Points of Geriatric Psychiatry o Epidemiology n n






 facilitieso 4. 13% elders in LTC facilities in 1995 o 8%")




")












- Slides: 64
Points of Geriatric Psychiatry o Epidemiology n n o o Normal aging Psychiatry disorders or problems commonly seen n o Prevalence of mental disorder Barriers to mental health service utilization Dementia, depression, delirium, sleep problems, anxiety, suicide Treatment n n Pharmacotherapy, Psychotherapy Treatment models
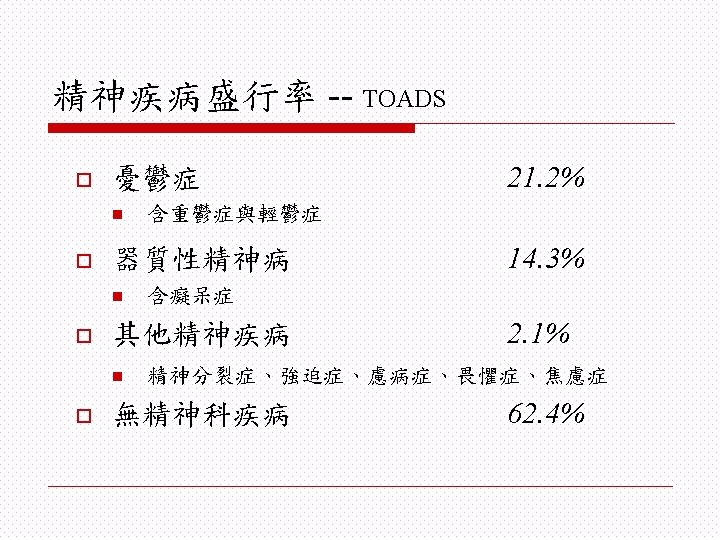
Mental disorders among older adults--ECA community inpatients Cognitive impairment 4. 9 30. 2 Affective disorders 2. 5 18. 5 Anxiety disorders 5. 5 5. 2 Alcoholism 0. 9 2. 6 Schizophrenia 0. 1 0 Somatization 0. 1 0 Personality disorders 0 8. 3 Others 0 7. 9
Normal aging -- neuropsychiatry o Brain structure n Decrease in gross brain weight n Widened sulci, gyral atrophy, Ventricles enlarge n Increased transport across BBB n Prefrontal lobes are disproportionately affected by aging changes n Subcortical monoaminergic cell populations are subject to prominent decline in aging
Normal aging -- neuropsychiatry o Cognition n Takes longer to learn new materials n IQ remains stable until age 80 n Verbal ability maintained with age n Psychomotor speed declines n Encoding ability diminishes n Simple recall declines
Normal aging -- Sleep o Latency to sleep onset o Frequency of awakening o Total stage-3, & -4 sleep o Total stage-1, & -2 sleep o Redistribution of REM sleep
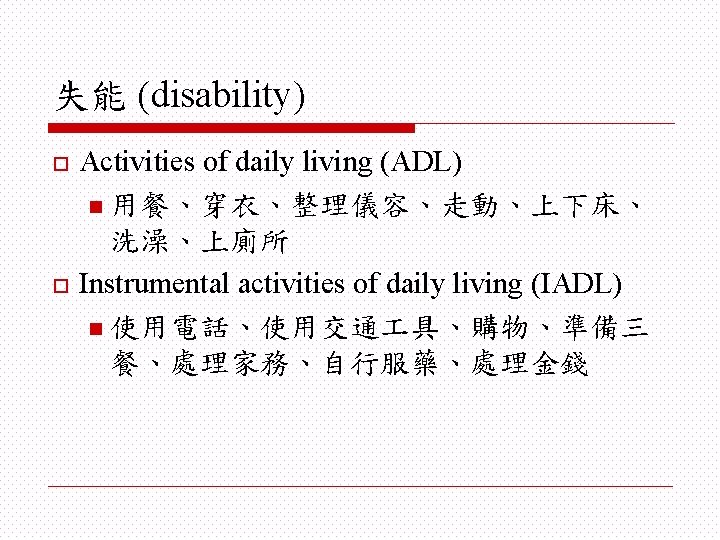
Features of Mental Problems among the elderly o Highly comorbid with n n o Complication of psychopathology n n o Medical illness Disabilities Cognitive dysfunction Distinct clinical courses Barrier to assess mental health resources
Long-term care (LTC) facilitieso 4. 13% elders in LTC facilities in 1995 o 8% of nation’s total health care costs o Mean age increased in LTC facilities o Very disabled o Options and setting becoming diverse Jones A: Vital Health Stat 13 2002: 1 -116 Gabrel C and Jones A: Vital Health Stat 13 2000: 1 -83 USA data
Barriers to geriatric mental health care o Poorly served by the mental health system n n n o Fewer visits for mental health care Rely more heavily on primary care physicians Low rate of depressive elders taking antidepressant Possible reasons n n n Stigma Low rate of case identification by primary physicians o Multiple medical illnesses divert physicians’ attention o Depression and anxiety may be viewed as normal Neglect by family
Life events o o o Death of significant others Medical ill of oneself or partner Disability Financial issues Relationship with family Retirement
Somatic Symptoms Physical Illness Depressive Disorder
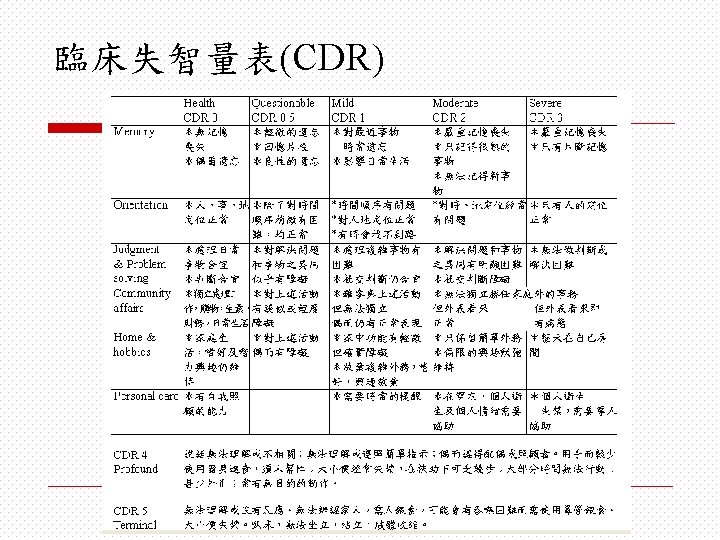
Cognitive deterioration Dementia Depression (pseudodementia)
Delirium譫妄
Causes of delirium o o o Drugs and alcohol Intracranial causes Metabolic and endocrine disorders Systemic infections Postoperative states
Late life depression o o Late-onset vs. early onset Vascular depression Subsyndromal depression Depression-executive dysfunction syndrome
Suicide Increases with: age bereavement isolation deteriorating health pain Actual & attempted are closely linked
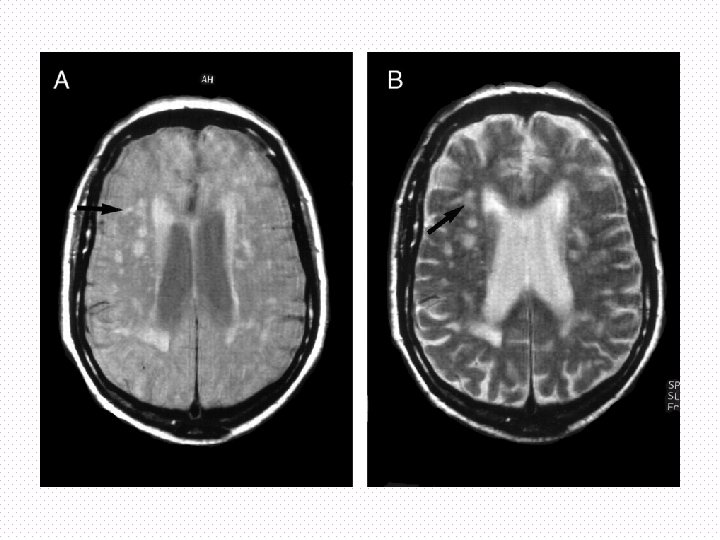
Vascular depression hypotheiss o o Subtype Vascular risk factors, neuroimaging findings More cognitively impaired, more disabled, more psychomotor retardation, less insight Disruption by vascular lesions of striato-pallodo -thalamo-cortical pathways
Medications associated with depression o Antihypertensions n n n o o Reserpine Methyldopa βblockers Oral contraceptives Steroids BZD H 2 antagonists n n Cimetidine Ranitidine o Chemotherapy n n o …. . Interferon Psychoactive substances n n n Alcohol Opiates Amphetamine withdrawal
Treatment o o Treating underlying medical conditions & reducing disability Psychopharmacology: selection depends on n n o o Side effect profiles Concurrent conditions and medications Target symptoms Previous treatment responses ECT Psychotherapy
Sleep disorders o o Lack of social or vocational activity Disturbed circadian rhythm n n o o o living in nursing home, without daily routines degenerative brain Breath related sleep disorders Alcohol or drugs induced sleep disorders Sleep related accidents
Neuropsychiatric syndrome o Post Stroke syndrome n o Depression, anxiety, apathy, psychosis, mania, emotional lability Parkinson’s disease and Parkinsonism n Depression, anxiety, mania, psychosis, drug induced psychosis
Principles of pharmacological treatment o o o Pretreatment medical evaluation Given in equally divided dose Reduced dose to 1/4~1/2 as the young need Simplified medicine Slow titration from low dose Know the interaction between medicine
謝謝收看 敬請指教 Email: sheng@kmu. edu. tw