GERIATRY AND GERONTOLOGY DR IOANA ALEXA THE MAJORITY














: old age is the highlight")



 U. S. Bureau of Census")
")






























 They let an individual live independently in a")

 and")












 Normal Mild cognitive impairment) Cognitive function Mild Dementia uşoară")








, Isabell Arnet, Philipp Walter and Kurt Hersberger, Pharmaceutical")









 1999 - 2006 n It has a 1000 words")




- Slides: 92
GERIATRY AND GERONTOLOGY DR. IOANA ALEXA
THE MAJORITY OF ELDERLY PATIENTS WOULD HAVE MULTIPLE HEALTH PROBLEMS n n n n n heart insuficiency class II NYHA paroxystic AF chronic myocardial ischemia atherosclerotic hypertension hypercholesterolemia diabetes mellitus chronic kidney disease, possibly secondary to ischemic nephropathy urinary infection prostate adenoma n n n n varicosis cerebral circulatory insuficiency chronic degenerative rheumatism systemic osteoporosis gallbladder stones early stage cataract both eyes minor cognitive impairment anxiety
THE FINAL PRESCRIPTION WOULD LOOK LIKE THAT: n n n n Amiodarone, od Acenocumarole, od indapamide, od nitrate, twice a day Ca channel blocker, od ACE inhibitor, od statine, od fibrate, od dyosminum twice a day Hepatrombine, ointment, twice a day Metformine, 2 -3 times a day Hypoglicemic sulfonamide, od Antibiotic, twice a day ± urinary antiseptic pills, 2 -3 times a day alpha adrenergic blocker, od n n n n Pentoxifilin, 400 mg x 3/zi Derivaţi de gingko biloba, 1 tb x 3/zi Stugeron, în 2 -3 prize/zi Milgama (dată fiind şi prezenţa diabetului), în 2 prize/zi Inhibitor de COX-2 (Arcoxia, 60 mg/zi) Diclofenac 5%, ung local x 3/zi Mydocalm, 150 mg x 3/zi, 10 zile Tramadol/Zaldiar, 50 mg x 3/zi Myacalcic (Calcitonină) spray, 1 puff x 3/zi Cal. Devit, 1 tb x 2/zi Rubjovit, sol. oftalmică, 1 -2 pic instilaţii oculare Lorazepam, 0. 5 mg/zi Buspironă, 5 mg x 3/zi Piracetam, 1 tb x 2/zi Pronoran, 1 tb x 2/zi
This will sum up to: n an impressive diet, as our patient should have restriction on glucose, lipids, proteins, salt, smoking, drinking, too much exercise, too little exercise. . 29 drugs 48 administrations as: n n tablets n ointment n spray ophthalmic drops n n
Our goal: the right medication, the right dose, the right time
n POLIMEDICINE POLIPHARMACY IATROGENY n WHO TAKES CARE OF SUCH PATIENTS? n n
GERIATRICS AND GERONTOLOGY n n The branch of medicine that focuses on health care of the elderly It aims to promote health and to prevent and treat diseases and disabilities in elderly patients
n Geriatrics differs from adult medicine in many respects. The body of an elderly person is substantially different physiologically from that of an adult. Old age is the period of manifestation of decline of the various organ systems in the body. This varies according to various reserves in the organs, as smokers, for example, consume their respiratory system reserve early and rapidly.
n n Geriatricians aim to treat the disease and to decrease the effects of aging on the body Years of training and experience, above and beyond basic medical training, go into recognizing the difference between what is normal aging and what is in fact pathological.
n n n The decline in physiological reserve in organs makes the elderly develop diseases (such as dehydration from a mild gastroenteritis) and be liable to complications from mild problems Fever in elderly persons may cause confusion leading to a fall and to a fracture of the neck of the femur ("breaking her/his hip"). Functional ability, independence and quality of life issues are of greater concern to geriatricians, perhaps, than to adult physicians.
n n n Treating an elderly person is not like treating an adult. A major difference between geriatrics and adult medicine is that elderly persons sometimes cannot make decisions for themselves. The issues of power of attorney, privacy, legal responsibility, advance directives and informed consent must always be considered in geriatric procedure. Elder abuse is also a major concern in this age group. In a sense, geriatricians often have to "treat" the caregivers and sometimes, the family, rather than just the elder.
n The so-called 'Geriatric giants' are: n n n Immobility Instability Incontinence Impaired intellect/memory Health issues in older adults may also include elderly care, delirium, use of multiple medications, impaired vision and hearing.
n n n In the United States, geriatricians are primary care physicians who are board-certified in either family medicine or internal medicine and who have also acquired the additional training necessary to obtain the Certificate of Added Qualifications (CAQ) in geriatric medicine. In the United Kingdom, most geriatricians are hospital physicians, while some focus on community geriatrics. In contrast to the United States, geriatric medicine is a major specialty in the United Kingdom; geriatricians are the single most numerous internal medicine specialists.
HISTORY n n n Bible: Matusalem = 969 years old, Moses = 120 years old Ancient Egypt: Ebers papyrus (1550 b. c. ): “The weakness of the old ones is due to dilatation of the heart” India: “life can be prolonged by a healthy way of living”
n n n China (sec VI b. c. ): old age is the highlight of life as we gain wisdom and knowledge Confucius: elderly deserve the higher respect Grece: Sophocles = 91 years old, Socrates = 98 years old n Aristote: the first Textbook of Geriatry (7 pages)
WORLD POPULATION
LIFE EXPECTANCY
Source: United Nations Department of Economic and Social Affairs, Population Division. World Population Prospects. The 2004 Revision. New York : United Nations, 2005.
Number of Americans >65 (Millions) U. S. Bureau of Census
Total U. S. Market for Elderly Drugs ($ Billion)
EVALUATION OF AN ELDERLY PERSON
HISTORY n Physicians often need to spend more time interviewing and evaluating elderly: n n n Many non-specific symptoms, making difficult to focus Sensory deficits (hearing or vision impairment) Underreport symptoms which they consider part of normal aging NO SYMPTOMS SHOULD BE ATTRIBUTED TO NORMAL AGEING!
HISTORY n n n Clinical features of diseases may differ from those in younger patients: dyspnea may be absent in a patient with HF and arthritis Because of cognitive dysfunction they may have difficulties recalling all past illnesses and drugs Patient’s chief complaint may differ from what the family considers the main problem
APPROACH TO THE INTERVIEW n n n Ask the patient about everyday concerns, social circumstances and find out information about one’s psychology; it will help orient and guide the interview Ask him to describe a typical day: it may reveal more than focusing only on the main complaint and it will give information about quality of life, liveliness of thought, and physical independence This approach is very important especially during the first meeting!
n It is important to establish a good relationship with the patient: it will help you to communicate with him and the family members and to obtain adherence with treatment
n n Patient should be fully clothed during the interview and should wear dentures, eyeglasses or hearing aid if necessary so communication can be facilitated The interviewer should stay close to the patient, facing him directly, speaking clearly and slowly (to allow lip-reading) and looking directly in his eyes
n Some patients prefer to have a relative present but, unless mental status is impaired, the patient should be interviewed alone to encourage the discussion of personal matters
PAST MEDICAL HISTORY n n n The physician should record the drug history, topical drugs must be included It could be better if the patient could bring all the pills, ointments or liquids the patient uses The patient should be tested if capable to take the medication recommended (recognize drugs, read labels, open vials)
n n The physician should know nutritional habits, alcohol intake, dietary fiber, and the amount of money the patient can spent on food and if he has suitable kitchen facilities We should assess the patient’s ability to eat: decreased vision, arthritis, immobility, tremors, urinary incontinence
FAMILY AND SOCIAL HISTORY n Family history should focus on: n n Alzheimer’s disease Diabetes cancer Social history includes assessment of patient’s living arrangements, best achieved by a home visit (home features that can lead to fall should be identified and solved) n n Let the patient describe a typical day Marital status, economic difficulties, tobacco and alcohol use
n Don’t forget to ask: n n What are your wishes regarding measures for prolonging life Who is taking surrogate decisions in case of incapacity
PHYSICAL EXAMINATION n n May require additional time to undress and transfer to the examining table: they should not be rushed! Preliminary assessment: observe personal hygiene
VITAL SIGNS n n During measurement of height and weight: patients with balance problems should be helped Temperature recording (the absence of fever does not exclude infection) Pulse (taken for more than 30 sec) and blood pressure Respiratory rate
BLOOD PRESSURE n n BP might be overestimated because of arterial stiffness: there should be several measurements under resting conditions Orthostatic hypotension is quite common: all patients should be checked for it (BP in supine position, than observed more than 3 min in standing position)
SKIN n n n Search for pre-malignant and malignant lesions and tissue ischemia ! Pressure sores: the ulceration of the skin surface is smaller than the underlying soft tissue lesion Unexplained bruises may indicate abuse
EYES n n n Loss of orbital fat enophthalmos (not necessarily a sign of dehydration) Test visual acuity Screen for glaucoma and cataract
CARDIOVASCULAR SYSTEM n n n The size of the heart: one can find displacements of the apex due to kyphoscoliosis, not to HF Systolic murmur: aortic valve sclerosis (it may not be hemodynamically significant) Bradycardia may be normal but should be investigated anyway
GASTROINTESTINAL AND GENITO-URINARY SYSTEMS n n Weak abdominal muscles: it may result hernias Look for abdominal aortic aneurysm Examine ano-rectal area + perform a digital examination (examine the prostate as well) Regular pelvic examination
MUSCULOSKELETAL SYSTEM n n n Examine carefully joints: tenderness, swelling, subluxation, crepitus, redness, etc Determine active and passive range of motion Identify and treat any foot problems: it will maintain elderly’s independence
n SARCOPENIA is the degenerative loss of skeletal muscle mass and strength associated with aging.
NEUROLOGIC STATUS n n The neurologic examination is similar to that for any adult = assess cranial nerves, motor function, sensory function and mental status Non-neurologi disorders common in elderly may complicate the examination: n Diminished sight and hearing may impair cranial examination
n Homeostenosis = the characteristic, progressive constriction of homeostatic reserve that occurs with aging in every organ system.
n Parameters that don’t change with aging: n n n RBC, WBC, PLT Electrolytes Ureea Liver tests Thyroid tests
n Parameters that change with aging: n n n n Blood glucose ESR Creatinine Serum albumine asymptomatic bacteriuria X-ray ECG
COMPREHENSIVE GERIATRIC ASSESSMENT
COMPREHENSIVE GERIATRIC ASSESSMENT n n The cornerstone of the practice of geriatric medicine is the multidimensional assessment of the elderly The term comprehensive geriatric assessment (CGA) refers to this process of evaluation and management of older patients The 1987 National Institutes of Health (NIH) consensus conference defined CGA as “a multidisciplinary evaluation in which the multiple problems of older patients are uncovered, described, and explained, if possible, and in which the resources and strengths of the person are catalogued, need for services assessed, and a coordinated care plan developed to focus interventions on the person's problems” This approach is useful in all settings in which we encounter older patients, whether in the home, office, hospital, day facility, or institutional setting.
DIFFERENTIATE
COMPREHENSIVE GERIATRIC ASSESSMENT n Evaluation of functional status includes information on the patient's ability to perform basic and complex activities of daily living. Gait, balance, and risk of falls should also be assessed. The findings on functional assessment are often linked to the basic physical health assessment.
BASIC ADL Consist of self-care tasks, including: n Personal hygiene and grooming n Dressing and undressing n Self feeding n Functional transfers (getting into and out of bed or wheelchair, getting onto or off toilet, etc. ) n Bowel and bladder management n Ambulation (walking with or without use of an assistive device (walker, cane, or crutches) or using a wheelchair) A useful mnemonic is DEATH: dressing, eating, ambulating, toileting, hygiene.
FUNCTIONAL ASSESSMENT n n Typically ADL performance is lost in a predictable sequence. Skills for bathing and dressing are diminished before transferring, toileting, grooming, and eating. An atypical pattern of loss may have diagnostic significance. For example, early loss of continence may reflect a more localized problem with the genitourinary system. ADL deficits often indicate a need for in-home assistance in the community setting. The number and type of deficits suggest the amount of assistance needed. Problems with bathing alone may indicate a need for a home health aide 2 to 3 times per week, whereas dependence in more areas may require daily or 24 -hour care.
INSTRUMENTAL ACTIVITIES OF DAILY LIVING (IADLs) They let an individual live independently in a community: n Housework n Taking medications as prescribed n Managing money n Shopping for groceries or clothing n Use of telephone or other form of communication n Using technology (as applicable) n Transportation within the community A useful mnemonic is SHAFT: shopping, housekeeping, accounting, food preparation/meds, telephone/transportation.
Occupational therapists often evaluate IADLs when completing patient assessments. Assessments may include 9 types of IADLs that are generally optional in nature and can be delegated to others: n Care of others (including selecting and supervising caregivers) n Care of pets n Child rearing n Use of communication devices n Community mobility n Financial management n Health management and maintenance n Meal preparation and cleanup n Safety procedures and emergency responses
n Mental health evaluation should include the use of standardized cognitive screens (MMSE) and more thorough testing when indicated. Because of the atypical presentation of depression in this age group, screening for depression should also be included.
COMPREHENSIVE GERIATRIC ASSESSMENT n n The social assessment should identify support network strengths and weaknesses. Some determination of the patient's values and the presence or absence of formal advance directives should be determined. Caregiver burden should be evaluated. Financial resources to meet current and future needs should also be assessed. Environmental issues should be evaluated through patient and/or family reports or direct observation of the living situation. Accurate information allows for recommendations that may maximize functional independence in the individual's environment and address basic safety issues.
IATROGENY AND THE ELDERLY
INTRODUCTION n n The etymology of iatrogeny is from Greek: iatros = physician; gennon = induce Iatrogeny refers to any unwanted event induced by an intervention belonging to health system either ambulatory or during hospitalization … by any person involved in medical gestures: doctors, nurses, persons performing kinesitherapy or physiotherapy, psychotherapists and the patient himself (lack of proper surveillance) Soubrié et Lebrun-Vigne
DEFINITION n Iatrogeny should include any unwanted effect induced by any diagnostic, therapeutic or prophylactic gesture performed in the health system.
CAUSES OF INCREASED VULNERABILITY OF ELDERLY
DECREASE OF FUNCTIONAL RESERVOIR OF ORGANS AND SYSTEMS n n Aging is always associated with a progressive decline in all functions which favors drugs’ side effects and iatrogenic complications of interventional medicine Multiple hospitalization favor nosocomial infections with multiple resistant germs
ALTERATIONS OF MUSCLES, JOINTS AND BONES n n Parkinson Rheumathoid arthritis Arthrosis Stroke
n FDA Warning July 2009: Tablet splitting: a risky practice n n n 24. 1 % of recommended tablets are capable of splitting 8. 7 % are not made for splitting 3. 8 % should not be splitted
VISUAL ALTERATIONS n n n Catharact/glaucoma Do not identify tablets by their color! Be able to identify the tubes with adequate tablets!
PHYSIOLOGICAL CHANGES THAT INFLUENCE PHARMACOKINETICS AND PHARMACODYNAMICS IN ELDERLY n n n decrease of absorption decrement of hepatic functions will induce decrease of liver’ capacities of metabolizing drugs decrease of renal function
SLEEP DISTURBANCES INSOMNIA
DEPRESSION
DEMENTIA MCI (Mild Cognitive Impairment) Normal Mild cognitive impairment) Cognitive function Mild Dementia uşoară Severe Dementia Age
ELDERLY AND VULNERABILITY n n n Numerous comorbidities need numerous medical services, which expose elderly people to the risk of aggressive investigations (contrast investigations, endoscopy, catheterism) and to polimedication, usually prescribed by different specialists Medical non-compliance is much more severe in elderly usually due to polimedication associated with difficult medical schemes recommended in patients with cognitive disorders, sensory and motor deficiencies and lack of a familial or social support for the possible handicap Drug posology is usually inappropriate
CONCLUSION n n Elderly patients need a careful monitorization and a refined therapeutical individualization because they are difficult to include in the standardized medical procedures due to comorbidities with functional deficits, which may need polipharmaceutical approach with possible medical interferences Therapeutical individualization must take care of the patient’s and his family’s needs, respecting the rules of informed consent; these patients should have a multidisciplinary approach without excessive hospitalization
CONCLUSION n n The demographic trend of the aging of population with an increment of the old and very old persons suggest the imperious need of a geriatric education for all doctors, no matter the specialty, which should be acquired during studenthood and afterwards Geriatry, until recently still in the process of defining itself, begins to surface in the first line of medical assistance (in hospitals and out-patient system) as every specialist would have to treat elderly persons
CONCLUSION n Iatrogenic pathology, extremely frequent in elderly, should be introduced in every specialty’s curricula because avoiding drugs’ side effects is as important as insuring therapeutical efficacy; iatrogeny can spoil the results of any good treatment and can increase greatly patients’ suffering and medical costs.
GUIDELINES FOR EFFECTIVE PRESCRIBING n n Obtain a complete drug history. Have patients bring all drugs to the office visit for review. Ask about allergies, adverse reactions, use of tobacco, alcohol, caffeine, and recreational drugs and any other health care providers. Use no drugs before its time. Avoid prescribing when no diagnosis has been established, when symptoms are minor or nonspecific, or when the benefit of drugs is questionable
GUIDELINES FOR EFFECTIVE PRESCRIBING n n Use no drug beyond its time. Review drug lists at each visit and update them. Discontinue any drugs that are no longer indicated. Monitor the use of as-needed and over-the-counter drugs. Know the drugs you use. Know the pharmacologic profile of the drugs you prescribe and the potential adverse effects and toxicities. Monitor patients closely for deterioration in functional parameters that could be drug related
GUIDELINES FOR EFFECTIVE PRESCRIBING n n Start low, go slow. Always use the minimum dose necessary for efficacy. Use drug levels when available and appropriate. Treat adequately. Use dosages sufficient to achieve therapeutic goals, as tolerated. Do not withhold therapy for treatable diseases.
GUIDELINES FOR EFFECTIVE PRESCRIBING n n Encourage treatment adherence. Clearly communicate with patients about therapeutic goals and methods to achieve them. Give legible written instructions. Consider complexity of dosing schedules, expense, and potential adverse effects when choosing a drug. Use new drugs with particular caution. Most new compounds have not been thoroughly evaluated in the elderly, and the risk/benefit ratio is often unknown. The Merk Manual of Geriatrics
n Polymedication Electronic Monitoring System (POEMS), Isabell Arnet, Philipp Walter and Kurt Hersberger, Pharmaceutical Care Research Group, Department of Pharmaceutical Sciences, University of Basel, Switzerland, 2013
GERONTECHNOLOGY AND THE QUALITY OF LIFE
m a i n t a i n g a n d c o n t i n u a l l y i m p r Role of technology as a means of maintaining and continually improving the functional independence and quality of life in aging individuals through gerontechnological solutions in the home, community, and institutional environments of elderly
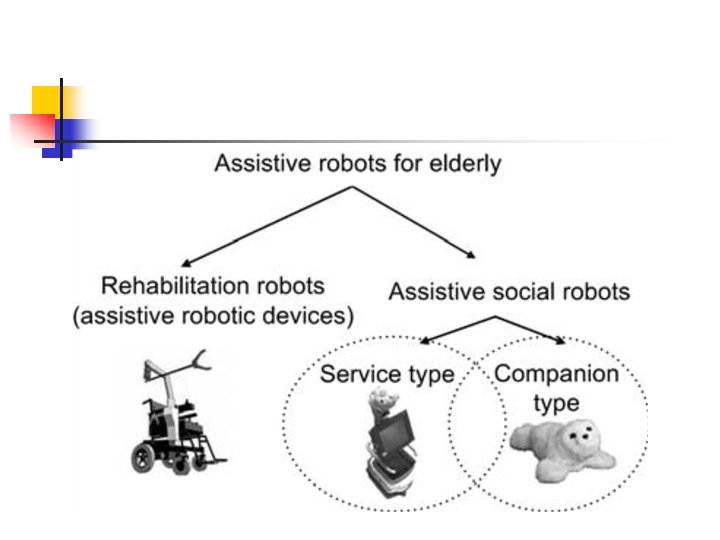
IF AGING ISN'T YOUR CONCERN NOW, WAIT AWHILE, IT WILL BE! n ROBOTS
ASSISTIVE ROBOTIC WALKER
THE FITNESS INSTRUCTOR n n Taizo is aprox. 70 cm high, weights aprox. 7 kg and has 20 functional “joints” He can do 30 types of physical exercises implemented by a fitness expert and he can say “Hello” and “Let’s do another exercise. ”
ASSITIVE ROBOTIC DEVICES DOMO – the housekeeper robot It helps the elderly in daily elementary activities: preparing the meals, bathing, dressing It provides several domestic tasks: cleaning, monitoring health parameters, security
WAKAMARU – LIVES WITH PEOPLE It is 1 m high and has a nice, human-like expression It offers company (it is connected to Internet and has an extended vocabulary)
ASSISTIVE SOCIAL ROBOTS Increase the quality of life by escaping loneliness
AIBO (Artificial Inteligence ro. BOt) 1999 - 2006 n It has a 1000 words vocabulary, so he can ask his master about simple things
THE EMOTIONAL ROBOT CAT i. Cat has 13 servers that control different parts of the face so it can express joy, surprise, sadness Hasbro White Cat – music loving cat n
THE HUGGABLE n n n Pets diminish stress, decrease hearts rate and increase optimism Pet therapy is often used for children/elderly hospitalized patients with depression/dementia If the patient is not capable to take care of a real pet, we can turn to the robots
PARO – THE CUDDLY ROBOT