Well Span Surgery And Rehabilitation Hospital Print copies

Well. Span Surgery And Rehabilitation Hospital Print copies are not controlled Updated 11 Sep 2019

Well. Span Health Mission Working as one to improve health through exceptional care for all, lifelong wellness, and healthy communities.
 • Chosen by Well. Span Health • A means of")
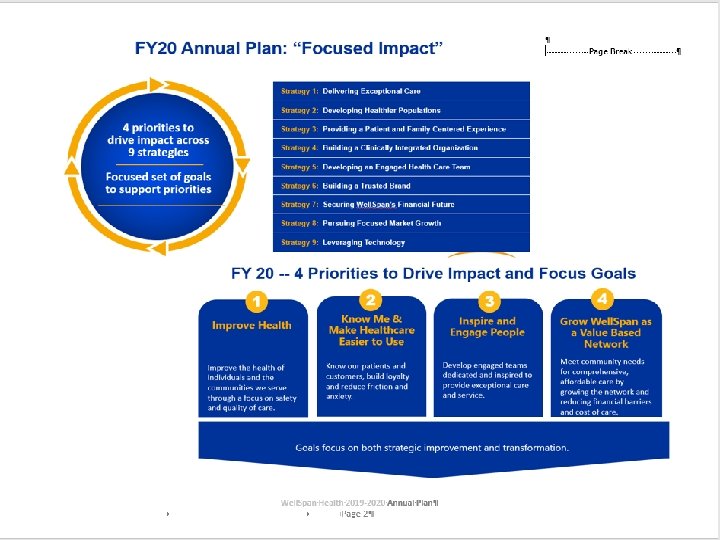
Wildly Important Goals (WIGs) • Chosen by Well. Span Health • A means of having all entities work on common goals • Current areas – Safety – Know Me (Patient‐related) – Employee Engagement – Access/Growth

Priority 1: Improve Health WIG: Safety – With the intent to eliminate avoidable harm, leverage the Leapfrog frameworks and pursue CMS 5‐stars performance. • With a two‐year goal of achieving an A rating or better for all rated hospitals, achieve a minimal Leapfrog B (predicted) rating at the end of FY 20. • All rated hospitals will achieve or maintain CMS 4 Star performance (per the WSH 12‐month calculator) at the end of FY 20.

Priority 2: Know Me & Make Healthcare Easier to Use WIG: KNOW ME – knowing the patient’s story – Continue to learn and apply what our patients tell us about themselves to create perfect patient experiences for every patient. Focus on: • Meeting individual preferences • Reducing points of friction and anxiety

Priority 3: Inspire and Engage People WIG: Employee Engagement • With the belief that providing an outstanding employee experience fuels an outstanding experience for those we serve, our focus will improve employee engagement in times of organization change throughout the lifecycle of our team members. – Communication: Create and execute a comprehensive communication strategy that inspires and connects staff members to the key aspects of change including the organization’s vision, mission, values, transformation and diversity/inclusion. – Change Management: Identify and utilize a consistent change management approach that provides resources for leaders and support to staff members in our changing environment. – Recognition: Enhance a culture of recognition through re‐vitalization of system‐wide recognition opportunities that provide a framework from entity‐ based and local recognition efforts.

Priority 4: Grow Well. Span as a Value‐ Based Network WIG: Access/Growth: Expand patient access to comprehensive local care

Well. Span Surgery and Rehabilitation Hospital Mission Supporting the journey to optimal health and independence by providing exceptional orthopedic, spine and acute rehabilitative care in a healing environment and coordinated through a comprehensive system of care.

Well. Span Surgery & Rehabilitation Hospital Victoria Diamond President, WSRH Controller David Martin Vice President Operations - WSRH Carol Smith , MSN, RN Department Chairs Director of Quality/ Regulatory Compliance Ruth Eckert , RN Medicine Dan Motter , DO Physical Medicine Rehabilitation Hugh Gregory, MD Surgery Craig Ruder , MD Nursing Practice Employee Health Patient Safety Peer Review Quality Regulatory Compliance Risk Management ISO Coordinator & Safety Officer Liaison Emergency Preparedness Director of Business Operations Director of Patient Care Services & Chief Nursing Officer Rosa Hickey , RN Chief Medical Officer Alyssa Moyer , MD Infection Control Pamela Goodling Rehab Nursing Magnet Coordinator Patient Experience Post Surgery Nursing Liaison Clinical Informatics Laboratory Pharmacy Respiratory Care Clinical Educator Pastoral Care Wound Care Dialysis Director of Inpatient Rehabilitation Elizabeth Trumble, PT Val Daniels PACU PHAS Pre. Op OR Scheduling Stage II Sterile Processing External Contracts Biomedical Engineering Supply Chain Facility Management -Engineering Facilities Specialists Housekeeping Laundry LDMS Rollout Food Services Liaison Imaging Admissions Business Development Liaison Services Prospective Payment System Rehab Coding Liaison Case Management Guest Services Volunteer Services HIMS Occupational Therapy Physical Therapy Speech Therapy Therapeutic Recreation Outpatient Rehabilitation Rehab Program Development -FIM -Outcomes -Specialty Designations Liaison Psychology
 Print copies are not controlled")
Our Cultural Pillars (Our Values) Print copies are not controlled

Peak Performance & Patient Centeredness Respect for All Working as One Assume Positive Intent Do the Right Thing Engaged Employees Supportive Leadership Structure Find a Better Way

Emergency Management Coordinator Steve Gibson

Fire Alarm Procedure • Remember, the Fire Alarm voice notification is to inform visitors of procedure, not staff • Report to your Charge Person/Home Department • Charge Person should account for Staff. • Clinicians should account for patients. • Await further instructions. • Don’t forget R. A. C. E. and P. A. S. S. Smoke/Fire Door Closure

Well. Span Surgery and Rehabilitation Hospital 55 Monument Rd York, PA 17403 FIRST FLOOR Security 812 -6555 B OR 3 OR 4 OR 1 OR 2 Meditation Room Entrance/Exit Stairs Exit Only Elevato r AED Pharmacy Smoke Compartment Outline A B Rally Points Training Room 9 La b PACU Imaging Stage II B 10 A 11 12 A Food Services -Engineering -Environmental Services -Receiving 3 15 Pre-Op Administration 16 2 Outpatient Surgery Exit 911 Response 1 st floor 1 Main Entrance 17 06/20 12

Well. Span Surgery and Rehabilitation Hospital 55 Monument Rd SECOND FLOOR York, PA 17403 Observation Rooms Therapy Garden Exit Only Elevator Rooms 2401 2421 4 Therapy Gym 7 Rehab Patient Entranc e 5 25 Bed Post Surgical Unit Stairs 911 Response 2 nd Floor Security 812 -6555 Rooms 2201 2207 Entrance/Exit C C D Rally Points AED 8 Bed Brain Injury Unit 8 6 ADL Apartmen t Smoke Compartment Outline Patient Dining Rooms 2501 2508 D D Activity Rooms 2101 - 2118 C Rooms 2301 - 2318 40 Bed Inpatient Rehab Unit 06/20 12
 – – • ASCOM Phone (Portable)")
Emergency Communications • Avaya IP Phone (Desk Phone) – – • ASCOM Phone (Portable) – – • Component Failure On Emergency Power Send and Receive outside calls Personal Distress Emergency Overhead Page – – • • • Network Outage Power Outage On Emergency Power 6 Placed throughout WSRH To be used only if everyone needs to know immediately Key to be kept in area of mic Emergency Phones Radios When All else fails, RUNNERS

DISASTER CODE MATRIX *The External Disasters emergency code will only be initiated by WSRH Facilities and/or WSRH Administration.

HAZARDOUS MATERIALS & WASTE • Hazardous Materials – Types of Hazardous Materials – – Oxygen Natural Gas Cleaners Formulin • Hazardous Waste – Types of Hazardous Waste – – Regulated Medical Waste Chemo Therapy Waste Pharmaceutical Waste Solid Waste (Batteries and Light Bulbs) • SDS System • Accessible via the INET SDS SHEETS – Waste Collected by Staff and Contractors. • Hazardous Materials Room is the collection point.
 Disposed of in black hazardous waste bins • The bins")
Pharmaceutical Waste Medications (MEDS) Disposed of in black hazardous waste bins • The bins are not meant for: – Regular trash – Needles or other sharps – Controlled substances (Rx Destroyer) • The lids to the black hazardous waste bins should remain closed. • The bins are located in secure areas by the automated dispensing machines (PYXIS)

Medical Gas Zone Valves • Medgas ON, cover fits. • Medgas OFF, cover will not fit. • The Charge Nurse or Designee is responsible for Medical Gases in an emergency. • Know where the panels are in your work area • If you have any questions, contact Maintenance.

AEDs • There are three AEDs in the building – By the vending machines – By the receiving dock in back of house – On the second floor next to the Activity Room door (near the public elevators)

General Evacuation • • • EVAC Devices • Await instructions to evacuate the building. Horizontal Relocation then Vertical. Move at least one set of Smoke and Fire doors away if your area is evacuated Know who is to “clear” your area. – Charge Nurse/Area Supervisor will designate who will “clear” the area (Room by room). • • • Rally Point Use the Cleared signs (All areas but Surgical Services) Surgical Service uses orange cones at foot of the room. Know your rally point (Door Number and Letter). Bring your ASCOM phone and a WOW. Remember a fire alarm does not mean you have to evacuate. Know your smoke compartments.

Ruth Eckert, RN Director of Quality & Regulatory Compliance • • Patient Safety Officer Chair of Patient Safety Committee Risk Manager Management Representative (ISO) Print copies are not controlled
 Through Feb 2020 Entire hospital Annual")
Accreditation Det Norske Veritas – Germanischer Lloyd (DNV-GL) Through Feb 2020 Entire hospital Annual and unannounced survey Commission on Accreditation of Rehabilitation Facilities (CARF) Through Nov 21 Rehab side only; specialty accreditation Comprehensive Adult Inpatient Rehabilitation Brain Injury Stroke Amputee Spinal Cord

DNV GL Accreditation • Standards are called National Integrated Accreditation for Healthcare Organizations (NIAHO ®) • First integrated accreditation program in US – CMS Conditions of Participation for Hospitals – ISO 9001 Quality Management System requirements
 – A")
What is ISO? • ISO = the organization (International Organization for Standardization) – A network of 163 member countries – Focused on International standards • ISO = the standards (9001: 2015) – A minimum set of quality standards – Not Healthcare specific: Applicable to all types of organizations – Not very prescriptive

Seven Quality Management Principles of ISO 9001: 2015 1. 2. 3. 4. 5. 6. 7. Customer Focus Leadership Engagement of people Process approach Improvement Evidence-based decision making Relationship management

Your Role in ISO 9001: 2015 • Customer Focus – Know your direct and indirect customers: patients, families, visitors, co ‐workers, supervisors, other departments – Understand their needs and expectations – Be aware of your patient satisfaction scores from Press Ganey – Ensure new processes are designed with the patient in the center • Leadership – Know the organization’s mission, vision, strategies, policies and processes throughout the organization – Follow the WSRH Cultural Pillars – Be committed to quality – SPEAK UP if you see any issue

Your role continued • Engagement of People – Promote collaboration throughout the organization – Identify opportunities for improvement in your department and WSRH – Work with your supervisor/manager to create goals to facilitate your personal and professional development – Fill out the Employee Engagement Survey from Well. Span • Process approach – Know if workflows or standard work have been created for the work you do • Follow the workflows or standard work • If you identify an issue/difference between your practice/work and the workflow – SPEAK UP – Let your supervisor/manager know if there is a process that needs to have standard work created

Your role continued • Improvement – SPEAK UP when you see an opportunity for improvement – Participate in department huddles – Be a problem solver • Evidence-based decision making – Ask to see the data/metrics from your department – Use the data to drive process improvement • Relationship management – Share concerns or satisfaction with vendors, suppliers

Your role continued • Control of Documents – Put expiration dates on any created materials – Toss posted materials that are expired – Do not keep copies of printed policies • Print Use Discard DO NOT HOARD PRINTED DOCUMENTS • Ensure you are using the most current version of the document, form etc • Notify supervisors/managers of any identified defects (any where) – Complete SRS report when you identify an unexpected occurrence or event – Bring the issue up at your department huddles (Heads Up, Speak Up)

Patient Safety – Act 13 Print copies are not controlled

Definitions in Act 13 • • • Health Care Worker - An employee, independent contractor, licensee or other individual authorized to provide services in a medical facility Incident - An event, occurrence or situation involving the clinical care of a patient in a medical facility which could have injured the patient but did not either cause an unanticipated injury or require the delivery of additional health care services to the patient. The term does not include a serious event. Infrastructure failure - An undesirable or unintended event, occurrence or situation involving the infrastructure of a medical facility or the discontinuation or significant disruption of a service which could seriously compromise patient safety. Serious Event - An event, occurrence or situation involving the clinical care of a patient in a medical facility that results in death or compromises patient safety and results in an unanticipated injury requiring the delivery of additional health care services to the patient. The term does not include an incident. Sentinel Event - A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. (Joint Commission) Print copies are not controlled

Requirements of Act 13 • Patient Safety Officer – Ruth Eckert • Patient Safety Committee – 2 nd Thursday of every month – Open to anyone who wants to come • System to report serious events and incidents that is accessible 24/7 – Safety Reporting System (SRS) • No retaliatory action against a health care worker for reporting a serious event of incident • Written notification to the patients/family Print copies are not controlled

Reporting • Event Reports are to be made immediately or as soon as reasonably practicable – MUST be NO later than 24 hours after the occurrence or discovery of a serious event of incident • If you are not sure what to do, call Ruth – Desk phone 812 -6153 – ASCOM phone 812 -6453 Print copies are not controlled

Patient Safety • Events are to be reported in the Safety Reporting System – Link is on the INET home page – Connects to PAPSRS (PA Reporting System)

Patient Safety • Just Culture – A safety-supportive system of shared accountability • Management is accountable for good system design and responding to the behaviors of their staff in a fair and just manner • Staff members are accountable for the quality of their choices and for reporting errors, adverse events, and system vulnerabilities • Crew Resource Management – Stop the line concept: any team member can/should ask for clarification or interruption of a process when s/he perceives an Immediate Risk to Patient Safety – Staff must feel empowered to use it! Print copies are not controlled

Regulatory Issues • Tobacco – free – No use of tobacco in any form on campus, including in your cars – Include vaping, e‐cigarettes • Badges – Must be worn above your waist – Quick release lanyards – No defacing eg stickers – If you forget yours, get a temporary one
 Law allows new parents to surrender their newborn within")
Safe Haven (PA Act 201) Law allows new parents to surrender their newborn within 28 days of birth, ANONYMOUSLY, that is not a victim of abuse or criminal activity. – Any employee can accept; volunteers cannot – Confirm that the parent is surrendering their infant to you. – Contact 911 to have the baby taken to YH Emergency Department via Ambulance for further care. – If there is an indication of abuse, also notify Police

Adult Protective Services Act of 2010 • Provides protection of adults who are abused, neglected, exploited or abandoned • 18‐ 59 • Physical/mental impairment limiting 1 or more major life activities • Actions to take – Assure the individual’s health & safety – REPORT – See WSRH Policy, Abuse of Vulnerable Populations, for details – Please notify Ruth if you are concerned any of these situations exist

WSRH Risk Management • Proactive rather than reactive – Need to identify and report “Good Catches” – Notify Employee Health if you are injured • Risk Manager is Ruth Eckert

Top Physical Environment/Safety Items 1. Keep your area clean and clutter‐free. 2. Keep overhead storage at least 18 inches below the sprinkler heads. 3. DO NOT prop open doors. 4. DO NOT block fire doors, pull stations or extinguishers. 5. Keep corridors and hallways free from obstructions. 6. Medical devices must be checked by Biomedical. 7. Personal plug‐in devices must have a safety check 1 2 3 4 6 5

Security Management • WSRH Security Department – Call 812 -6555 • Security Considerations – Park in designated areas. • Please ensure your vehicle(s) are registered with Well. Span Health • Please use your Well. Span hangtag in your vehicle – Security can escort you to your car – Don’t allow individuals to “tailgate” through access controlled doors. • If someone is lost, give them directions to appropriately enter the facility or area
 • Zero Tolerance: patient staff, staff patient, staff, visitors patients, etc")
Workplace Violence (WPV) • Zero Tolerance: patient staff, staff patient, staff, visitors patients, etc • Categories: – Threat – Near Miss – Actual Event with or without injury • Reporting – All categories are to be reported – SRS report must be filed for an actual event with injury – All others may be reported using the worksheet on the forms section of the WSRH portal

WPV • You will get an email with information related to documents for you to read – Brochure – A statement to sign and return • Task Force – Multidisciplinary volunteer group – Looking for more volunteers

Process Improvement • You are encouraged to identify opportunities for improvement – What is not working? – What frustrates you? – What do could be done better? • Everyone is encouraged to speak up Print copies are not controlled

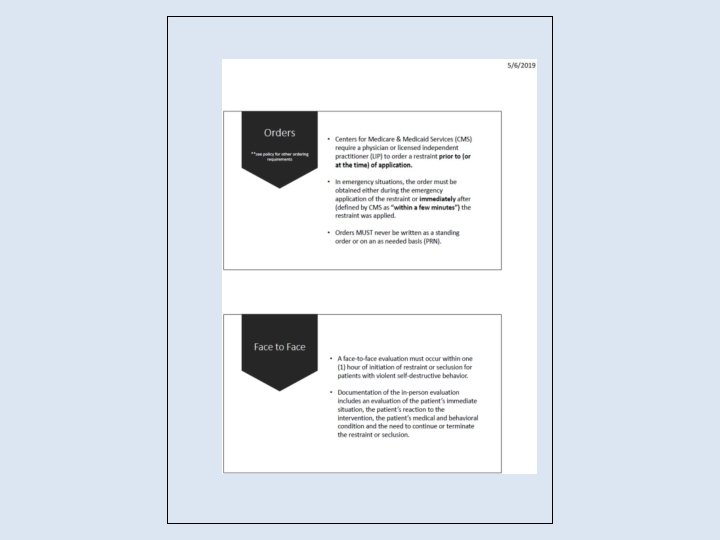
https: //portals. wellspan. org/sites/wsnursing/System%20 Policies/Practice%20 and%20 Quality/SYS‐ PQ%20 Restraint%20 Policy. pdf





Pam Goodling • Manager Infection Control and Prevention Print copies are not controlled

Infection Control Basics Print copies are not controlled

Why Is Hand Hygiene So Important? • Thousands of people die every day around the world from infections acquired while receiving health care. • Hands are the main pathways of germ transmission during health care. • Hand hygiene is therefore the most important measure to avoid the transmission of harmful germs and prevent health care‐associated infections. Print copies are not controlled

Why should you clean your hands? • Any health‐care worker, caregiver or person involved in patient care needs to be concerned about hand hygiene • Therefore hand hygiene concerns you! • You must perform hand hygiene to: üprotect the patient against harmful germs carried on your hands or present on his/her own skin üprotect yourself and the health‐care environment from harmful germs Print copies are not controlled

Hand Hygiene – Observations • All staff must perform hand hygiene upon entering the patient’s room. • All staff must perform hand hygiene upon exiting the patients room. • If patient is not in their room, hand hygiene must be performed before contact with the patient. Print copies are not controlled

Hand Hygiene and Glove Use – The use of gloves does not replace the need to clean your hands! – You should remove gloves to perform hand hygiene, when an indication occurs while wearing gloves – You should wear gloves only when indicated otherwise they become a major risk for germ transmission Print copies are not controlled

Fingernails and Artificial Nails • Natural nail tips should be kept to ¼ inch in length • Artificial nails should not be worn when having direct contact with patients and patient care items. • Nail length is important because even after careful handwashing, HCWs often harbor substantial numbers of potential pathogens in the subungual spaces. Guideline for Hand Hygiene in Health-care Settings. MMWR 2002; vol. 51, no. RR-16. 60

Standard Precautions • Use for the care of all patients • You never now what is lurking in the next room • Use standard precautions whenever there is a chance you’ll be exposed to: – Blood – Any other body fluids, secretions, or excretions – Nonintact skin (broken skin) – Mucous membranes • Respiratory etiquette Print copies are not controlled

Why is Adherence to Standard Precautions So Important? • Because colonization with multidrug resistant organisms (MDROs) is often unrecognized (e. g. , MRSA, VRE, CRE, ESBL, etc. ). – We can’t screen for every possible MDRO. • Because other infectious organisms may spread (e. g. coagulase-negative Staph. , MSSA, Serratia species, Pseudomonas species, Klebsiella species etc. ) Print copies are not controlled

Respiratory Etiquette • Observe Droplet Precautions (i. e. , wearing a surgical or procedure mask for close contact), in addition to Standard Precautions, when close contact with a patient with symptoms of a respiratory infection, particularly if fever is present. These precautions should be maintained until it is determined that the cause of symptoms is not an infectious agent that requires Droplet Precautions Print copies are not controlled

Dirty Patient Care Equipment/Items is a Source of Indirect Transmission of Microorganisms • Equipment that is contacting the patient and/or the patient environment should be properly cleaned between patients with a Well. Span approved disinfectant wipe between patients. Print copies are not controlled

Other MDRO • • Fluroquinolone-resistant P. aeruginosa Erythromycin-resistant S. pneumonia Carbapenem-resistant S. marscens Extended spectrum ß-lactamase, E. coli, K. pneumoniae (ESBL) • CRE (Carbapenemase-producing Enterobacteriaceae Print copies are not controlled

The Iceberg Effect Infected Colonized • This iceberg graphically represents colonization versus infection. Those patients that are infected with an organism represent just the “tip of the iceberg” of patients that are colonized or infected. • Just because a patient is not infected, or showing signs of infection, does not mean that they do not carry organisms that could be transferred to another patient if proper hand hygiene and other infection control precautions are not taken. Print copies are not controlled

Standard Precautions • Patients with MDROs can be cared for using Standard Precautions if they have contained secretions/excretions. • Secretions/excretions (including wound drainage, stool and urine) are contained when they are unable to leak out of containment products (e. g. , wound dressings, incontinence product, urine bags, ostomy bags, etc). Print copies are not controlled

Print copies are not controlled 68

C. diff • Patients suspected with or confirmed with C. diff will require contact precautions. • Once positive, the patient must remain in precautions until cleared by a member of the Infection Prevention Team • Test of cure should NOT be performed for the purposes of treatment or to justify discontinuing isolation Print copies are not controlled

C. difficile Protocol • Contact Precautions as soon as testing is ordered (purple octagon for C. diff). • If assay negative ‐ consider other pathogens before removing from precautions. • The disease is from ingestion of the organism not in the air or general contact Print copies are not controlled

C. difficile Protocol • If assay is positive, keep on precautions until pt has “normal” stools x 48 hrs – Do not test for cure! – Room must be terminally cleaned prior to removing patient from Contact Precautions – Leave the sign in place until housekeeping has designated the room clean and ready for use. Print copies are not controlled

Overly resistant • Multi‐drug resistant organisms may cause a significant risk to patients. MDROs are ever changing and emerging. • Current examples – Any Vanco Resistant or Intermediate Staph aureus (VISA/VRSA) – Resistant Acintobacter in the respiratory tract (especially in our ventilated patient population) – Carbapenem‐resistant Enterobacteriaceae (CRE) Print copies are not controlled

uncontained wound • This can be a little tricky, what is uncontained? • When wounds are open and draining and are not contained within a dressing (particularly when infected i. e. bed sores, ulcerations, etc), there is a risk of spread REGARDLESS of the organism. • This is a clinical decision that needs to be made with nursing and providers. • Please consult with the Infection Prevention Team as needed. Print copies are not controlled

Trach w/ increased • Those patients with open trachs and/or open suctioning that are showing increased secretions require isolation. The offending organism is not the driving factor. • This is a clinical decision that needs to be made with nursing and providers. • Please consult with the Infection Prevention Team as needed. Print copies are not controlled

Acute onset • C. diff is not the only cause of acute diarrhea. • Norovirus (as well as other viruses) may cause acute onset diarrhea and is highly contagious to both patients and staff. • It is important to separate the normal “loose” stools that some patients may be prone to from uncontained acute onset diarrhea. • When seeing an unexplained acute onset diarrhea, place those patients on contact precautions. Print copies are not controlled

• For patients with a MDRO in their urine who: – Do NOT have a Foley catheter – Are incontinent and urine cannot be contained by a brief Print copies are not controlled

think • No lab finding or algorithm can replace the critical thinking and judgment of a health care professional. There will be times that will seem appropriate to place enhanced precautions on a patient. • The patient’s team needs to be open and discuss concerns to ensure that our patients are safe. • When in doubt, do it! Print copies are not controlled

Discontinuing Contact Precautions • When the condition of the patient with an MDRO changes (e. g. , drainage contained) and they therefore no longer meet the criteria for requiring Contact Precautions, they may be cared for using Standard Precautions. • Before removing any patient from Precautions the Infection Preventionist must be consulted (ASCOM ext. 26489). Print copies are not controlled

Automatic Isolation Orders • An automatic order for precautions is triggered for the following laboratory testing: – C. difficile – Contact Precautions – Influenza AB RSV PCR – Droplet & Contact Precautions – Respiratory Viral Detection Panel – Droplet & Contact Precautions • If RSV positive maintain the patient on Contact and discontinue the Droplet. • If RSV negative but positive to any other respiratory virus, maintain Droplet and discontinue Contact. Print copies are not controlled

Stop Sign • The Stop Sign is used for any patient placed on Contact, Droplet, Airborne or Neutropenic. • It is an alert for staff to check Room Link for the specific type of Precautions the patient is on. • It is also an alert for visitors to stop at the nurses station for instruction on any type of precautions they must take before entering the patient’s room. Print copies are not controlled

Contact Precautions Signage for C. difficile • When the order is triggered the Room Link will display Contact Precautions. • In addition to the STOP Sign a purple octagon indicating Contact Precautions for C. difficile

Transmission‐Based Precaution Signage 82

Contact Precautions • Perform hand hygiene • Gown and gloves MUST be worn when entering patient room for any reason. • Change gloves after having contact with material that may contain high concentrations of microorganisms. • Remove PPE before leaving patient room. • Perform hand hygiene immediately after glove removal Print copies are not controlled

Droplet Precautions • Perform hand hygiene • Use Standard Precautions in addition Droplet Precautions. • Mask and Eye Protection – Must be worn to enter the room – Eye glasses do not provide adequate protection – Wear a procedure mask with attached eye shield. • Patients must don a surgical mask and perform hand hygiene prior to leaving their room • Remove your PPE before leaving patient room. • Perform hand hygiene immediately after PPE removal Print copies are not controlled

Airborne Precaution Protocol • Mask the patient with a isolation mask. • Contact Infection Control ASCOM# 26489. • Call Facilities at ext. 26555 to have the negative air room turned on. • Ensure that the room is functioning. • Transfer patient to negative air room. Print copies are not controlled

BIOHAZARDOUS WASTE • Laboratory waste • Human surgery specimens or tissues • Items saturated or dripping with blood or • OPIM or caked with dried blood or OPIM. • Waste containing discarded material contaminated with excretion, exudates or secretions from humans who are isolated for Biosafety Level 4 pathogens such as Ebola, Lassa or Marburg viruses. Print copies are not controlled

Non‐Medical Waste Medical waste does not include: • Urine, feces, saliva, sputum, nasal secretions, sweat, tears, or vomitus, unless it contains fluid blood • Waste which is not biohazardous, such as articles containing nonfluid blood and other medical solid waste products commonly found in hospitals Print copies are not controlled

How to reach me. . . • I can be reached by at ASCOM phone # 26489 Monday thru Friday, 7 am – 3: 30 pm • After hours I can be contacted by leaving a message on my voice mail. This will initiate an email to my PDA that someone has left a message. • If it is an emergency after hours contact the operator and have her contact the Infection Preventionist on call • When I am out of the office there will a voice message directing you to call the IC main extension # 12251. Print copies are not controlled
- Slides: 88