Northeast Regional Epilepsy Group Christos Lambrakis M D

Northeast Regional Epilepsy Group Christos Lambrakis M. D. 1

October 29 th, 2016 How is Epilepsy Diagnosed Recognizing Types of Seizures and Imitators of Epilepsy 2

3

Brain *Weight: 3 lbs *Made of 75% water * 2% of body weight * 20% of energy requirements *Contains 100 billion neurons *Each neuron has 1000 to 10, 000 synapses *100, 000 miles of blood vessels *Likes: Oxygen, Glucose, Cute cat videos

5

6

7

8

What is a Seizure? • A seizure is caused by abnormal electrical activity between cells of the brain (neurons) • A seizure can temporarily disturb many of the brains normal functions. • This abnormal electrical activity results in the clinical manifestations of the seizure. 9

What is a Seizure? • The clinical manifestations of the seizure are determined by the region of the brain where the abnormal electrical activity is located. • Clinical manifestations of a seizure are varied depending on the region of the brain involved. Examples include changes in movement, sensation, behavior or awareness. 10
 11")
EEG (Normal) 11
 12")
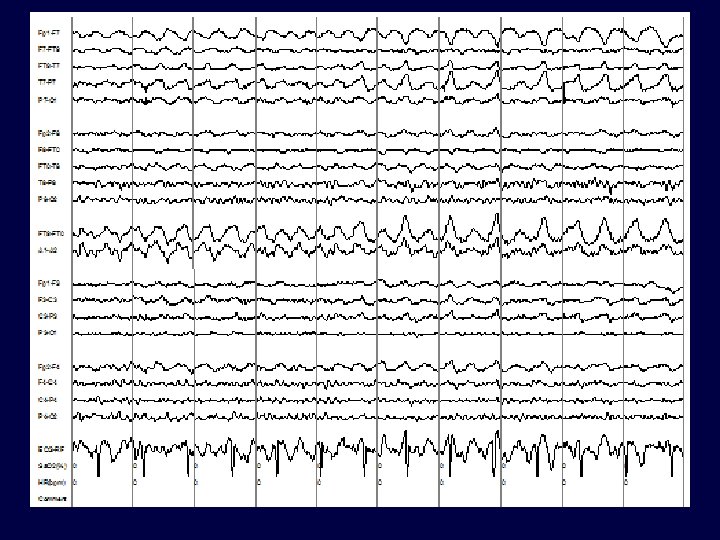
EEG (Seizure) 12

What is Epilepsy? • Epilepsy is the term applied to the state of recurrent seizures. • Epilepsy is a condition of the brain, of various causes, which predisposes the patient to recurrent epileptic seizures. • Epilepsy is a tremendously variable condition in terms of its cause, seizure types and response to treatment. 13

How is Epilepsy Diagnosed? 14

Epilepsy Diagnosis • Clinical description of the seizure events provides very important information. – What was seen? (Confusion, Loss of consciousness, Body movements, Head turning, Eye deviation, Right side/Left side or both) – What was felt by the patient? (At the start of the seizure (Aura) or as seizure evolves) • **Helps us to localize the seizure (where in the brain did it originate from).

Epilepsy Diagnosis • Precipitating factors: – Lack of sleep, fever, current illness, medications, flashing lights, hyperventilation. • Predisposing factors: – Past medical history (head trauma, stroke), Family history • **Helps us to better understand why the seizures occurred (Etiology). 16
 – General (Head size, dysmorphic features,")
Epilepsy Diagnosis • Physical Examination – Vitals (Fever) – General (Head size, dysmorphic features, skin lesions, stiff neck). – Neurologic Examination (Confusion, memory loss, speech difficulty, motor weakness, sensory loss) 17

Epilepsy Diagnosis • Acute Symptomatic Seizures • Chronic Symptomatic Seizures • Idiopathic Seizures 18
. –")
Epilepsy Diagnosis-Etiology • Acute Symptomatic Seizures (Seizures caused by a suspected acute reason). – Trauma (Head injury) – Metabolic (Electrolyte imbalance, Uremia) – Toxic (Ingestion, Medication) – Infectious (Meningitis, Encephalitis, Sepsis) – Vascular (Stroke, Hemorrhage) 19

Epilepsy Diagnosis-Etiology • Chronic Symptomatic Seizures (Seizures caused by preexisting conditions which favor the development of seizures). – Remote injury (Past head injury, Birth trauma) – Developmental (Cortical dysplasia) – Degenerative Disorders (Alzheimer’s) – Metabolic (Amino and organic acid disorders) 20
 – The cause of the seizures")
Epilepsy Diagnosis-Etiology • Idiopathic Seizures (Etiology is unclear) – The cause of the seizures cannot be determined from our current knowledge or conventional testing. – Approximately 50% of patients will fall under this category. 21

Epilepsy Diagnosis Diagnostic Studies • Blood work (Electrolytes such as Sodium, Potassium, Calcium; Glucose, Kidney and Liver function) • Electro-diagnostic (EEG) • Imaging (CT, MRI, SPECT, PET and MEG) 22
 23")
Electroencephalogram (EEG) 23

Electroencephalogram EEG • Represents a record of the small shifting brain electrical potentials from the surface of the brain recorded over the scalp. • As seizures are caused by a disturbance of electrical activity, the EEG is uniquely suited to further our understanding of a patients seizures.

Goals of Video-EEG Monitoring • Is it really an epileptic seizure? (Epilepsy vs. non-epileptic events) • What type of seizure is it? (Characterize epilepsy type) • Where does the seizure originate from? Is it focal? (i. e. does it come from one specific region? )

Electrodes 26

27

28

29

30

31

Video-EEG Monitoring • Long term inpatient monitoring allows for recording of seizure events. • Clinical and electroencephalographic features can be reviewed aiding in seizure characterization and localization. • Baseline EEG may be helpful in determining risk of future seizures.

Inpatient Video-EEG 33

Outpatient Ambulatory Video. EEG 34

Brain MRI • Provides a structural assessment of the brain. • We look for developmental abnormalities, strokes, tumors or scar tissue that could be focus for electrical irritation that could cause a seizure.

Brain MRI

Recognizing Types of Seizures 37

Seizure Classification • Two major categories: – Generalized – Partial 38

Generalized Seizures
 40")
EEG (Seizure) 40

Seizure Classification • Generalized Seizures Tonic/Clonic Absence Myoclonic Atonic Tonic

Generalized Seizures Tonic/Clonic • Electrically the entire brain is affected all at once. • Patients loses consciousness at the onset of the seizure. • Stiffening (tonic) and rhythmic jerking movements (clonic) follow. • Cyanosis, tongue biting and loss of bladder control are common.
.")
Generalized Seizures Absence • Results in a brief period of staring (5 -10 sec). • Patient is usually unaware of his surroundings. • Sometimes accompanied by eye blinking or chewing movements. • Prompt recovery. • Commonly seen in childhood and may be mistaken for day-dreaming.

Generalized Seizures Other Less Frequent • Myoclonic seizure: Brief jerk like contractions which can be localized or generalized. • Atonic seizure: Drop attacks 44

Partial Seizures Complex
 region of the brain. Depending")
Partial Seizures • Seizures originate from a specific (focal) region of the brain. Depending on what area of the brain is stimulated a variety of clinical presentations can occur. • Seizures are often stereotypic to the patient. • Examples include changes in awareness, sensation, rhythmic jerking or stiffening of a specific limb, visual hallucinations.

Partial Seizures • Can progress to a Generalized Tonic/Clonic seizure ‘Secondary Generalization’. • Often associated with aura. • Often associated with automatisms (coordinated involuntary, non-purposeful movements). Examples would include lip smacking, picking, rubbing etc. 48

Partial Seizures • Two Types: Simple and Complex • Simple Partial: No impairment of consciousness. • Complex Partial: Impairment of consciousness.

Partial Seizures Motor

Partial Seizures Complex

Generalized vs Partial Seizures • Sudden onset with no warning/aura • Symmetrical movements • Loss of consciousness • May begin with aura (subjective symptoms experienced by the patient) • Asymmetric or focal motor movements • Alteration of awareness. 52

Imitators of Epilepsy 53

Differential Diagnosis • Seizures can produce sudden neurologic symptoms. • Many diseases can produce sudden neurologic symptoms. • ** Many neurologic diseases can be mistaken for epilepsy and vice-versa. 54

Differential Diagnosis • Non-Epileptogenic events can be secondary to organic or psychogenic etiologies 55

Differential Diagnosis • How do we differentiate between events that are seizure related and those that are caused by a non-epileptic medical or psychiatric condition? • ** Capturing an episode on EEG and demonstrating abnormal electrical activity during the event. 56

Differential Diagnosis • In general episodes stemming from nonepileptic neurologic issues are NOT associated with EEG changes. • Caveats – Some partial seizures can remain electrical silent (i. e. not obvious on EEG). – Some neurologic diseases can cause changes on the EEG (Migraine, Syncope) 57
")
Seizure Imitators Loss of Consciousness • • • Cardiac (heart failure, heart attack, arrhythmias) Hypoglycemia (fasting, excess insulin) Hypovolemia (dehydration) Hypoxia (lung disease) Panic attack (vasovagal response) Syncope (orthostatic) 58

Syncope • Decreased delivery of oxygenated blood to the brain resulting in loss of consciousness. – Very common with many etiologies – Sudden and unpredictable – Recurrent – Stereotypic – Premonitory symptoms (nausea, sweating) – ‘Convulsive’-type movements 59
 – Inter-Ictal (between episodes) •")
Syncope Work-Up • Video-EEG monitoring – Ictal (during event) – Inter-Ictal (between episodes) • EKG/ Holter Monitor • Carotid Ultrasound • Tilt Table Testing 60
 • Endocrine (Hypo/Hyperglycemia, Thyroid Disease) •")
Seizure Imitators Confusion • Cerebrovascular (TIA, Stroke, TGA) • Endocrine (Hypo/Hyperglycemia, Thyroid Disease) • Migraine Headaches (complicated) • Metabolic (hepatic or renal encephalopathy 61
 • Panic")
Seizure Imitators Motoric or Behavioral Change • Movement Disorders (Tics, Tremors, RLS) • Panic Attacks • Sleep Disorders (Night terrors/ Sleep walking, Benign myoclonus, Sleep apnea) • Psychogenic Non-Epileptic Seizures (PNES) 62

Psychogenic Non-epileptic Seizures • Resemble epileptic seizures but lack EEG correlate. • Can mimic any type of epileptic seizures. • Very common (~25% of patients referred to Video-EEG monitoring for evaluation of intractable epilepsy). 63
 • Unconscious production")
Psychogenic Non-epileptic Seizures • Psychiatric manifestation – Somatoform/Conversion Disorder (most common) • Unconscious production of physical symptoms due to psychological factors. A psychological defense mechanism to keep internal stress out of conscious awareness. – Factitious Disorder • Consciously determined symptoms driven by a powerful unconsciously determined need. – Malingering • Willful production of symptoms for a specific external 64 incentive.

Psychogenic Non-epileptic Seizures • Often difficult to distinguish clinically from epileptic seizures. • Clues: – Resistance to AEDs – Emotional Triggers (stress) – Bilateral clonic movements without loss of consciousness – Absence of post-event confusion/lethargy. • Video-EEG is very helpful in diagnosis. 65
 –")
Psychogenic Non-epileptic Seizures • Many clinical patterns: – Migratory motor activity (most common) – Generalized motor activity – Unilateral (less common) – Alteration of awareness (Common) ** Can be difficult to distinguish from frontal lobe seizures. 66

Psychogenic Non-epileptic Seizures • Characteristics of PNES – Variable responsiveness or preserved awareness. – Out of phase movements of extremities. – Discontinuous motor activity – Pelvic thrusting. – Side to side head movements. – Eye closure/eye flutter 67

Psychogenic Non-epileptic Seizures • Characteristics of PNES – Varied character of events – Suggestibility – Emotional triggers – Prompt recovery (Absence of post-ictal state) – Poor response to anti-epileptic medications 68

Psychogenic Non-epileptic Seizures • Although such findings as urinary incontinence, tongue biting and injuries are often attributed to epileptic seizures they can also be seen in PNES. 69

Psychogenic Non-epileptic Seizures • ~20 % of patients with PNES will also have coexistent epileptic seizures. • Latency between manifestation of PNES and diagnosis is ~ 7 years. • Prompt diagnosis is crucial to avoid iatrogenic morbidity (Exposure to unnecessary medication ~80%, Intubation ~50%). 70
- Slides: 70