COMMON SURGICAL DISEASES OF THE STOMACH AND DUODENUM



 • Periodicity • Problems( Complications) – Bleeding – Perforation –")











 – Vagotomy • Truncal Vagotomy")






















")










 • Deep penetrated")
 • Confinement to mucosa and")
 • Varity of")














 – Simple")



- Slides: 71
COMMON SURGICAL DISEASES OF THE STOMACH AND DUODENUM • Dr. Babiker Ali Babiker Mohammed • MBBS, FRCSEd, Diploma in Laparoscopy • Consultant General & GI Surgeon • Prince Mohammed bin Abdulaziz Hospital
COMPONENTS • PEPTIC ULCER • GASTRIC TUMOURS • DUODENAL TUMOURS
Peptic ulcers
APD • Pain (dyspepsia) • Periodicity • Problems( Complications) – Bleeding – Perforation – Gastric Outlet obstruction
APD Pathology Duodenal Ulcer: • Ist part of duodenum • Anterior ulcer perforates • Posterior ulcer bleeds • Kissing ulcer • Always benign Gastric Ulcer: • Along the lesser curve at Incisura • Larger • Benign or Malignant – Ulcerated ca – Ulcer---- Ca • Size/Site/Margin • Multiple biopsy
Peptic ulcer – cause……………. .
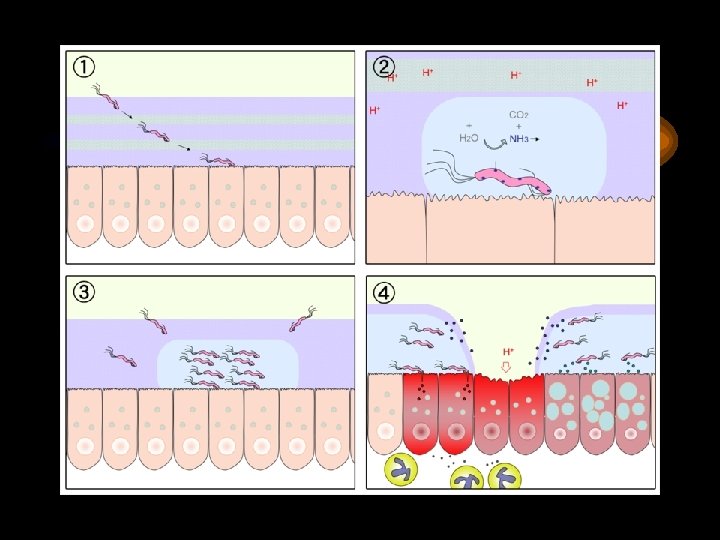
H pylori • • Gram negative flagellate bacillus Urease producing Penetrates mucosa Responsible for DU: 80% GU: 66% Barry Marchal
H pylori
Proposed natural history of H pylori infection Environmental factors Gastric Ca GU Lymphoma Chronic Active Gastritis Multifocal atrophic gastritis H pylori Acute gastritis Antral predominant gastritis DU Lymphoma
• Haemotology • Biochemistry – Serology for H pylori/Urea Breath test • Radiology – Barium meal • Special – Endoscopy and biopsy – CLO test Investigations
Points for Practice H Pylori Infection: Endoscopic Diagnosis Rapid Urease test H Pylori Histology
Non Endoscopic Diagnosis Urea Breath Test Heliprobe
Uncomplicated Duodenal ulcer Needs only Medical Managemen
H Pylori Infection Treatment • Triple Therapy – Drugs ( PPI with 2 of the 3 drugs as given below) • Amoxicillin, : 1 gm BID • Clarithromycin : 500 mgm BID • Metronidazole : 500 mgm BID ( or tinidazole) – Duration: 10 -14 day – Practical points: • Beware of resistance of metronidazole • Tetracycline, Bismuth are other drugs( Quadruple therapy) • Rabeprazole regime: for 1 week Chiba N, et al Meta-analysis of the efficacy of antibiotic therapy in eradicating Helicobacter pylori. Am J Gastroenterol 1992; 87: 1716 -27.
APD Treatment • Diet • Drugs – H 2 blockers/PPI/ – Eradication therapy: ‘Triple therapy’ for One Week • Amoxycillin+Metronidazole+Omeprazole • Clarithromycin+Metronidazole+Omeprazole
Uncomplicated APD Treatment 2 • Surgery: Rarely done (historical) – Vagotomy • Truncal Vagotomy with Drainage – GJ/Pyloroplasty • Selective Vagotomy with Drainage – GJ/Pyloroplasty • Highly selective Vagotomy – Preserve Latarjat nerve – Gastrectomy • Billroth I and II
Billrith I and II Gastro duodenal continuity GJ and Duodenal stump
APD Complications • Bleeding • Perforation • Gastric Outlet obstruction
Minimally Invasive Surgery
Complicated Duodenal Ulcer Needs Minimal access/Surgical management -Bleeding DU -Stricture -Perforation
Perforated DU/GU • Etiology – refer • Pathology – refer • • Clinical Presentation Investigation DD Treatment
Perforated Ulcer • As ‘Acute Abdomen’ • Hypovolumic shock/ Board like abdomen • DD – Pancreatitis – Cholecystitis – AAA – Medical cause • MI/Pleurisy/Pulmonary embolism etc
Perforated ulcer Investigation • Haemotology – FBC • Biochemistry – Urea and electrolytes – Amylase • Radiology – X ray chest and abdomen – US/CT • ECG
Perforated Ulcer Treatment • Resuscitation • Analgesia/Aspiration/Anti biotics/Acid suppression • Surgery – Peritoneal lavage and Omental patch – Definitive ulcer surgery(refer)
Perforation of DU
Bleeding Ulcer
Endoscopic Haemostasis Options: n. Injection Dilute Adrenaline u n. Heat Probe n. Diathermy n. Laser
Endoscopic Haemostasis of Bleeding ulcer: Injection therapy When to consider • Forrest 1 A, 1 B /2 A What to administer • 1/10, 000 adrenaline in saline • 23 G sclerotherapy needle How to give 1 -2 cc aliquot upto 20 ml Can be combined with thermal methods
Modes of Endoscopic Haemostasis Injection Bicap proble Laser Heater probe
Role of Surgery in Bleeding DU Indication: • Failure of conservative management or endoscopic haemostasis Eg: Large posterior DU in an unstable pt Laparotomy/ • Gastroduodenotomy/underrun bleeding ulcer with figure of 8 suture/ pyloroplasty /vagotomy
Gastric Outlet Obstruction Etiology • Congenital • Inflammatory: Chronic DU • Neoplastic – Ca distal stomach – Ca head of pancreas
GOO Pathology • Obstructing lesion – Benign/malignant • Dilated atonic stomach with undigested food
GOO Clinical Features Symptoms: • Projectile vomiting – Yesterdays food! • Wt loss Signs: • Dehyrated patient – Dry tongue – Sunken eyes – Skin ridge • Distended stomach – VGP – Succussion Splash
GOO Investigation • Haemotology – Hb/PCV • Biochemistry – Urea – Na, K low – Hypochloraemic alkalosis • Radiology – Ba me/US/CT • Special – Endoscopy
GOO Treatment • Rehydrate the dehydrated patient – Saline • Empty the distended stomach – Wide bore Ryle’s tube • Drain the obstructed stomach – Gastrojejunostomy
Pyloric Stenosis: Balloon Dilatation/GJ Management: 1. Endoscopic balloon dilatation 2. Gastrojejunostomy • Open • Lap
Tumors of the stomach and duodenum These are : Polyps Tumours : benign malignant
INTRODUCTION - STOMACH Benign • Polyps – Hyperplastic – Fundic gland – Neoplastic – Multiple • Tumors – Leiomyomas – Lipomas Malignant • Tumors – Carcinoma – Lymphoma – Sarcoma – Carcinoid
GASTRIC POLYPS • Hyperplastic polyps – Most common type of polyp (65 – 90%) – Inflammatory or regenerative polyps • In reaction to chronic inflammation or regenerative hyperplasia • Often found in HP infections
GASTRIC POLYPS – Sessile and seldom pedunculated • Mostly in the antrum • Multiple in 50% of cases • Varying in size but seldom < 2 cm – Rate of malignant transformation 1 – 3% • Usually larger than 2 cm
GASTRIC POLYPS • Fundic Gland – Small elisions in the fundus • Hyperplasia of the normal fundic glands – Often associated with FAP • Therefore important as a marker for disease elsewhere in the GIT tract
GASTRIC POLYPS • Neoplastic polyps – Types • Tubular • Villous (often larger - > 2 cm - and malignant) – Macroscopically • More often in antrum • Pedunculated with malignant potential • Solitary, large and ulcerated – Treatment • Endoscopic removal if no malignancy identified
GASTRIC POLYPS • Multiple gastric polyps – Rare condition • Adenomatous and hyperplastic polyps • 20% incidence f adenocarcinoma – Treatment • If confined to corpus and antrum – distal gastrectomy • Otherwise total gastrectomy
GASTRIC POLYPS – Sometimes associated with Polyposis syndromes • • • FAP Gardner Peutz-Jeghers Cowden Cronkhite Canada
GASTRIC LEIOMYOMA • Incidence of 16% at autopsy • Pathology – Arise from smooth muscle of the GIT tract • Difficult to distinguish from GIST – 75% benign • Differentiation only on mitotic index – Large protruding elisions with central ulcer
GASTRIC LEIOMYOMA • Usually presents with bleeding if at all • Treatment is local excision with 2 – 3 cm margin
GASTRIC LIPOMA • Rare subcutaneous lesions – Asymptomatic – On routine endoscopy – Require no treatment • Pillow sign
ADENOCARCINOMA OF THE STOMACH • Declining incidence in western world – HP associated due to chronic atrophic gastritis – Also related to • Low dietary intake vegetables and fruit • High dietary intake of starches • More common in males ( 3 : 1 )
ADENOCARCINOMA OF THE STOMACH • Histology – Invariably adeno-carcinoma – Squamous cell carcinoma from oesophagus • Involves fundus and cardia
ADENOCARCINOMA OF THE STOMACH • Histological typing – Ulcerated carcinoma (25%) • Deep penetrated ulcer with shallow edges • Usually through all layers of the stomach – Polipoid carcinoma (25%) • Intraluminal tumors, large in size • Late metastasis
Adenocarcinoma of the stomach – Superficial spreading carcinomas (15%) • Confinement to mucosa and sub-mucosa • Metastasis 30% at time of diagnosis • Better prognosis stage for stage
ADENOCARCINOMA OF THE STOMACH • Histological typing – Linitis plastica (10%) • Varity of SS but involves all layers of the stomach • Early spread with poor prognosis – Advanced carcinoma (35%) • Partly within and outside the stomach • Represents advanced stage of most of the fore mentioned carcinomas
ADENOCARCINOMA OF THE STOMACH • Symptoms and signs – Vague discomfort difficult to distinguish from dyspepsia – Anorexia • Meat aversion • Pronounced weight loss
Adenocarcinoma of the stomach • At late stage – Epigastric mass – Haematemesis usually coffee ground seldom severe – Metastasis • Vircho node in neck • Blumer shelf in rectum
ADENOCARCINOMA OF THE STOMACH • Surgical resection only cure – Late presentation makes sugary often futile – Palliation controversial for • Haemorrhage • Gastric outlet
ADENOCARCINOMA OF THE STOMACH – Simple gastrectomy as effective as abdominal block • Splenectomy often added due to direct involvement • Only for the very distal partial gestrectomy • Rest total gastrectomy • Prognosis overall 12% 5 year survival – 90% for stage I disease
GASTRIC LYMPHOMA • 5% of all primary gastric neoplasm's • 2 different types of lymphoma – Part of systemic lymphoma with gastric involvement (32%) – Part of primary involvement of the GIT (MALT Tumors) • 10 – 20% of all lymphomas occur in the abdomen • 50% of those are gastric in nature
GASTRIC LYMPHOMA • Risk factors – HP due to chronic stimulation of the MALT – In early stages of disease Rx of HP leads to regression of the disease
GASTRIC LYMPHOMA Primary MALT • Early stages also referred to as pseudolymphoma – Indolent for long periods – Low incidence of • Spread to lymph nodes • Involvement of bone marrow – Therefore much better prognosis
GASTRIC LYMPHOMA Primary MALT • Mostly involves the antrum • 5 different types according to appearance – Infiltrative – Nodular – Combination - Ulcerative - Polypoid
GASTRIC LYMPHOMA Primary MALT • At time of presentation – Larger than 10 cm (50%) – More than 1 focus (25%) – Ulcerated (30 – 50%) • Pattern of metastasis similar to gastric carcinoma • Signs and symptoms – Occur late and are vague – Relieved by anti-secretory drugs
GASTRIC LYMPHOMA Primary MALT • Treatment controversial – Surgical treatment for patients without systemic involvement • Mandatory for high grade lesions • Possible not needed for low grade lesions • Total gastrectomy and en-block for direct involvement – Sparing duodenum and oesophagus
GASTRIC LYMPHOMA Primary MALT – Palliative resection with intra-abdominal spread • Good for bleeding, obstruction and perforations – Radiation and chemotherapy combination for most
GASTRIC SARCOMA • 1 – 3 % of gastric malignancies • Include a wide variety of tumors – Leiomyosarcoma – Leiomyoblastoma – GIST
INTRODUCTION DUODENUM • • • Benign Brunners gland adenoma Leiomyoma Carcinoid Heterotopic gastric mucosa Villous adenoma Malignant • Peri-ampullar adeno CA – Duodenum – Cholangio – Pancreatic head • Leiomyosarcomas • Lymphomas Others • Duodenal d. Iverticula
DUODENUM Benign tumors • Brunners gland adenomas – Small submucosal • Sessile and pedunculated variants – Posterior wall junction D 1 and D 2 – Symptoms due to bleeding or onstruction • Leiomyoma – Asymptomatic
DUODENUM Benign tumors • Carcinoid – Mostly active (gastrin, SS and serotonin) – Simple excision
DUODENUM Benign tumors • Hetrotopic gastric mucosa – Multiple small mucosal lesions – No clinical significance • Villous adenoma – Intestinal bleeding – Obstruction of ampulla with jaundice – Risk of malignancy high (50%) – Endoscopic snaring or local excision
DUODENUM Malignant tumors • Located in the descending part of the duodenum • Symptoms – Pain, obstruction bleeding and jaundice – Earlier than pancreas head
Malignant tumours • Treatment – Pancreatico-duodenectomy for localized lesions • Much better prognosis than pancreas Ca (30% 5 year as opposed to 0%) – Palliative bypass procedures if not resectable – Radiotherapy for advanced disease ?