Case Presentation PK 19 15 51 Identifying Data



 : 2001년 진단 받고 regular medicaion p")
 : 20년 전 stop, 소주 1병 * # 2")
 p Hypertension (-) p")





 Uvular deviation (-) XI. SCM & Trapezius muscle")
Tone : normal 2) Power 4 4 4 5 5")
 Biceps jerk(+/+) Triceps jerk (++/++) Patella jerk")

 : 손 들라하면 손듬 Expressive dysphasia")








")

")


 Lack of understanding of the rules for")
. Cognitive Brain Research")


- Slides: 37
Case Presentation 신경과 PK 19 조 15, 51번 신상우, 오민주
Identifying Data p p p Name : 장 OO Age : 68 Sex : Male
Chief Complaint Rt. sided weakness and language disturbance for 9 days
Past History p Type 2 DM (+) : 2001년 진단 받고 regular medicaion p HTN p p (+): 2001년 진단 받고 regular medicaion Pul tuberculosis (-) Previous cerebraovascular accident history (+) : 2001년 Rt. side weakness로 경희 의료원 입원 치료후 증상 호전 p previous operation hx p Previous headache history (-)
Personal History p Alcohol (-) : 20년 전 stop, 소주 1병 * # 2 -3 일/ week p Smoking (+) : 40 PY 1갑/일, 40년 p Occupation: 농업 p Education : 초졸 p Rt. Handness p Height: 170 cm Weight: 70 Kg
Family History p Pulmonary tuberculosis p Type 2 DM (-) p Hypertension (-) p (-) Cerebrovascular accident history (+): farther's
Physical Examination p Vital sign : BP 140/80 p G/A p HEENT p p p PR: 72 RR: 20 BT 36. 4 : well developed : Not pale conjuntiva Anicteric sclera Carotid bruit(-/-) Chest : symmetric expansion on respiration Heart : regular heart beat murmur Lung : clear breathing sound Abdomen : soft and flat Extremity : no pitting edema, no cyanosis
Neurologic Examination Mental status 3/22 Consciousness level: looks alert Speech: intact § Speech: : mild dysarthria language § fluency (+) comprehension (+) language : conductive aphasia repetition (+) naming(-) writing (-) reading(+) fluency (+) comprehension (+) repetition (-) naming(-) writing (-) reading(-) § Memory Remote, recent, immediate : unable to check due to poor cooperation § Orientation Time, place, person : unable to check due to poor cooperation §
Neurologic Examination Cranial Nerves I. Olfactory n. – Intact II. Optic N. V/A: Unable to check due to poor cooperation V/F: unable to check due to poor cooperation Fundus: no papilledema & retinal change(-)
Neurologic Examination III. IV. VI. Nerve EOM : intact Pupil : RRERL c 3 mm Nystagmus : no spontaneous or gaze evoked nystagmus V. Facial sensation Pain, temperature, touch, vibration : intact
Neurologic Examination VII. NLFF : unable to check due to poor cooperation Forehead wrinkling (+/+) VIII. Hearing difficulty : intact Weber test : unable to check due to poor cooperation Rinne test : unable to check due to poor cooperation
Neurologic Examination IX. X Gag reflex(+/+) Uvular deviation (-) XI. SCM & Trapezius muscle : intact XII. No tongue deviation on protrusion
Neurologic Examination Motor 3/22 1)Tone : normal 2) Power 4 4 4 5 5 5 5 5 5 3) Muscle bulk : no muscular atrophy Sensory Pain, temperature, Touch, Vibration, position : intact 5 5
Neurologic Examination DTR : Brachioradialis jerk (+/+) Biceps jerk(+/+) Triceps jerk (++/++) Patella jerk (++/++) Ankle jerk (+/+) Babinski's sign (-/-)
Neurologic Examination Cerebellar sign unable to check due to poor cooperation Gait unable to check due to poor cooperation
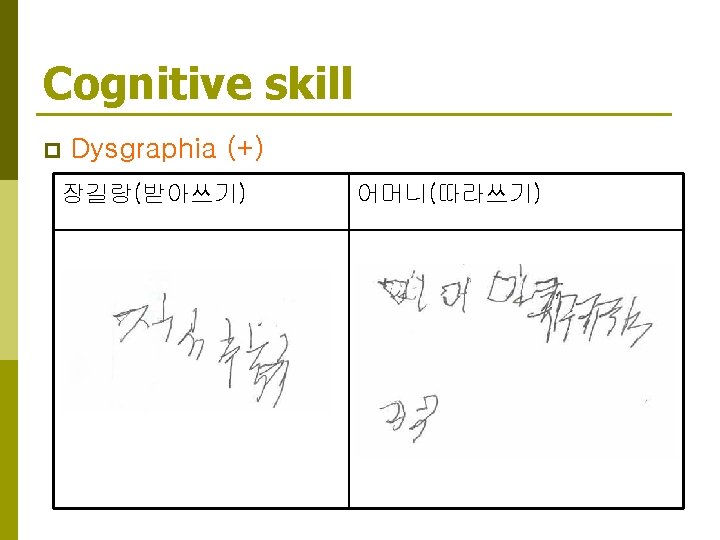
Cognitive skill p p p Receptive dysphasia (-) : 손 들라하면 손듬 Expressive dysphasia (-) : 증상 호소 가능 Dyslexia (-) : 어머니란 단어를 읽을 수 있음 Nominal dysphasia (+) Agnosia finger agnosia : 첫번째 손가락 실인 Dyscalculia : 간단한 계산 (ex. 10 -7=? ) 을 잘 못함
Lab Finding p p p CBC WBC/ RBC/HGB/HCT Electrolyte: Na/K/Cl 6. 61 x 103/u. L /4. 21/12. 20/36. 80 145/3. 6/108 Glucose 141 mg/d. L Hb. A 1 C 8. 6 4. 5 -6. 3 Total cholesterol 107 mg/d. L Lipid Profile(serum) Triglyceride 66. 2 mg/dl HDL-Cholesterol 38. 0 mg/dl LDL-Cholesterol 58. 4 mg/d. L Apolipoprotein A 105. 5 mg/dl Apolipoprotein B 49. 3 m. Eq/L (120~220) 40 -160 >55 <130 여 110 -205 남 110 -180 여 50 -130 남 60 -140
Lab Finding p p p Homocysteine 8. 92 D-DIMER 0. 63 APTT 26. 8 sec PT 0. 91/10. 3(INR/sec) Fibrinogen 435. 6 CRP 0. 9 mg/d (5 -15) 0. 4 20 -38 (1/10~14) 200 -400 L 0 -0. 5
Problem List 1. History DM, HTN , cerebraovascular accident hx, smoking , familial hx 2. Neurologic examination & Cognitive skill Rt. sided weakness Dysarthria Dysgraphia Dyscalculia finger agnosia 3. Lab Finding Glucose 141 mg/d. L Hb. A 1 C 8. 6 4. 5 -6. 3
Formulation 1 Rt. hemiparesis, Dysarthria : Lt. medulla 상방의 corticospinal tract, corticobulbar tract involve 하는 centrum semiovale, corona radiata, int capsule, upper pons lesion 가능 p Conductive aphasia : arcuate fasiculus손상 p Anomic aphasia : any brain area leasion 가능. pons, midbrain, inf. temporal lobule p Dyscalculia : angular gyrus 위 소견을 종합해볼때 corticospinal tract, corticobulbar tract을 포함 하는 Lt. MCA territory의 문제임을 생각해볼 수 있다. p Dysgraphia , dyscalculia , finger agnosia를 볼때 Gerstman syndrome을 의심해 볼수 있으며, dementia 배재할수 없다.
Formulation 2 p History 상 Rt. side weakness and language disturbance for 9 days 를 주소로 내원한 68세 남자 환자로 DM, HTN , CVA hx, smoking , familial hx를 가지고 sudden onset 하는 neurologic deficit 가진 점은 vascular origin 가능성 높다. Trauma history 없으며, headache 없었던 것으로 보아 hamorrhge 보단 occlusion 이나 stenosis 의 가능성이 더 크다. 하지만 gradual 하게 neurologic deficit 심해진 것으로 보아 hamorrhge 배 제할수 없다. sudden onset으로 maximal 한 neurologic deficit 보인 점으로 보 아 emboli에 의한 occlusion 가능성 크다.
Impression p Cerebral infarction - Ischemic, hemorrhagic R/O Occlusion and stenosis of Lt. MCA R/O Gerstman syndrome R/O Dementia p
Diagnostic Plan p Brain CT angiography p Brain MRI- DWI, angiography p SPECT
MRI 3/16 MRA 3/8 안동병원 MRI-DWI 3/16 MRI-DWI
SPECT(03/20)
Diagnosis p Lt. MCA cerebral infarction p R/O Gerstman syndrome R/O Dementia
PTA (MCA stenting procedure, 3/21)
Disease report Gerstmann’s Syndrome
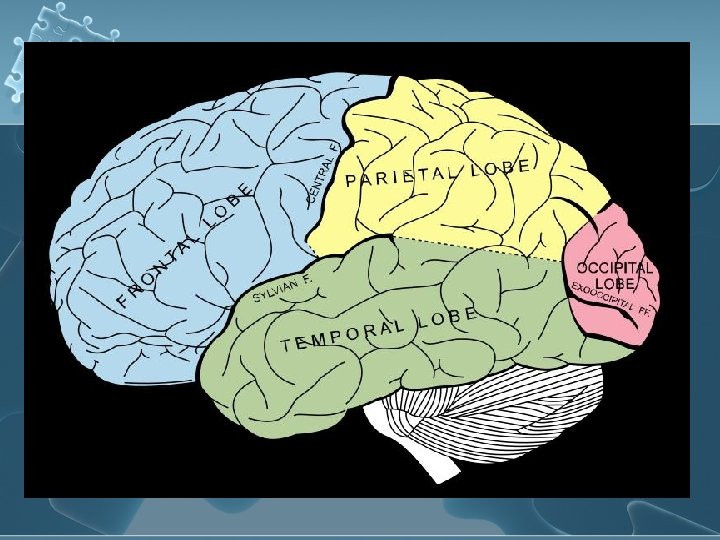
Cause l l l This disorder is often associated with brain lesions in the dominant (usually left) side of the angular and supramarginal gyri near the temporal and parietal lobe junction. 성인에서는 Stroke나 parietal lobe와 연관된 손상이 원인이다. Stroke나 외상시 출혈이 brain의 left parietal lobe(angular gyrus) 침 범. 소수에서는 viral encephalitis, tumor, or toxic exposure 후에도 발생 소아에서는 극소수의 경우만이 있었고, 원인 은 미상이다.
Symptoms l l Writing disability (agraphia, dysgraphia) Lack of understanding of the rules for calculation (acalculia, dyscalculia) Inability to distinguish right from left (Left-right disorientation) Inability to identify fingers (finger agnosia)
우리가 글을 쓸때 l Lt. sup. parietal lobe 가 활성화(P<0. 01). Cognitive Brain Research Volume 12, Issue 2 , October 2001, Pages 337 -340
Treatment There is no cure for Gerstmann's syndrome. l Treatment is symptomatic and supportive. l Occupational and speech therapies may help diminish the dysgraphia and apraxia. In addition, calculators and word processors may help school children cope with the symptoms of the disorder. l
Prognosis In adults, many of the symptoms diminish over time. l In children symptoms may diminish over time, it appears likely that most children probably do not overcome their deficits, but learn to adjust to them. l