - In chronic epilepsy the pt focus shifts from seisure control to side effects of AED & comorbidities - Cognitive side effects are the most important tolerability problems in chronic AED - Poly therapy ↑rate of co-morbidities - Chronic AED use ↑rate of co-morbidities

How important is the problem? -Patients with epilepsy frequently report some subjective impairment in cognitive functioning, with prevalence rates ranging from 44% for difficulties in learning and psychomotor retardation to 59% for sleepiness or tiredness. In addition, 63% of patients perceive that AEDs prevent them from achieving activities or goals. -Epilepsy Res. 68(1), 63– 67 (2006). -CNS Drugs 23(2), 121– 137 (2009).

How important is the problem • - 1 st drug trial→ 49% seizure free • • • - 2 nd drug trial→ additional 13 % seizure free - 3 rd drug trial add only 4 % seizure free - Significant benefit from other drugs is 10% or less - Each failure of AED trial→ risk of DRE↑ -20%of 1 ry GTC &60% of focal epilepsy develop DRE • Drug failure→failure of drug adherence→ • ↑epilepsy co morbidities

Cognitive Disorders & Epilepsy Outline: - Definition of Cognition - Aspects of cognition - Cognitive effects of Epilepsy - Cognitive effects of Antiepileptic Medications - How to deal with these effects

Cognitive Disorders & Epilepsy What is Cognition ? The capacity of the brain to process information accurately and to program adaptive behaviour This includes *focus attention, *remembering, memorize information *producing and understanding language, *solving problems, *making decisions Also can include *emotional problems like depression and anxiety * On higher level ►dealing with complex situations creatively by transcending from immediate circumstances to future act

Cognitive Disorders & Epilepsy - Aspects of cognition 1 - Memory problems 2 -Attention & concentration deficits 3 - Executive function deficits 4 - Language deficits:

Aspects of cognitive Disorders Memory problems: - The most important complaint - People with epilepsy may forget how often they forget - More observed with mesial temporal lobe focus (TLE) - More with focal epilepsy - Verbal deficit → dominant hemisphere - figural deficit → non dominant hemisphere - Bilateral temporal lobe epileptic foci → generalized momory impairments affecting all aspects of momory - Personal semantic momory usually remain intact (Epilepsia, 47, 615 -635, 2006)

Aspects of cognitive Disorders Attention & Concentration deficits - Selective attention, concentration, focus attention are important for proper many tasks of life - Deficits in attention are common in epilepsy and may affect other aspects of cognition → more with frontal epilepsies (attention) → more with complex partial seisure (sustained conc. ) → more with children & younger pts - In a study published in J of seisure 1992, found that 30 % of newly diagnosed adults with epilepsy with no brain lesions had deficits in sustained attention and mental flexibilty - ↑ risk of ADHD with range from 17 -58% ( pediat Neurol, 2005, 32 -1 -10, Child Neurol, 2006, 45, 50 -54 )
frontal")
Aspects of cognitive Disorders Executive function deficits: → more with frontal epilepsies - Pre)frontal lobe dysfunction is responsible for disturbances in executive functions by direct dysfunction (epilepsy focus) or indirect due to the seizure spread. - Frontal lobes seem to be the preferred target of ictal and interictal spreading of focal epilepsy as well as idiopathic generalized epilepsies. - Frontal lobe excutive functions, usually develop through adolescence. These facts together could explain that attention and executive function deficits are impaired whatever the syndrome, especially in younger patients. (Seisure, 2006, 15, 4, 227 -234)

Aspects of cognitive Disorders Language deficits: - Children tend to be more impaired than adults. - More common language problems are poor lexical knowledge, word-finding difficulties and anomia. reading and spelling are also affected. - More with higher interictal spike frquency , more with (ESES) → CSWS, LKS, MRE , - More with temporo-posterior seizure involvement . (Seisure, 2006, 15, 4, 227 -234)

Cognitive Disorders & seizures Which comes first? Before → shared underlying abnormality, Or After → seizures & AED Or Both NB. 25% of children with new-onset idiopathic epilepsies needed support from special education services before the onset of seizures. Similarly, some adults with new-onset epilepsy already show cognitive and behavioural disturbances, (Lancet, 2012; 380: 1180 -92)

Cognitive Disorders & seizures Which comes first? A total of 247 untreated patients with newly diagnosed epilepsy Underwent a brief test battery focusing on attention nd executive functions and memory. and executive functions and memory. �Impairments in attention and executive funct func were seen in 49. 4 % of the patients and memory deficits in 47. 8 %. (J Neurol (2012) 259: 1727– 1731)

Cognitive Disorders & seizures Which comes first? NB. Children with absence epilepsy have a high rate of Pre-treatment attentional deficit That may persist despite seisure freedom ►a threat To academic achievement (Neurology, oct. 29, 2013)

Cognitive Disorders & seizures Which comes first? Now there is increasing evidence that cog. problems often exist From the beginning resulting from synergestic effects between initial & later acquired lesions (J Neurol Neurosurg Psych, 84, 2013)
")
Cognitive Disorders & seizures - Causes (seizure related, pt. related & drug related ) * Static & irreversible → Shared etiology * Dynamic & reversible - Seizure itself - AED side effects - Interictal epileptiform discharge ( Neurology, 81, july, 2013, Epilepsy, june, 2013) NB. Cognitive dysfunction in epilepsy is multifactorial in origin, with multiple variables being involved, including epilepsy-related, antiepileptic drug-related and patientrelated variables, (Future Neurol. 2015; 10(1): 41 -48)

Cognitive Disorders & seizures - Higher cog. functions are more vulnerable to seizure effects: * Seizure types, EEG findings, age at onset, severity, chronicity, prognosis, anatomical location and etiology are the principal epilepsy related aspects where each of these parameters may affect cog. * Poly fits, frequent, serial fits, status epilepticus, poorly controlled fits, TLE, malignant epilepsy↑cog. disorders - More severe seizures , longer duration, late age of onset→ long term damage→hipocammpal , thalamic atrophy& hypo metabolism , Neuronal cell loss(epilepsia, june, 6, 2016) - More common in learning age child & elderly- More common in children born of epileptic mother

Cognitive Disorders & seizures * Around 10 % of people with chronic epilepsy, some of whom were younger than 40 years of age, showed senile plaques. * Further more, plaques formed more rapidly in people with chronic epilepsy than in the general population, especially in those patients expressing the epsilon 4 allele. * Other studies link epsilon 4, which encodes apolipoprotein E 4, with an increased risk of Alzheimer’s disease and cardio vascular conditions. ) (Epilepsia, 2008; 49: 731 -40)

Cognitive Disorders & seizures Patterns of impairment The pattern of cognitive impairment depends on the pathophysiology underlying the seizure disorder. TLE Seems to arise in the hippocampus and mesial temporal lobe, and typically produces anterograde memory loss. , the extent and site of hippocampal atrophy seems to predict the severity and form of the memory impairment. People who are left-dominant for language, atrophy of the left hippocampus typically translates into impaired verbal learning and memory. Atrophy of the right hippocampus is, in general, associated with defective non-verbal learning and memory

Cognitive Disorders & seizures Petit Mal epilepsy Changes in the thalamocortical network seem to underlie childhood absence epilepsy, which is characterised by impaired attention as well as defective linguistic abilities, executive functions and social competences Benign. Rolandic epilepsy • Dysfunction of the Sylvian and Rolandic regions of the brain seems to produce benign epilepsy with centrotemporal spikes, which is commonly associated with impaired linguistic abilities. However, patients may also show mildly impaired attention and executive functions. (Epilepsia, 2012, 53, 1690 -, Lancet, 2012, 380, 1180)

Cognitive Disorders & seizures JME Neuropsychological testing reported subtle dysfunctions in verbal fluency, comprehension, expression, nonverbal memory & mental flexibility Structural& diffusion tensor MRI reported reduction in gray matter volume in the supplementary motor area (predicted defects in word naming tasks&expression scores) and in the posterior cingulate cortex (predicted cong. inhibition scores on bility tasks, (Neurology, 4, 76, 2011)

Cognitive Disorders & seizures In fact, a progressive cognitive deterioration in epilepsy are limited to a specific epilepsy syndromes, (mesial temporal lobe epilepsy and epileptic encephalopathies ) - juvenile myoclonic epilepsy ►executive dysfunction; - - Unverricht–Lundborg disease ►short-term visuospatial memory dysfunction, executive dysfunction and frontal lobe dysfunction; - - Landau–Kleffner syndrome ► language dysfunction - Dravet syndrome and Rett syndrome ►, poor language acquisition and visuospatial defects. Even ‘benign’ epilepsies, such as benign epilepsy of childhood with centrotemporal spikes or benign occipital epilepsy, seem to be characterized by a specific pattern of cognitive dysfunction. Epilepsia 55(8), 2014, Epilepsia 54(Suppl. 8), 14– 21 (2013).

Cognitive Disorders &IED I ED → Affect brain network activity → cognitive impairment • (prolonged reaction time, misperception of visual stimuli) * Normalization of EEG is needed even with seizure free pts ? ? → It seems now evident that the persistence of epileptic discharges during sleep interferes with cognitive development and cognitive functioning, representing one of the main reasons for progressive cognitive impairment in those patients, (Future Neurol. 2015; 10(1): 41 -48, )

Cognitive Disorders &IED NB. EDs have negative impact on cognition independent of focal brain lesions, and additive effects documented for frequent & bilaterally distributed IEDs as will as sleep induced IEDs ( epilepsia, september, 9, 57, 2016)

Cognitive disorders &AED - AED may have +ve as well as – ve effects on cognition - All AEDs can impair cognition , many of these side effects are modest The risk ↑ with - Classical 1 st generatio AED – Rapid titration - Large doses & ↑AED blood levels - Poly therapy-Tow used AED with mild cognitive effects →may induce serious cognitive disorders NB. with 1 st generation AED → no cognitve difference level between commonly used drugs , while with newer agents vary widly by specific drug (contiuum, 2016, 22(1) 191 -203)

Cognitive disorders &AED - It is recognized that AEDs potentiating GABAergic neurotransmission have more detrimental effects on cognitive functions than those modulating voltagegated channels - For most drugs, side effects occur early and for a short period , after which normalization occurs. - As with all drugs, cognitive adverse effects are dose dependent in the majority of cases. ►data on plasma levels should always be taken into account when discussing the impact of AEDs on cognition

Cognitive Disorders &AED NB: Definite evidence of drug-induced cognitive impairment has been established for: 1 - PB→momory impairment(short term memory, visuomotor memory & IQ impairment) 2 - PHT → mental slowing(memory, mental speed &attention) 3 -Topiramate → mental slowing (impairment of verbal functions, mental speech, psychomotor slowing&dysphasia)

Psychiatric and Behavioral Side Effects of New AEDs (Weintraub et al. Epilepsy & Behav 2007: 105 -110) 221 of 1394(16%) patients experienced PSEs Average rate of AED-related PSEs for a single AED : 8. 4% 6. 1% resulting in dosage change 4. 3% resulting in AED discontinuation Past history of psychiatric illness was the most significant predictor of PSE – (23% vs 12%)

Con. Vagran and Oxaleptal
 is a broad spectrum AED approved worldwide")
Convagran ( Zonisamide ) is a broad spectrum AED approved worldwide

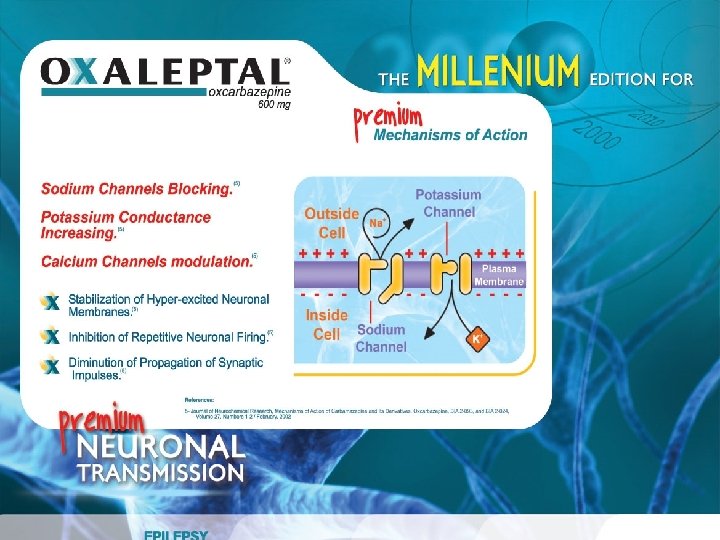
Con. Vagran mode of action 1. Blockage of voltage sensitive Na channels. 2. Blockage of voltage dependent T-type calcium channels. 3. Reduction of glutamate–mediated synaptic excitation. 4. Increase γ-amino butyric acid (GABA) via : - Increase release from the hippocampus and - Decrease re-uptake by suppress transporter enzyme Also , work by other mechanisms? ?

Efficacy of zonisamide • The current overview of ZNS use and effectiveness is based on both a long-term prospective postmarketing survey and current zonisamide use , data were collected from individual physicians and 23 survey groups throughout Japan, assessed the effectiveness of ZNS in 1631 patients. • ZNS was highly effective for treating partial seizures, with 70% of patients reporting improvement. More than half of patients with generalized seizures (58%) and half of patients with myoclonic and atypical absence seizures showed improvement with zonisamide treatment. ( seisure, 2004, 135, 541 -548 ) • ZNS was effective, well tolerated and significantly improved myoclonus- dystonia ( Neurology, may, 3, 86, 2016. )
 A pooled")
Zonisamide in Elderly with Epilepsy. (Acta Neurol Scand 2013: 128: 422 -428) A pooled analysis of ZNS therapy (add-on/monotherapy) between elderly (n=95) and adults (N=1389) No significant differences in safety/tolerability between the elderly and the adults patients No AEs specific to elderly

Convagran indications Monotherapy in the treatment of partial seizures, And generalized seizures ( Myoclonic, absence, and GTC), in adults and children aged 6 y. Adjunctive therapy in the treatment of adult patients with partial seizures, with or without secondary generalization in adults and children aged 6 y. Monotherapy or Add-on in patients with Generalized Epilepsy ( TC, Myoclonic and absence seizure)

How is Con. Vagran used ? • When Con. Vagran is used in newly diagnosed adults, the recommended starting dose is 100 mg once a day for two weeks, which may be increased by 100 mg at intervals of two weeks. The usual maintenance dose is 300 mg a day. • When Con. Vagran is used as an ‘add-on’ to existing treatment in adults, the recommended starting dose is 25 mg twice a day. After one week the dose may be increased to 50 mg twice a day and then further increased in steps of 100 mg every week, depending on the patient’s response. • The usual maintenance dose is between 300 and 500 mg


The exerted effect on QOL

In a recent study published in journal of • Neurology 29 September 2015, mindfulness-based therapy a form of short-term psychotherapy based on mental meditation (mind-body approach) was associated with greater benefits than social support alone in QOL, mood, seisure frequency, and verbal memory, where this form of therapy can help epileptic pts to address and accept all seisure –related comorbidities including physical and psychological symptoms(Neurology, 85, 13, Sept. 29, 2015)

Role of neurologists in psychiatric management of patients with epilepsy As a neurologists, we tend to focus on seizure control, and psychiatric co morbidities are often underestimated. Recognizing psychiatric manifestations is an area that needs improvement. Once symptoms are identified, the following questions arise : 1 -Are the symptoms related to the occurrence of seizures (preictal, postictal, interictal)? 2 -Are the symptoms related to AEDs? 3 -Is the onset of symptoms associated with the remission of seizures in patients who had previously failed to respond to AEDs?

Take a home message * Efforts should be done at every clinic visit to screen for common co morbidities that have significant adverse effects on health & epilepsy * The top co morbid conditions in epilepsy are cognitive & psychiatric disorders →recently emerged as an important priority for proper treatment of epilepsy * Early and complete seizure control and EEG normalization is mandatory to prevent developmental and cognitive disorders * Both physians &health care providers have an important role in improving quality of life of their pts even with uncontrolled seizures

Take a home message * Therapy & polytherapy in particular , need to take the cog. side effects of AED in consideration * Both physians &health care providers have an important role in improving quality of life of their pts even with uncontrolled seizures * Patients appear to underreport cognitive deficits. Thus, a routine application of a brief standardized neuropsychological screening before the initiation of a pharmacological treatment would be appreciated to provide a baseline to evaluate subsequent treatment success, to eventually initiate countermeasures, and to monitor the course of the disease


Epilepsy co-morbidities nges in epilepsy management By Gharib Fawi Mohamed Professor Of Neurology Sohag Faculty Of Medicine Egypt

Agenda 1 - Epilepsy co-morbidities Cognitive impairment Mood & psychiatric disorders Cardiovascular, respiratory, metabolic Endocrinal changes Poor physical fitness Drug related weight gain Higher risk of bone fracture & decreased BMD Sleep disorders Migraine

How important is the problem? * Epilepsy is a chronic disorder that may need life time treatment in special situations * Epilepsy is more than seizures, an ongoing epileptogenic process can irreversible damage the brain →Mental health problems which may persist even with seizure freedom * Epilepsy interacts with many aspects of health, can cause both morphological and functional changes within the brain as well as cognitive and neuropsychological alterations * Uncontrolled seizures impair cognitive functions with effects being most sever in infancy & early childhood → need for early aggressive treatment & siezure controll in those pts

How important is the problem? - Tolerability of AED is more important to pts than seizures reduction - Cognitive side effects are the most important tolerability problems in chronic AED - Poly therapy ↑rate of co-morbidities - Chronic AED use ↑rate of co-morbidities

How important is the problem • - 1 st drug trial→ 49% seizure free • • • - 2 nd drug trial→ additional 13 % seizure free - 3 rd drug trial add only 4 % seizure free - Significant benefit from other drugs is 10% or less - Each failure of AED trial→ risk of DRE↑ -20%of 1 ry GTC &60% of focal epilepsy develop DRE • Drug failure→failure of drug adherence→ • ↑epilepsy co morbidities

Epilepsy& common co-morbidities Mood & psychiatric disorders NB • AED which modify the balance between normal excitation &inhibition through their effects on neurotransmitter system &/or ion channel activities , → at the same time may modify systems which regulate mood and behavior • The preexisting mental state of the pt is very important predicting factor • Adverse mood effects of AED are often not recognized? ? • Psychiatric adverse events are usually reversible

Risk factors of psychiatric Aspects -Patient related factors Psychosocial stress&state Structural brain lesions Seizure related brain dysfunction Genetic predisposition -Seizure related factors Seizure type, severity, duration, … etc -AED related factors Polytherapy Psychotropic effects DD interaction Dose dependant Idiosyncratic Drug titration, withdrwal
→ play a major role, , where")
Depression as a co-morbidity -Neurotransmitters changes (mainly serotonin)→ play a major role, , where both epilepsy &DD have ↓ serotonin receptor binding, (Neurology, 80, april, 1465, 2013) - Others, as, Noradrenaline, GABA, Glutamate play a role Anti-Dep may→provoke seizures , or may act as AED * Tricyclic → 1 st epileptogenic 15% * Tetracyclic → may cause but less New anti-dep eg, SSRI, SNRI → more save&may act as AED * Four antidepressants can cause seizures at therapeutic doses: clomipramine, maprotiline, amoxapine, and bupropion, although the evidence of the latter is still the subject of debate. (Epilepsia, 14 jan, 2016 )

Depression as a co-morbidity Both D. D and epilepsy have: Hippocampal atrophy - Changes in structure of amygdala - Programmed cell death in hippocampal formations - Abnormalities on imaging Positron Emission Tomography - 5 HT-1 A (serotonin 1 A) receptor binding decreases in frontal, temporal, and limbic cortex in both depression and Temporal Lobe Epilepsy (Neurology , April, 16 , 2013) -

Mood disorders in epilepsy Mood disorders General population Epileptic population Major Depression 2 -4% 11 -60% Anxiety disorders 2. 5 -6. 5% 19 -45% Psychosis 0. 5 -0. 7% 2 -8% 2 -10% 25 -30% ADHD

Depression as a co-morbidity • • The commonest co-morbidity , up to 60% AED & Antidepressants →a reciprocal interaction Epilepsy is 2 -7 times in pts with depression Epilepsy & dep. → bidirectional relation not only PWEat greater risk of developing these two psychiatric comorbidities, but patients with these psychiatric disorders have a twofold to sevenfold higher risk of developing epilepsy • Systematic reviews support an increased prevalence of depression in patients with epilepsy and suggest that a broad biopsychosocial approach is necessary to better understand the factors associated with depression. (14 JAN 2016, epilepsia)

Depression as a co-morbidity Comorbid depression has a range of adverse consequences - Decreased quality of life, - Diminished medication adherence, - Poorer treatment outcomes, - Increased health service use, - Increased cognitive complaints, - Increased risk of other chronic diseases such as cardiovascular disease, and suicide. However, the risk factors that contribute to this important comorbidity remain uncertain. Better identification of these factors is needed to advance treatment and prevention of depression in patients with epilepsy. (14 JAN 2016, epilepsia)

What Is Unique about Depressive Episodes in Epilepsy? In PWE, psychiatric symptoms and/or episodes are typically classified according to their temporal relation with seizures into two major classes: Interictal and periictal, Periictal►subclassified into preictal , ictal or postictal Postictal episodes can occur (immediate postictal episode), or (delayed postictal period). Clinically, however, interictal and periictal episodes may be identified in the same patient. The need to recognize the type of depressive episode is of the essence as the type of treatment differs for interictal and periictal depressive episodes. Indeed, total seizure remission is required for suppression of periictal events, whereas interictal depressive episodes may require pharmacotherapy with psychotropic drugs and/or psychotherapy. (14 JAN 2016, epilepsia)

Anxiety Disorders. The Forgotten Psychiatric Comorbidity # Anxiety Disorders is the second psychiatric co-morbidity # Comorbid anxiety disorders severely affect daily living and quality of life in patients with epilepsy # Evidence suggests that the abnormal functioning of GABA receptors could be of great importance in the pathophysiology of epilepsy and anxiety disorders # The highest rates of psychiatric comorbidities, including anxiety, are reported in patients with chronic, refractory seizure disorders

Anxiety Disorders as a co-morbidity # The risk of anxiety is higher in focal (more frequent in . temporal lobe) epilepsy than in generalized epilepsy # Anxiety in patients with epilepsy can be preictal, postictal, or interictal # Interictal anxiety has a great influence on the quality of life of patients, since most of them have a permanent fear. (Epilepsy Curr. May-Jun, 2011)

Mechanisms of psychotropic effects of AED 1 -Dose –dependant toxicity 2 - dose independent idiosyncratic drug effects 3 - withdrawal effects 4 - AED effect (forced normalization )

Idiosyncratic AED effects include 2 main recognized mechanisms 1 -GABA ergic AED effects →anxiolytic, sedating, antimanic, but → depressogenic (barbit, topiramate, vigab. , tiagabin, valp) 2 -Anti-glutamatergic drugs→antidepressive vating, but → anxiogenic, insomnia (felbamate, lamotrigine)

NB - PB→ provoke ADHD, irritability, &aggressive behavior - PHT→ may provoke schizoph. like psychoses with high serum levels - Topiramate, tiagabine, vigabatrin → High frequency of dep.

Psychotropic effects of AED +ve Psychotropic effects -ve Psychotropic effects Barbiturates Sedative Aggression, Depression Benzodiazepines Sedative , Anxiolytic Withdrawal syndromes Ethosuximide - Insomnia Phenytoin - Toxic schizoph. psychosis Carbamazepine Mood stabilizing, impulse control Valporate Mood stabilizing anti manic Vigabatrin - ? ? Depression Aggression, Depression, withdrawal Lamotrigine Antidepressant Insomnia Felbamate ? Stimulating Agitation ? Gabapentin Anxiolytic, Antidepres ? Rarely aggression in children Tiagabin - Depression Topiramate - Depression

Role of the neurologist in the psychiatric management of patients with epilepsy As a neurologists, we tend to focus on seizure control, and psychiatric co morbidities are often underestimated. Recognizing psychiatric manifestations is an area that needs improvement. Once symptoms are identified, the following questions arise : 1 -Are the symptoms related to the occurrence of seizures (preictal, postictal, interictal)? 2 -Are the symptoms related to AEDs? 3 -Is the onset of symptoms associated with the remission of seizures in patients who had previously failed to respond to AEDs?

In a recent study published in journal of • Neurology 29 September 2015, mindfulness-based therapy a form of short-term psychotherapy based on mental meditation (mind-body approach) was associated with greater benefits than social support alone in QOL, mood, seisure frequency, and verbal memory, where this form of therapy can help epileptic pts to address and accept all seisure –related comorbidities including physical and psychological symptoms(Neurology, 85, 13, Sept. 29, 2015)

Take a home message * Efforts should be done at every clinic visit to screen for common co morbidities that have significant adverse effects on health & epilepsy * The top co morbid conditions in epilepsy are cognitive & psychiatric disorders →recently emerged as an important priority for proper treatment of epilepsy * Early and complete seizure control and EEG normalization is mandatory to prevent developmental and cognitive disorders * Both physians &health care providers have an important role in improving quality of life of their pts even with uncontrolled seizures


Medication adherence & compliance - Adherence problems - Choice of AED - Therapeutic strategy in epilepsy treatment - How to avoid drug failure

Medication adherence problems poor compliance Why it is important * may affect 30 -50%of pts * One of the most common causes of drug failure Adherence related problems. Memory impairment. Psychiatric disorders. Adverse events. Instructions of use , dosing regimen. Unsatisfactory doctor-pt relationship NB. All these problems→ ups & down

How we can improve compliance 1 -Good selection of AED 2 -Minimize No of prescribed AED 3 -Simplify dose regimen 4 -Good doctor-pt. relationship

Which drug to choose The optimum chosen drug must depend on the following: 1 - Seizure profile(type, frquency, severity, …) 2 - Pt. profile(age, sex, metabolic state, occupation, comorbid conditions, life style…) 3 - Drug profile(efficacy, toxicity , adverse events interaction, tolerability, mode of action, cost, ease of use, availability, dose regimen, hepatic enzyme effect, adherence, …. etc)

Advantages of broad-spectrum drugs * Higher probability of seizure control when syndromic diagnosis is in doubt * Simultaneous control of multiple seizure types * Less likely emergence of new seizure types * Lower probability of seizure aggravation

Main Mode of Action of AEDs and seizure efficacy spectrum AED Main Mode of Action Broad spectrum yes Carbamazepine Block voltage dependant Na channel No Clobazam Increase inhibition by GABA No Clonazepam Increase inhibition by GABA No Ethosuximide Block T type Ca channel No Gabapentin Multiple modifies Ca Channel and neurotransmitter release) No Lamotrigine Block voltage dependant Na channel Yes Levetiracetam vel binds to synaptic vesicle protein(SV 2 A) yes Oxcarbazpine Block voltage dependant Na channel No Phenobarbitone Multiple(↓Na; ↓Ca; ↑GABA; ↓Glutamate) yes Phenytoin Block voltage dependant Na channel No Tiagabine Increase inhibition by GABA No Topiramate Multiple(↓Na; ↓Ca; ↑GABA; ↓Glutamate) yes Valproate Multiple(↓Na; ↓Ca; ↑GABA; ↓Glutamate) yes Vigabatrin Increase inhibition by GABA Selective and irreversible GABA transaminase inhibitor thus increasing whole brain levels of GABA No zonisamide Multiple(↓Na; ↓Ca) yes Panayiotopoulos C. P. 2005

Efficacy of Main AEDs in Seizure Types AED Focal simple or complex Secondarily GTCS Primary GTCS Myoclonic Jerks Absence seizures Carbamazepine Effective Exaggerate Clobazam Effective? Effective? Clonazepam Effective? Exaggerate? Effective Ethosuximide Ineffective Exaggerate? Effective Gabapentin Effective Ineffective Exaggerate Lamotrigine Effective Exaggerate Effective Levetiracetam Effective Effective Oxcarbazpine Effective Exaggerate Phenobarbitone Effective Exaggerate? Phenytoin Effective Ineffective Exaggerate Tiagabine Effective Ineffective Exaggerate Topiramate Effective Effective? Valproate Effective Effective Vigabatrin Effective Ineffective Exaggerate Zonisamide Effective Effective? Panayiotopoulos C. P. 2005

Seizures and Syndromes Most Commonly Subject to Selective Aggravation AEDs Seizures Aggravated Barbiturates Absence, tonic Benzodiazepines ( i. v. use, Lennox-Gastaut syndrome and West syndrome) Carbamazepine, oxcarbazepine, phenytoin Absence, myoclonic, atonic, tonic Vigabatrin, tiagabine Absence, myoclonic Gabapentin, pregabalin Myoclonic Lamotrigine Many seizure types in severe myoclonic epilepsy of infancy (SMEI)

Can drug resistance in epilepsy be avoided or minimized or even reversed ? Yes through seven concepts: 1. Good understanding of → Antiepileptic drug selection. → Dose requirement. → Drug combination. → D. D interaction. 2. Failure to increase the dose to the highest tolerated limits → high proportion of drug resistant epilepsy.

3. Understanding the underlying mechanism of AED: • Pharmacodynamics, (efficacy, toxicity, interactions, dose and side effects). • Pharmacokinetics (absorption, plasma protein binding, half life and elimination). • Pharmacogenetics ( genotype, phenotype ) 4. Monitoring of AED serum levels. 5. Better management of epilepsy co-morbidities and QOL improvement → better seizure control and decrease drug resistance. 6. Use of MDR protein inhibitors e. g. . verapamil. 7. Successful epileptic surgery alone is not curative → we have to continue AED.

Treatment Algorithm For Medical Management of Epilepsy Months of treatment Patients with newly diagnosed, previously untreated epilepsy 0 Monotherapy (drug 1) 4 Success Failure Consider withdrawal after 2 - 5 years of complete seizure control Alternative monotherapy (drug 2) Success Failure Consider withdrawal after 5 years of complete seizure control Polytherapy (drug 1 and 2) Success Failure Consider withdrawal after 5 years (with patient considerations) Substitution and transfer to monotherapy with drug 3 Success Failure Consider withdrawal after 5 years (with patient considerations) Presurgical evaluation? Diagnostic re-evaluation 8 12 16 (Gram L & Schmidit D. 2000)

Discontinuing AEDs Take into account the following issues - Natural history of epilepsy - Probability of seizure free after withdrawal - Duration of seizure-free interval - Risk factors for seizure recurrence - Risk of long-term effects of AED - Possible changes in therapeutic efficacy of AEDs restarted after relapse

Discontinuation of treatment * If seizure freedom has been achieved for 2 -5 years, treatment discontinuation is an option except patients with epileptic syndromes and those with secondary brain lesions. * Seizure recurrence in adulthood is highest for JME (80% recurrence) vs 40 -50% for other subtypes. * 75% of relapses occur within first 12 months, and at least half of those relapses occur in the first three months. * No driving during tapering. Tapering should occur over 6 -10 weeks for all drugs except barbiturates and benzodiazepines, which probably should be tapered over 10 -16 weeks.

Take a home message * Efforts should be done at every clinic visit to screen for common co morbidities that have significant adverse effects on health & epilepsy * The top co morbid conditions in epilepsy are cognitive & psychiatric disorders →recently emerged as an important priority for proper treatment of epilepsy * Early and complete seizure control and EEG normalization is mandatory to prevent developmental and cognitive disorders * Both physians &health care providers have an important role in improving quality of life of their pts even with uncontrolled seizures

- Slides: 88