WOMEN WITH EPILEPSY MANORI WIJAYATH STAFF SPECIALIST NEUROLOGY


 • Pregnancy complications PIH, LSCS, premature labour, miscarriages, bleeding Seizure")









 orofacial defects, (cleft lip/cleft palate)")








- Slides: 23
WOMEN WITH EPILEPSY MANORI WIJAYATH STAFF SPECIALIST- NEUROLOGY
PREVALENCE OF EPILEPSY IN WOMEN • Commonest medical condition in pregnant female • USA- Year 2000, 3 -5 /1000 births are for WWE • Australia - 1500– 2000 women on AEDs become pregnant each year
WOMEN WITH EPILEPSY (WWE) • Pregnancy complications PIH, LSCS, premature labour, miscarriages, bleeding Seizure frequency and seizure freedom Management Medications medication related foetal complications • Lactation • Contraception
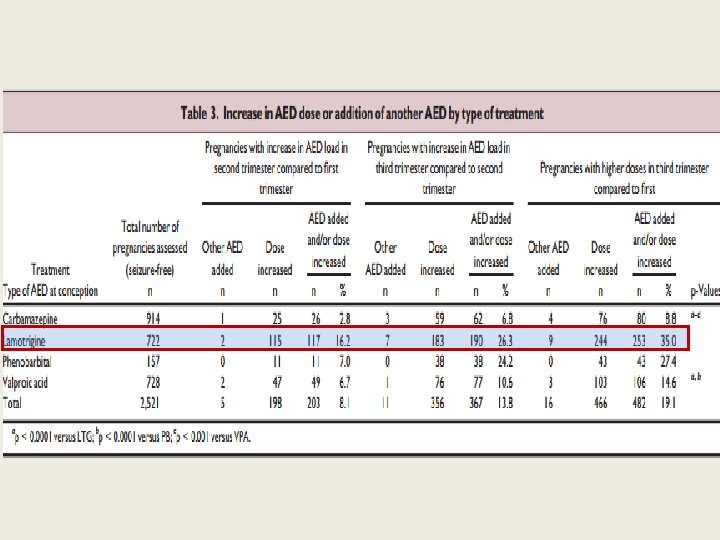
Seizure control and treatment changes in pregnancy: Observations from the EURAP epilepsy pregnancy registry Epilepsia, 54(9): 1621– 1627, 2013 • Prospective 3, 806 pregnancies of 3, 451 WWE on AEDs (monotherapy with CBZ, LTG, PB, VPA) Enrolment : 8. 9/40 (SD 3. 3) IGE: 39. 3%, Focal: 47. 01%, undetermined: 13. 6% • Sz Frequency Sz free: 66. 6% continuing: 33. 4% Sz freedom for at least 9 months prior to pregnancy - 84– 92% chance of remaining sz free 1 st vs 2/3 T Unchanged 70. 5% Reduction 12% Increase 15. 8%
DO WWE HAVE AN INCREASED RISK OF PREGNANCY-RELATED COMPLICATIONS? • Class I study (Viinikainen et al. , 2006)-n=179 Cesarean instrumental delivery Preeclampsia/ PIH No significantly increased risk of above BUT lack statistical precision to comment of an increased risk Premature contractions and premature labour and delivery Non smoking – no increase Smoking- substantial increase Spontaneous abortion- inadequate data
Perinatal foetal outcome with intrauterine AED exposure
Facts to remember in Rx *Altered pharmacokinetics- eg- pronounced decline in serum concentrations for AEDs eliminated by glucuronidation (UGT) *Adverse effects of AEDs on the foetus are dose-dependent (Meador et al. , 2009 a; Tomson et al. , 2011; Hernandez-Diaz et al. , 2012; ) *Aim at reducing GTCS- maternal and foetal morbidity and mortality *Review and possibly revise treatment well before conception *Titrate to the lowest effective dose before pregnancy (Harden et al. , 2009, Tomson & Battino, 2012)
free concentrations may be preferable in such situations- PHT, VPA (Johannessen & Tomson, 2006; Patsalos et al. , 2008) No Rx failures LTG, OXC, Variable, cannot predict (Tomson & Battino, 2007; Patsalos et al. , 2008 p. H, gastric emptying, intestinal motility
TREND Utilization of antiepileptic drugs during pregnancy: the EURAP registry -1999 -2005
LAMOTRIGINE • LTG clearance markedly increases in late pregnancy (Ohman et al. , 2008; Pennell et al. , 2008; Tomson et al. , 2013) § 55% protein bound § met by UGT decline markedly (50 -60%) Starts in T 1 marked in mid T 3 trimester § less pronounced when combined with VPA • Rapid return to pregnant level post delivery starts D 1 and completed in 2 to 3/52 postpartum
§ AEDs whose pharmacokinetic properties are affected, the extent variable between individuals. § Polytherapy makes it even more difficult to predict
What should we monitor? • AAN/AES guidelines
MAJOR CONGENITAL MALFORMATIONS • • • heart malformations, (VSD) orofacial defects, (cleft lip/cleft palate) urologic defects, (hypospadias) skeletal abnormalities, (radial ray defects, phalangeal hypoplasia, ) neural tube defects. (spina bifida) (Meador et al. 2008 a)
Mechanism? • Uncertain folate deficiency, ischemia, neuronal suppression, reactive intermediates (e. g. free radicals or epoxides) AED-induced neuronal apoptosis • T 1 exposure • T 3 exposure- highest risk of anatomical defects highest risk of behavioural
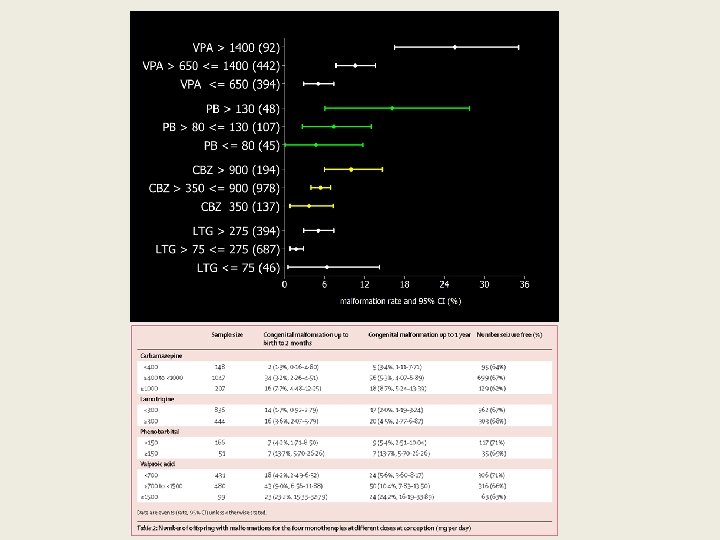
Anatomical terratogenesis • MCMs- 4. 5% as opposed to 2. 1% in controls • Increased risk for MCMs only with VPA(5. 6%, p = 0. 005) AED polytherapy (8. 6%, p = 0. 02) (Meador et al. 2008 a) • VPA as mono or in poly has the highest risk • dose-dependent esp VPA and LTG
Behavioural terratogenesis • WWE on RX neuronal apoptosis in neonatal rat brain -Clon, Diaz, PB, PHT, synergistic effect of two AEDs, given at below threshold dosages AEDs inherently not producing apoptosis in monotherapy, (CBZ, LTG and TPM) can enhance apoptosis induced by another • WWE no RX No difference to normal controls
Exposure to antiepileptic drugs in utero and child development: A prospective population-based study *†Gyri Veiby, ‡§Anne K. Daltveit, ¶Synnve Schjølberg, ‡¶Camilla Stoltenberg, ¶#Anne-Siri Øyen, ‡¶Stein E. Vollset, *†Bernt A. Engelsen, and *†Nils E. Gilhus Doses during pregnancy ? Sz freq in un. Rx WWE?
FOLIC ACID Insufficient data but 2 x class II studies proved benefit Recommend- 0. 4 mg, preceonception (AAN) Vit K Inadequate evidence Practise- If enzyme-inducing AEDs used, routinely receive vitamin K at delivery (AAN)
AEDs and lactation § Safe short t ½ >80% protein bound § Contraindications Long t ½- cumulative effect- sedation with BDZ High milk to plasma ratio- ETX, ZNS § Most 1 st G AEDs can be considered safe VPA, CBZ, PB, PHT, Primidone § 2 nd G AEDs- not much known clinically significant amounts in BM – LEV, LTG, OXC, TPM but therotical infant dose < therapeutic dose for neonates considered moderately safe • ***remember to drop the LTG dose, PP
AED and contraception • COCP, levenogestral implants- avoid with CBZ, PHT, PB, TPM, OXC Start with oestradiol >50 mcg/day • Preferred – intrauterine device/Depo- 10 wkly • COCP can reduce the LTG level – 25 -70%
THANK YOU Australian Pregnancy Registry