Presentation Geriatric Case Conference BowTum 22655 Chief complaint

Presentation… Geriatric Case Conference Bow&Tum 22/6/55


Chief complaint หลงลม 5 ป



Problems list

Differential diagnosis

New Dementia Criteria Loss cognitive or neuropsychiatric symptom O Interfere with work or usual activities O Decline from prior level of ���� ADLs functioning O Not explained by delirium or other psychiatric disorder R/O other cause

Loss cognitive or neuropsychiatric symptom Behavior Languag e Memory Executiv e function Visuospatial Impairment ≥ 2

Physical Examination GA : หญงไทยแตงตวด สะอาด ไมคอยแสดงสหนา BP 120/80 mm. Hg PR 70/min HEENT : not pale, anicteric sclera, normal tooth & gum, no oral lesion LN : no cervical LN enlargement Heart : regular, normal s 1, s 2, no murmur Lung : clear, equal both, no adventitious sound Abd: soft, no mass, not tender , no hepatosplenomegaly

Physicial Examination Ext : No edema, no cogwheel rigidity, no spastic, no resting tremor N/S : pupil 3 mm. RTLBE, full EOM, motor power gr. V all, BBK – plantar flextion both Gait : normal Speech : normal

Test/Date Orientation for time Orientation for place Registration Attention/Calculation Recall Naming Repetition Verbal command Writing command Wristing Visuo-contruction ���� 28/6/54 24/1/55 28/2/55 ���� 1 ���� 2 ���� 3 0 1 0 2 0 3 3 0 0 2 0 1 0 0 0 2 0 1 1 0 0 2 1 0 0 7 8 9

Test/Date CDT Test/Date Cube 28/6/54 ���� 1 24/4/55 ���� 2 2/10 1/10 28/6/54 24/4/55 ���� 1 incorrect ���� 2 Incorrect

Dementia? Severity?



Investigation

Investigation CBC WBC 5200 N 60 L 31 M 6 E 2 Hb 12. 7 Hct 40. 9 MCV 89 MCH 27. 2 RBC morpho normochromia Cr 0. 77 TSH 1. 646 (0. 35 -4. 94) Vitamin B 12 338. 5 (243. 0 -894. 0) VDRL NR B 1

MRI brain O Mild volume loss of hippocampi and parahippocampal gyri with thining of entorhinal cortex, bilaterally which may be represent Alzheimer disease. O The bilateral pars compacta of the substantia nigra of the midbrain are well identified. O The rest of brain parenchyma shows normal signal intensity without space occupying lesion. Brainstem and the cerebellum are unremarkable. The calvarium and the skull base have normal marrow signal intensity. No midline shifting, hydrocephalus or extraaxial collection is detected. Impression O Mild volume loss of hippocampi and parahippocampal gyri with thining of entorhinal cortex, bilaterally which may be represent Alzheimer disease. O Generalized mild cerebral volume loss.

FDG PET O The study reveals severely decreased FDG activity in bilateral parietotemporal cortices which is relative symmetric. There is also mildly to moderately decreased FDG activity in the frontal cortices, right slightly involved more than left. The tracer distribution in the rest of the scanned regions appears within normal limits. Limited low dose, noncontrast CT images show no corresponding abnormality. Impression O Severe hypometabolism of bilateral parietotemporal cortices with less involvement of frontal cortices favor Alzheimer’s disease, less likely Pick’s disease.

Diagnosis

Clinical Features Distinguishing AD and Other Dementias O AD: O Memory, language, visual-spatial disturbances, indifference, delusions, agitation O Frontotemporal dementia: O Relative preservation of memory and visual- spatial, skills, personality change, executive dysfunction, excessive eating and drinking O Lewy body dementia: O visual hallucinations, delusions, extrapyramidal, symptoms, fuctuating mental status, sensitivity to antipsychotic medications O Vascular dementia: O abrupt onset, stepwise deterioration, executive dysfunction, gait changes

Cognitive domain AD DLB bv. FTD Va. D Depression Free recall +++ ++ +/- + + Recognition +++ - - Prompting X √ √ Intrusions +++ +++ + + Semantic memory (naming) ++ + +/- - + + Procedural memory

Cognitive domain AD DLB bv. FTD Va. D Depres sion Working memory ++ +++ ++ +/- Insight +++ + +++ - - Attention ++ +++ Executive functions ++ typical AD +++ frontal variant +++ +++ ++ ++ typical AD +++ PCA +++ - + + Visuospatial skills

Memory impairment in AD

Memory impairment in AD

Memory impairment in AD

Memory impairment in AD

Memory impairment in AD

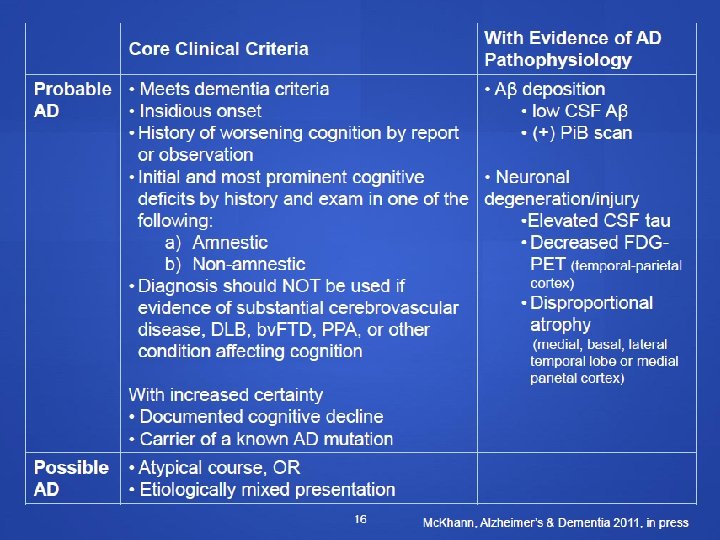
Alzheimer’s dementia criteria O Probable AD O Possible AD O Probable or possible AD with evidence of the AD pathophysiological process O Biomarkers of brain amyloid-beta (Ab) protein deposition O Biomarkers of downstream neuronal degeneration or injury

Atypical AD O Logopenic progressive aphasia O Language O Frontal variant AD O Behavior, Executive O Posterior cortical atrophy O Visuospatial

Frontotemporal dementia FTD

FTD O Dementia in persons younger than 65 years O A neurodegenerative disease of unknown etiology O Behavioral and language O Relatively preserved memory
 usually demonstrates frontotemporal atrophy")
O Neuroimaging (MRI) usually demonstrates frontotemporal atrophy

Types of FTD O Behavioral variant frontotemporal dementia O Semantic dementia O Progressive nonfluent aphasia

Treatment
 1 patch แปะ q 24 hr O Memantine (10) 1")
Medication O Rivastigmine patch(10) 1 patch แปะ q 24 hr O Memantine (10) 1 x 1 oral pc O Sertraline(50) 1 x 1 oral pc O Na valproate chrono(500) 1 x 1 oral pc O Quetiapine (25) 1 x 1 oral hs O Amlodipine (5) 1 x 1 oral pc O Folic (5) 1 x 1 oral pc O Vitamin B 1612 1 x 2 oral pc

Therapeutic strategies O Symptomatic treatment O Disease-modifying therapy O Lifestyle O Diet O Physical Exercise O Mental Exercise

Cholinesterase Inhibitors O Donepezil, Rivastigmine, Galantamine O Mild to moderate dementia O Benefit in severe dementia not as clear

Memantine O Mechanism of action: partial NMDA- receptor antagonist O May block glutamate excitotoxicity O May provide symptomatic benefit via effects on hippocampal neurons O Moderate to severe. Alzheimer’s dementia O Safe in combination with Ch. EI

Pharmacologic Treatment of Agitation Symptoms Medication Agitation in context of nonacute psychosis Olanzapine 2. 5– 10 mg/d Quetiapine 12. 5– 100 mg/d Risperidone 0. 25– 3 mg/d Agitation in context of depression SSRI, eg, citalopram 10– 30 mg/d Anxiety, mild to moderate irritability Trazodone 50– 100 mg/d Agitation or aggression unresponsive to first-line treatment Carbamazepine 300– 600 mg/d Olanzapine (intramuscular) 2. 5– 5 mg IM Sexual aggression, impulse-control symptoms in men Second-generation antipsychotic If no response, conjugated equine estrogens 0. 625– 1. 25 mg/d
 O High in vegetables, legumes, fruits,")
Diet O Mediterranean diet (Scarmeas N. JAMA. 2009) O High in vegetables, legumes, fruits, nuts, cereal, fish, olive oil O Low in saturated fats O Up to 40% reduction in risk for developing dementia

Non pharmacological treatment in dementia O Cognitive focus intervention O Cognitive stimulation O Cognitive training O Cognitive rehabilitation O Other O Music therapy O Aromatherapy O Massage and touch O Exercise Cognitive rehabilitation is an individualised approach where personally Cognitive stimulation is relevant goals are identified engagement in aisrange Cognitive training guided and therapist works with ofthe activities and practice onand a set standard person hisofor her tasks to devise discussions (usually in to family strategies designed to reflectatparticular a address group) aimed cognitive range these. Thefunctions; emphasisa is on general enhancement of difficultyperformance in improving ofeveryday levelsmaylife be available within the standard of taskstests, to cognitive social rather thanand onset cognitive suit building on the person’s functioning. the individual’s level of ability. strengths It may be offered in individual and developing ways of or compensating for group sessions, with pencil impairments and paper or computerised exercises.

Cognitive stimulation

O Control group : usual activity O Doing nothing O Game : bingo, singing, art and crafts

O Intervention : programme O 14 -session programme , twice a week, 45 min per session over 7 weeks O Reality orientation and cognitive stimulation O Topic : using money, word games, the present day and famous faces O Reality orientation board

Cognition



Follow up


O Communication and social interaction • Qo. L • GDS

O ADL, Behavior, caregiver non significant

Cognitive training and cognitive rehabilitation

O Cognitive training : 9 studies O Cognitive rehabilitation : none

Change in MMSE

CHANGE in… O Immediate verbal memory scores O Delayed verbal memory scores Non sign scores O Verbal letter fluency ifican t O Verbal category fluency scores O Executive function scores O Self-report of memory functioning O Participant self-report of mood (depression) O Informant report of participant memory functioning
 O Informant report of participant")
CHANGE in… O Informant report of participant mood (depression) O Informant report of participant functional ability O O O (ADLs) Informant report of informant reaction to participant No memory and behaviour n s problems (Follow up) immediateigverbal nifi memory scores can(sequencing) scores (Follow up) executive function t (Follow up) informant report of participant memory functioning (Follow up) informant report of participant functional ability (activities of daily living)

Music therapy

O Type of music therapy O Receptive music therapy O Active music therapy

Total minute spent not wandering during all sessions of main therapy

Mean change in MMSE

Number of agitated behavior 2 week 4 week

Massage and touch

O The use of hand massage for an immediate and short-term reduction of agitated behaviour O The addition of touch to verbal encouragement to eat for the normalization of nutritional intake

Mean agitate score

Aroma therapy

O Only 2 RCT, other not good study design O Statistical significant in decreased agitated

Evaluation of Response to Any Cognitive Enhancer O Elicit caregiver observations of patient’s cognitive function and behavior (alertness, initiative) and follow functional status (ADLs and instrumental ADLs). O Follow cognitive status (eg, improved or stabilized) by caregiver’s report or serial ratings of cognition (eg, Mini-Cog, MMSE)

Test/Date Orientation for time Orientation for place Registration Attention/Calculation Recall Naming Repetition Verbal command Writing command Wristing Visuo-contruction ���� 28/6/54 24/1/55 28/2/55 ���� 1 ���� 2 ���� 3 0 1 0 2 0 3 3 0 0 2 0 1 0 0 0 2 0 1 1 0 0 2 1 0 0 7 8 9

Test/Date CDT Test/Date Cube 28/6/54 ���� 1 24/4/55 ���� 2 2/10 1/10 28/6/54 24/4/55 ���� 1 incorrect ���� 2 Incorrect

Follow up MMS E ADLs / i. ADL s Functio n Caregiv er Cogniti on Sleep Safety O • Hallu/Delu • Apathy • Depression • Agitation • Manic. Typical AD MMSE like/attention drop ≥ 3/yr GI, drop GU, ≤ 2/yr • REM O MMSE cardio, temp, BPSD • Insomnia work dysphagia O Advance directive !!! • Increase ANS sleep day Driving, falling, Neuro financial

THANK YOU
- Slides: 80





































 is to")




























































