Cerebrovascular Disorders Department of Neurosurgery Faculty of Medicine


Cerebrovascular Disorders Department of Neurosurgery Faculty of Medicine, Alexandria University

Cerebrovascular Diseases Stroke It is a heterogenous category of illness that describes brain injury, usually sudden, caused by vascular disease.

Cerebrovascular Diseases Stroke Epidemiology: n. Vascular diseases are one of the most frequent causes of admission to hospital. n. The third leading cause of death and primary cause of disability in USA. n A disease of the elderly - 5/1000 in the 5 th decade - 20/1000 in the 7 th decade

Cerebrovascular Diseases Stroke Risk factors: 1. 2. 3. 4. 5. 6. 7. Hypertension. Heart disease. Diabetes mellitus. Hereditary factor. High blood lipid. Alcohol and drugs Age, sex, race, family history
 - Transient ischemic attacks (TIAs)")
Cerebrovascular Diseases Classification 1 - Ischemic stroke (80 -85%) - Transient ischemic attacks (TIAs) - Reversible ischemic neurologic deficit (RIND) - Stroke in evolution - Complete stroke 2 - Hemorrhagic stroke (10 -15%) - Intracerebral hemorrhage (ICH) - Subarachnoid hemorrhage (SAH)

Cerebrovascular Diseases Stroke Etiology: A. Ischemic stroke: 1 - large vessel atherosclerosis 2 - penetrating artery disease (lacunar infarction) 3 - cardioembolism 4 - systemic hypoperfusion 5 - others (fat embolism, air embolism, tumor emboli)

Cerebrovascular Diseases Etiology: Stroke B. Hemorrhagic stroke: SAH and ICH may be: n Primary ICH (hypertensive) n Secondary ICH: 1 -Aneurysm and AVM 2 - vasculopathy 3 - coagulopathy 4 - intracerebral tumor 5 - drug abuse 6 - others

Cerebrovascular Diseases Stroke Clinical picture of ischemic stroke These are classified into: - T. I. A. (Transient Ischemic Attacks) - R. I. N. D. (Reversible Ischemic Neurological Deficit) - Incomplete stroke - Complete stroke
 - Episode which are sudden")
Cerebrovascular Diseases Stroke T. I. A. (Transient Ischemic Attacks) - Episode which are sudden in onset, resolve within 24 hours or less. - It leaves no residual deficit.
: - It lasts")
Cerebrovascular Diseases Stroke R. I. N. D. (Reversible Ischemic Neurological Deficit): - It lasts more than 24 hours, but resolve within one week.

Cerebrovascular Diseases Stroke Incomplete stroke: - This results in persistent residual symptoms, that are not disabling, e. g. incomplete paresis, and dysphasia.

Cerebrovascular Diseases Stroke Complete stroke: - Typically, it results in profound multimodal neurologic deficit. Such as: - hemiplegia. - hemianopia. hemisensory effect.

Cerebrovascular Diseases Stroke Clinical picture of ischemic stroke: Neurological manifestations dependent on the vessel involved: - carotid territory - vertebrobasilar territory - both carotid and vertebrobasilar

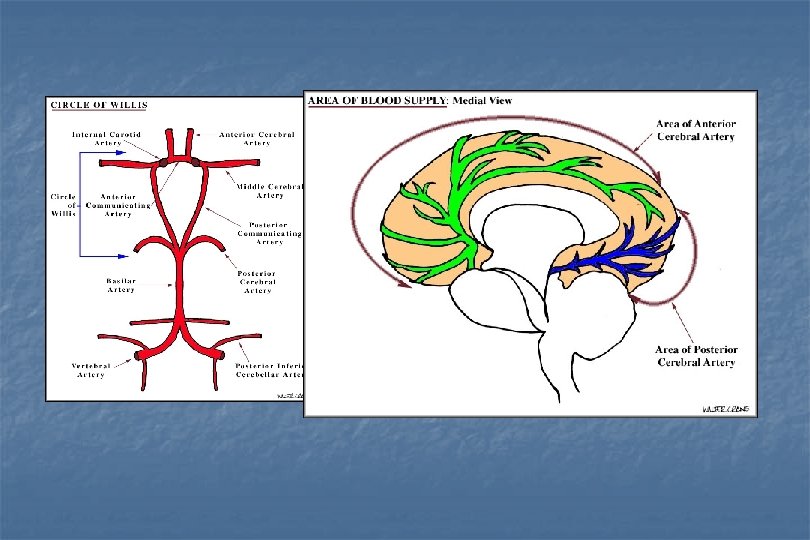
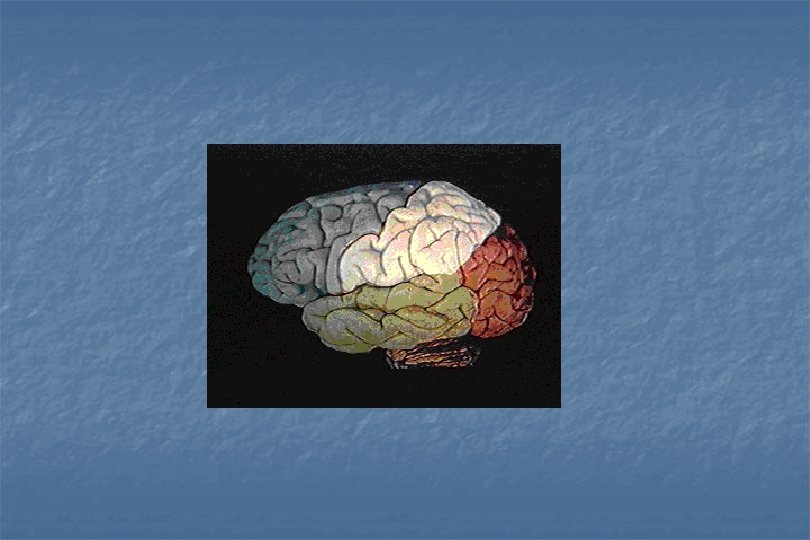
Cerebrovascular Diseases Blood supply of the brain Lateral view Medial view

Cerebrovascular Diseases Stroke Clinically: A. Affecting the carotid territory: - Reduction in retinal perfusion leading to transient monocular blindness (Amourosis Fugax). - Reduction in cerebral perfusion leading to hemiparesis, hemianaesthesia, and dysphasia.

Cerebrovascular Diseases Stroke Clinically: B. Affecting the vertebrobasilar territory: : - Binocular visual disturbance, diplopia, and nystagmus. - Bilateral weakness, and may be loss of consciousness. Vertigo, ataxia, deafness, and tinnitus. In this type, there is transient ischemia of the brain stem, occipital lobes, medial temporal lobes, and the upper spinal cord.

Cerebrovascular Diseases Stroke n Clinical picture of hemorrhagic stroke: 1 - focal neurological deficits (putamenal = 35%, lobar = 25%, thalamic = 20%, caudate, pontine & cerebellar = 7% each) 2 - manifestations of ↑ ICP 3 - change in the level of consciousness 4 - headache, neck stiffness (in SAH)

Cerebrovascular Diseases Stroke Diagnosis of stroke: 1. History and examination: - Will point to which arterial territory is affected. Number and frequency of episode. Underlying cardiac disease. Risk factors. 2. Investigations A- laboratory B- ECG

Cerebrovascular Diseases Stroke Diagnosis of stroke: 3. radiological: n chest X ray n computed tomography (CT), CT angiography (CTA) n magnetic resonance imaging (MRI) n magnetic resonance angiography (MRA) n Digital substraction angiography n Doppler ultrasound (carotid and transcranial) n functional studies

CT MRI

CTA Rt ICA stenosis Lt ICA stenosis

MRA Rt ICA stenosis Lt ICA stenosis

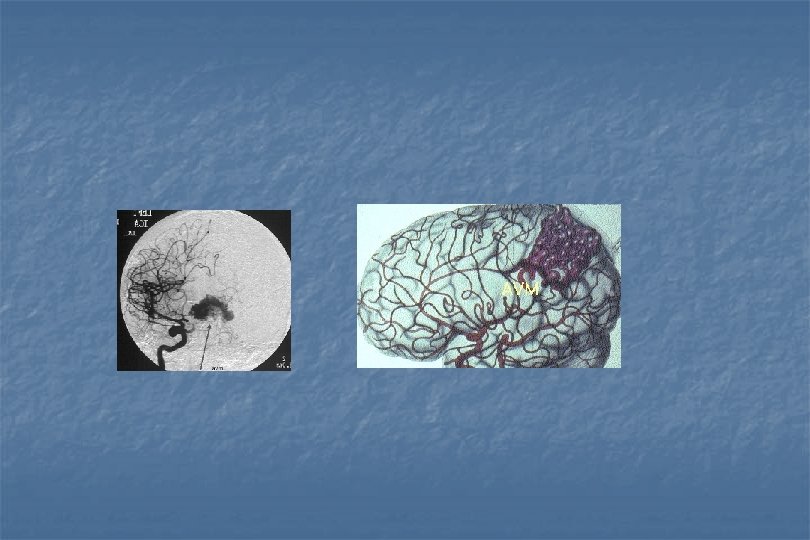
DSA Lt ICA stenosis AVM

Doppler Ultrasound
 -")
Cerebrovascular Diseases Stroke Treatment of ischemic stroke: A. medical: - Thrombolytic agents (TPA) - Antithrombotic therapy: Antiplatlet (aspirin), Anticoagulant (heparin and oral anticoagulant) - Medical treatment for the risk factors.

Cerebrovascular Diseases Stroke Treatment of ischemic stroke: B. surgical: - carotid endarterectomy - intracranial embolectomy - extracranial-intracranial bypass - decompressive procedures - surgical treatment of cerebellar infarction - endovascular procedures

Cerebrovascular Diseases Stroke Treatment of ICH: A. medical n n n care of respiration fluids, electrolytes and nutrients antiepileptic medication antihypertensive medication control of intracranial pressure

Cerebrovascular Diseases Treatment of ICH: Stroke B. surgical n n n continuous ventricular drainage craniotomy burr hole aspiration stereotactic thrombolysis and aspiration endoscopic evacuation

Cerebrovascular Diseases Treatment of ICH the choice of the method of treatment: A. Supratentorial heamatoma: - Surgical evacuation is indicated if the heamatoma is sizable and superficial, and the patient is clinically acceptable. However, conservative treatment is indicated for deep small heamatoma. B. Cerebellar hematoma: - Urgent evacuation through posterior fossa exposure. As relief of the brain stem compression may be life saving. C. Pontine hematoma: - Mortality rate is high, a conservative approach is usual.
: - Medical")
Cerebrovascular Diseases Treatment of SAH 1 - treatment of the cause (Aneurysm): - Medical treatment - Surgical treatment - Endovascular treatment 2 - treatment of complications: - rebleeding - vasospasm - hydrocephalus - seizures
 1.")
Cerebrovascular Diseases Subarachnoid Hemorrhage Treatment: A. Medical: (to prepare the patient for surgery) 1. 2. 3. 4. 5. 6. 7. Immediate bed rest, sedation and analgesics. Triple-H therapy: Hypertension, hemodilution and hypervolemia. Oxygenation. Corticosteroids. Stool softener and H 2 antagonist. Antiepileptic drugs. Calcium antagonists: Nimodipine( Nimotop) to prevent vasospasm by its effect in the smooth muscles of the blood vessels.

Cerebrovascular Diseases Subarachnoid Hemorrhage Treatment: B. Surgery: micro surgical treatment 1 - Clipping of the aneurysm. 2 -Trapping (put 2 clips and it will thromboses). 3 - Wrapping (strengthen the wall by for example acrylic substance) of the aneurysm. 4 - Proximal ligation (not done now). C. Endovascular surgery Induce thrombosis : using coils or balloons,

Cerebrovascular Diseases Arterio-Venous Malformation Treatment: 1. Microsurgical treatment: Complete excision. 2. Endovascular surgery: Selective embolization of the feeder vessels, so the AVM will shrink. 3. Stereotactic radiosurgery: using the gamma knife or Linac. Very effective for inoperable cases as that of brain stem and basal ganglion.

Cerebrovascular Diseases Stroke Complications 1 - venous thromboembolism and myocardial infarction 2 - pneumonia 3 - limb contractures 4 - bed sores 5 - depression
 3106023")
Data show design & preparation by : Dr. El-Sayed Amr - (012) 3106023



Cerebral Aneurysm

Cerebrovascular Diseases Cerebral Aneurysm Incidence: - It is 1% of autopsy brain. Incidence of ruptured aneurysm is less. In 10% of autopsied brain we can find small aneurysm <2 mm.

Cerebrovascular Diseases Cerebral Aneurysm Pathology: - It is a congenital defect in the tunica media and elastic membrane at the apex of the vessel when it bifurcates. The aneurysm may bleed at any time but the age usually between 40 -60 years (age of presentation).

Cerebrovascular Diseases Cerebral Aneurysm Site: Anterior circulation aneurysm 85% Anterior communicating artery is the commonest. The internal carotid is next (carotid cave, ophthalmic, and carotid siphon). The junction of the internal carotid and posterior communicating arteries. Anterior cerebral artery. Posterior circulation aneurysm 15% Tip of the basilar artery. Superior cerebellar artery. PICA (posterior inferior cerebellar artery). Middle cerebral artery. AICA (anterior inferior cerebellar artery). Vertebral artery.

Cerebrovascular Diseases Cerebral Aneurysm Clinical picture of cerebral aneurysm: 1. Asymptomatic. 2. Pressure symptoms: a. on the brain: especially big tumors (as brain tumors), usually presents with migraine attacks (4% of migraine patients suffer from aneurysm), and 5% presents with epilepsy. In addition to vomiting and headache. b. on the cranial nerves: commonest nerve is the 3 rd nerve ® ptosis or opthalmoplegia "superior orbital fissure syndrome" (diabetes mellitus can cause the same). 3. Leakage or rupture lead to SAH or - Rupture ® immediate death or Leakage ® warning and after 2 3 weeks ® immediate death.

Cerebrovascular Diseases Subarachnoid Hemorrhage Symptoms First grade: just a sudden severe excruciating headache, vomiting, dizziness, neck stiffness or pain radiating to the back of the neck may be associated due to meningeal irritation by the blood. It is mistaken as meningitis but here high fever not mild and it is not sudden. Second grade: may be momentary loss of consciousness then recovery. This stage is missed in diagnosis (1 st and 2 nd stages). Third grade: sudden coma preceded severe headache then recovery with neurological deficit (unilateral). Fourth grade: sudden coma with no recovery with bilateral neurological deficit.
, due")
Cerebrovascular Diseases Subarachnoid Hemorrhage On Examination a. mild pyrexia (37. 5 o-38 o), due to blood in the subarachnoid space. b. signs of meningitis: neck stiffness, Kernig's sign, and Brudzinski's sign are all positive.

Cerebrovascular Diseases Subarachnoid Hemorrhage Diagnosis: 1. Classical history of sudden severe headache at 40 th, 50 th, or 60 th followed by neck stiffness. 2. If lumbar puncture is done give red color CSF, and after 2 -3 days it become xanthochromic. 3. Clinical examination: mentioned before.

Cerebrovascular Diseases Subarachnoid Hemorrhage Investigations a. Lumbar puncture: - It is diagnostic if there is no CT scan. - If immediately done, it will show fresh blood. - If few days later, the picture will be xanthochromic.

Cerebrovascular Diseases Subarachnoid Hemorrhage Investigations b. CT scan: - Hyperdense shadow in the plain CT, and its density like that of bone at the site of one of the bifurcating vessels. - The CT scan guide to the cause of bleeding or the site of the aneurysm.
: - Nowadays digital subtraction angiography which")
Cerebrovascular Diseases Subarachnoid Hemorrhage Investigations c. Arteriography (angiography): - Nowadays digital subtraction angiography which is computerized arteriography is very helpful. - It can be done through the anti cubital or femoral vein, we introduce a catheter. - It is considered as an invasive technique but its hazards are less and give more details. N. B. in occlusive stroke, we can dissolve thrombus though a catheter.

Cerebrovascular Diseases Subarachnoid Hemorrhage Investigations d. MRA: - It is a non invasive technique, noting is injected. - It helps in the diagnosis of aneurysm, AVM, hemorrhage in a tumor. - It is to be used in cases when spasm is suspected.

Cerebrovascular Diseases Subarachnoid Hemorrhage Complications: - Rebleeding, and usually occurs in 30% of the patients who bleed in the first 2 weeks, and 50% bleed before the first year. Vasospasm due to blood in the subarachnoid space and it may cause loss of consciousness. 25% of the patients shows vasospasm, half of them die and the other half have permanent deficit. Hydrocephalus whether communicating or non communicating type. Seizures. N. B. : if an aneurysm is treated conservatively, only 25 out of 100 escape death during the first year.
 1.")
Cerebrovascular Diseases Subarachnoid Hemorrhage Treatment: A. Medical: (to prepare the patient for surgery) 1. 2. 3. 4. 5. 6. 7. Immediate bed rest, sedation and analgesics. Triple-H therapy: Hypertension, hemodilution and hypervolemia. Oxygenation. Corticosteroids. Stool softener and H 2 antagonist. Antiepileptic drugs. Calcium antagonists: Nimodipine( Nimotop) to prevent vasospasm by its effect in the smooth muscles of the blood vessels.

Cerebrovascular Diseases Subarachnoid Hemorrhage Treatment: B. Surgery: micro surgical treatment 1 - Clipping of the aneurysm. 2 -Trapping (put 2 clips and it will thromboses). 3 - Wrapping (strengthen the wall by for example acrylic substance) of the aneurysm. 4 - Proximal ligation (not done now). C. Endovascular surgery Induce thrombosis : using coils or balloons,

AV Malformation

Cerebrovascular Diseases Arterio-Venous Malformation It is a developmental anomaly of intracerebral vessels due to lack of capillary network leading to shunt formation, which will pass the blood directly to the venous system. Pathological types: a. b. c. d. Arterial angioma. Venous angioma. Telangiactasis AVM.

Cerebrovascular Diseases Arterio-Venous Malformation Incidence: It occurs in younger age groups (10 -20, maximum 30 years).

Cerebrovascular Diseases Arterio-Venous Malformation Clinical picture: 1. Epilepsy: first cause of epilepsy in childhood following idiopathic type is AVM, then low grade tumors (slowly growing). It is either focal "Jacksonian" or generalized. 2. Bleeding: whether subarachnoid, intracerebral, or intraventricular hemorrhage.

Cerebrovascular Diseases Arterio-Venous Malformation Clinical picture: 3. Weakness: gradual, progressive, and of one limb. Or dementia due to steel phenomena (all the circulating blood go to the AVM and the rest of the vessels are deprived from blood, hemiparesis or dementia occurs especially if near the frontal lobe).

Cerebrovascular Diseases Arterio-Venous Malformation Clinical picture: 4. Migraine may be present. 5. Signs: To and Fro murmur or bruit over the carotid or on the skull at the site of the AVM. It is diagnostic for carotid venous fistula and AVM.

Cerebrovascular Diseases Arterio-Venous Malformation Investigations: 1. Plain X ray skull: shows patch calcification (but it has no role in aneurysm). 2. CT scan: shows area of bleeding triangular in shape. CT scan with contrast shows a special pattern of vessels of AVM (differ from bleeding). 3. Arteriography: a. Retrograde femoral. b. MRA.

Cerebrovascular Diseases Arterio-Venous Malformation Treatment: 1. Microsurgical treatment: Complete excision. 2. Endovascular surgery: Selective embolization of the feeder vessels, so the AVM will shrink. 3. Stereotactic radiosurgery: using the gamma knife or Linac. Very effective for inoperable cases as that of brain stem and basal ganglion.
 3106023")
Data show design & preparation by : Dr. El-Sayed Amr - (012) 3106023

 D. D. of T. I.")
Cerebrovascular Diseases Stroke T. I. A. (Transient Ischemic Attacks) D. D. of T. I. As: 1. Focal epilepsy. 2. Syncope. 3. Hypoglycemia. 4. Vestibular diseases. 5. Migraine.

INTERNAL CAROTID ARTERY segments of ICA branches of ICA

ROLE OF CT BRAIN IN ISCHEMIC STROKE PATIENTS * Exclude simulating conditions or hemorrhagic stroke * Verification of infarction and its anatomical distribution Lt MCA infarction Lt ACA occlusion RT ganglionic infarction
 3106023")
Data show design & preparation by : Dr. El-Sayed Amr - (012) 3106023


Cerebrovascular Diseases Intracerebral Hemorrhage Etiological Classification: A. Capsular: - It occurs due to hypertension and atherosclerosis that leads to rupture of deep perforators on the thalamus, putamen, brain stem, and cerebellum. B. Lobar: - Due to superficial vascular rupture within the cerebral lobes due to AVM or aneurysm embedded in the parenchyma of the brain.

Cerebrovascular Diseases Intracerebral Hemorrhage Clinically: - Sudden coma in 80% of the patients. Signs of sudden rise of ICP. A. Supratentorial heamatoma: - Sudden onset of headache, followed by rapid or gradual loss of consciousness. - Focal signs: - hemiparesis. hemisensory affection. 3 rd nerve palsy with transient tentorial herniation.

Cerebrovascular Diseases Intracerebral Hemorrhage Clinically: B. Infratentorial hematoma: 1. Cerebellar: - Onset of headache. Cerebellar signs. Hydrocephalus due to obstruction of the CSF circulation. 2. Pontine: - Sudden loss of consciousness. Quadriplegia. Pinpoint pupil. Hyperthermia.

Cerebrovascular Diseases Intracerebral Hemorrhage Investigations: 1. 2. CT scan and MRI, to determine the site of the hematoma, its mass effect, and the extent. Angiography reveals AVM, or aneurysm.

Cerebrovascular Diseases Intracerebral Hemorrhage Management: II. Hemorrhagic strokes due to: - Either cerebral aneurysm or AVM.



n n Akher haga khales lebanon
- Slides: 79