Sex sexuality and paraphilias Ahmed Elshafei MD MPHc


 Endocrine organs for")



















 • One in 5 teenagers will have a STD: rates")
 • Syphilis (primary and secondary): – Cases have doubled since")









: • 10 to")
 treatment: • Assessment:")











 • Gender Role: Based on external behavioral patterns (Our society has")









 •")





- Slides: 65
Sex, sexuality, and paraphilias Ahmed Elshafei, MD, MPHc HEA 125
Physiology of SEX and SEXUALITY
Important structures include : Brain: Cerebral Cortex, Limbic system (including amygdala) Endocrine organs for hormones: pituitary, ovaries, testes, adrenal cortex Sensory receptors for touch, fine touch, proprioception, Eyes, Ears External genitalia (penis and scrotum, labia majora, minora and vagina) Internal genitalia (uterus, vas deferens, seminal vessicles, bulbourethral glands) Erectile tissue (corpus cavernosus, corpus spongiosus) Muscles of Orgasm: ischiocavernosus, bulbospangiosus muscles) Secondary sex characteristics (breasts, facial hair, body shape) Autonomic Nervous System (Symathetic for orgasm, parasympathetic for sexual arousal) Not for the exam Leonardo Da Vinci Studies on Mating Behaviors sketch 1493
Not for the exam
Not for the exam Fig. 28 -11, p. 1043
Desire for sex is mediated by the cerebral cortex, limbic system, pheromones, visualization. Sexual arousal is mediated by the ANS Desire vs Arousal
• Desire is the presence of erotic impulses , in thought, feeling or fantasy • Erotic impulses varying widely in recognition and in frequency of occurrence depending on individuals, circumstances and inhibition levels • Erotic impulses are distinct from the impulse to act on erotic thoughts or fantasies. Sexual Desire • Desire is vulnerable to emotional intrusion , most commonly via conflict (overt or covert ) generating anger or resentment between individuals. Anger is especially devastating to desire in men. (Goleman, 1988) • Desire is vulnerable to depression because of its effects on dopamine levels.
Sexual Arousal Testosterone has no effects on arousal. Sexual arousal is mediated by the Autonomic Nervous System (ANS) There are 2 branches of the ANS : The SYMPATHETIC branch and the PARASYMPATHETIC branch. They have separate nerves, neurons, neurotransmitters and pathways and are not interchangeable Parasympathetic (Feed and Breed) pathway is involved in erections in both men and women, lubricating secretions of the bulbourethral glands in men and women, and subjective perceptions of sexual arousal
Testosterone : a hormone , of the steroid type called an androgen Libido or desire is determined by levels of testosterone in both men and women. Testosterone is made in both men and women by the cortex of the adrenal gland in small amounts. Testosterone is made before birth in the XY fetus, and levels are high from the 7 th week to the sixth month and determines the “sex” of the fetus. Levels are low at birth. Testosterone is made by made men in the testes in response to Leutinizing Hormone (LH) from the anterior pituitary gland in larger amounts after puberty and is responsible also for Spermatogenesis Secondary sex characteristics: facial hair, increased muscle mass and fat distribution, muscle growth, metabolic activity Seminal vesicle functions (semen production)
Sex by Design: the role of the Brain in sex Not for the exam • Parasympathetic sexual arousal • Brain- serotonin? Dopamine? • Sympathetic orgasm and ejaculation • Brain-dopamine? Endorphins?
Not for the exam Skin can receive information for deep pressure, touch, light touch, pain/temperature as erotic. Skin covering the glans of the penis and clioris contains many more nocioreceptors and Meissner’s corpuscles than other skin Skin of the labia majora, minora, scrotum, shaft of the clitoris and penis, and inner thigh, all have increased density of Meissner’s corpuscles and Paccinian corpuscles, with small overlapping fields Sensory Information
Oxytocin: A hormone produced by the hypothalamus of the brain, released by the posterior pituitary Dopamine: A neurotransmitter important in orgasms, sensitization to orgasms, and increased sexual desire
v Adolescent Sexual Behavior • Nearly 70% of all unmarried females are non virgins by age 19 (80% of males): – Nearly 4 in 10 teenage girls whose first intercourse experience happened at age 13 -14 report that the sex was unwanted or involuntary – Average of first sexual experience: 16 Not for the exam
Adolescent Sexual Behavior • Adolescents in the aggregate still drift into sexual activity rather than decide to have sex: – Most adolescent sexual activity still takes place in the context of one primary relationship – Most adolescents are not promiscuous, but “serially monogamous”
Adolescent Sexual Behavior • Recent survey - 57% of adolescents claim to have used a condom the last time they had sex: – Other research suggests that they do not do as they say – More than 50% of sexually active adolescents do not use birth control regularly
Teenage Pregnancy • The CDC reports that 305, 388 babies were born to females age 15 -19 in 2012 • This reflects a decrease for US teens in this age group • Teens seem to be less sexually active, and more of those who are sexually active seem to be using birth control than in previous years
Teenage Pregnancy • Despite declines in rates of teen pregnancy in the US, about 820, 000 teens become pregnant each year • Nearly 80% of teenagers who become pregnant are unmarried • 80% of teenage pregnancies are unintended
Teenage Pregnancy • The main rise in the teen pregnancy rate is among females younger than 15 • Close to 25 percent of teen mothers have a second child within two years of the first birth
Teenage Pregnancy • About 1 million US teenagers become pregnant each year: – 10% of all teenage females – 50% of all unwed mothers are teenagers • 50% have the child: – 33% have elective abortions – The remainder are spontaneously aborted
Teenage Pregnancy • About 33% of females aged 15 -19 have at least 1 unwanted pregnancy • Single mothers account for 70% of births to females aged 15 -19
Consequences of Teenage Pregnancy • For mother: – Leading cause of school dropout – High risk for obstetric complications
Consequences of Teenage Pregnancy • For child: – Neonatal deaths and prematurity are common – Possible lower level of intellectual functioning – Problems of single-parent family (increased risk of delinquency, suicide)
Sexually Transmitted Diseases (STD) • One in 5 teenagers will have a STD: rates for gonorrhea and chlamydia are higher for adolescents than for any older group • Highest incidence: most common STD is HPV • Highest prevalence: one in 5 Americans has HSV-2 • Chlamydia is the most commonly reported STD in females and Gonorrhea in males
Sexually Transmitted Diseases (STDs) • Syphilis (primary and secondary): – Cases have doubled since 1970 – Rate now more than 20/100, 000 • Gonorrhea: – Number of cases has declined by half since 1975 – Since 1975, increase in resistant strains
v Male Sexual Response Cycle Not for the exam
v Female Sexual Response Cycle Not for the exam
Definitions • Paraphilias are frequent, intense, sexually arousing fantasies or behaviors that involve inanimate objects, children or nonconsenting adults, or suffering or humiliation of oneself or the partner. • Paraphilic disorders are paraphilias that cause distress or cause problems functioning in the person with the paraphilia or that harm or may harm another person. https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC 3769077/
Paraphilic Disorders • Pedophilia: sexual urges toward children. Most common paraphilic disorder • Exhibitionism: recurrent desire to expose genitals to stranger • Voyeurism: sexual pleasure from watching others who are naked, grooming, or having sex. Begins early in childhood
Paraphilic Disorders • Sadism: sexual pleasure derived from others’ pain • Masochism: sexual pleasure derived from being abused or dominated • Fetishism: sexual focus on objects, e. g. , shoes, stockings – Fantasies about/ or actual crossdressing
Paraphilic Disorders • Frotteurism: male rubbing of genitals against fully clothed female to achieve orgasm • Zoophilia: animals preferred in sexual fantasies or practices • Coprophilia: combining sex and defecation
Paraphilic Disorders • Urophilia: combining sex and urination • Necrophilia: preferred sex with cadavers • Hypoxyphilia: altered state of consciousness secondary to hypoxia while experiencing orgasm – Autoerotic asphyxiation, poppers, amyl nitrate, nitric oxide
Sexual Dysfunctions • Sexual Desire Disorders – Male hypoactive sexual desire disorder: • Deficiency or absence of fantasies or desires • Reasons: low testosterone, CNS depressants, common postsurgery, depression, marital discord
Sexual Dysfunctions • Sexual Arousal Disorders – Female sexual interest/arousal disorder: • Unable to achieve adequate vaginal lubrication • May be hormonally related • Antihistamine and anticholinergic medications cause decrease in vaginal lubrication • Maybe psychologically induced
Sexual Dysfunctions • Sexual Arousal Disorders – Male erectile disorder (impotence): • 10 to 20% lifetime prevalence, point prevalence is 3% • 50% of men treated for sexual disorders have this complaint • Incidence 8% young adult, 75% of males older than 80 • 50% more likely in smokers • Be sure to check alcohol usage, diabetes, marital conflict • Must determine if organic versus psychological
Sexual Dysfunctions • Sexual Arousal Disorders – Male erectile disorder (impotence) treatment: • Assessment: postage stamp test, snap gauge (to test physiological versus psychological) • Treatment: sildenafil (Viagra), vardenafil (Levitra), tadalafil (Cialis)
Snap gauge test for impotence
Sexual Dysfunctions • Orgasm Disorders – Female orgasm disorder: • Inability to achieve orgasm • 5% of married females older than 35 have never achieved orgasm • Overall prevalence from all causes: 30% • Treatment: fantasy, vibrators
Sexual Dysfunctions • Orgasm Disorders – Premature ejaculation: • Male ejaculates before or immediately after entering vagina • More common if early sexual experiences were in back seat of car or with prostitute (anxiety about sexual act) • Treatment: stop and go technique, squeeze technique, SSRIs
Sexual Dysfunctions • Genitopelvic Pain/Penetration Disorders: – Psychological in origin – Recurrent and persistent pain before, during, or after intercourse • Only diagnosed in females • Not diagnosed if due to medical problems – Involuntary muscle constriction of the outer third of the vagina that prevents penile insertion(vaginismus) • Treatment: relaxation, Hegar dilators
Sexuality and Aging • Sexual interest does not decline significantly with aging • Continued sexual activity means sexual activity can continue • Best predictor of sexual activity in the elderly is availability of a partner
Sexuality and Aging • Changes in males: – Slower erection – Longer refractory period – More stimulation needed
Sexuality and Aging • Changes in females: – Vaginal dryness – Vaginal thinning – Can be reduced by estrogen replacement
Masturbation • Normal activity from infancy to old age • Reasons: – In adults: lonely, tired, bored, relieve stress, help sleep – In children: normal, feels good • Frequency: 3 -4 times weekly for adolescents, 1 -2 times weekly for adults, once a month for married people
Masturbation • Equally common in males and females • Abnormal only if interferes with sexual or occupational functioning • Can lead to premature ejaculation in males who use it primarily to reduce tension
LGBTQ
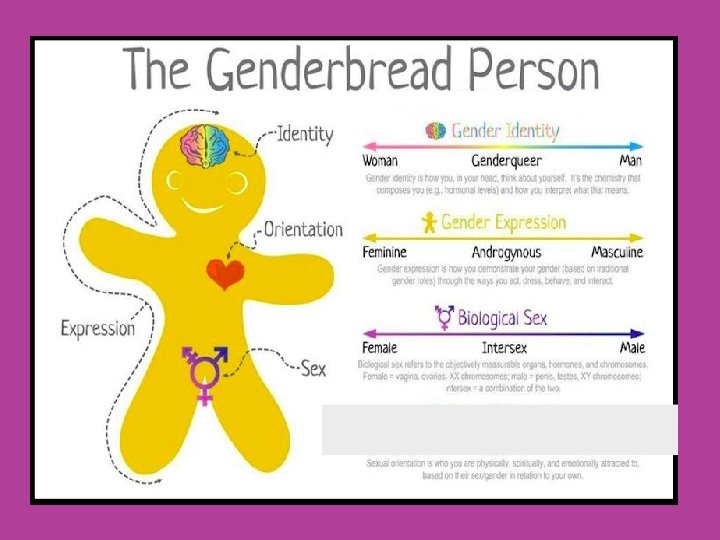
Human Sexuality: Terminology • Sexual Identity: Based on sexual characteristics • External and Internal Genitalia • Hormonal and secondary sexual characteristics • Gender Identity: Based on a person’s sense of feeling (man, woman, both, neither, etc. ) • Established by the age of 3
Human Sexuality: Terminology(cont…) • Gender Role: Based on external behavioral patterns (Our society has a set of ideas about how we expect men and women to dress, behave, and present themselves). https: //www. plannedparenthood. org/learn/sexual-orientation-gender/gender-genderidentity/what-are-gender-roles-and-stereotypes • Sexual Orientation: Based on a person’s choice of a love object • • • Heterosexual Homosexual Bisexual Pansexual Asexual
How does gender roles affect sexuality?
Facts There really is no single LGBTQ community, rather a very diverse population that comes from all racial, ethnic, cultural, socioeconomic, and geographic backgrounds. People who are LGBTQ may move to urban areas, if they can, where there may be a sense of greater acceptance and personal safety.
Facts It is very difficult to know the percentage of people who identify as LGBTQ. Stigma and the fear of biases contribute to an underreporting of actual sexual orientation. Some people may also self-identify one way even if their internal desires or sexual behavior imply a different orientation.
Facts Identify issues may be especially pronounced for LBGTQ people from particular racial and ethnic minority groups. In DSM-V: • Includes a separate, non-mental disorder diagnoses of gender dysphoria to describer people who experience significant distress with the sex and gender they were assigned at birth.
Stigma & risk factors • Stigma, both internal and external, continues to be the greatest problem facing sexual and gender minorities. • Internally, many LGBTQ people develop an internalized homophobia that can contribute to problems with self-acceptance, anxiety, depression, difficulty forming intimate relationships, and being open about what sexual orientation or gender identity one actually has.
Stigma & risk factors Externally, stigma may be exhibited by the surrounding society and even from within the LGBTQ community. For example, some gay and lesbian people have a difficult time accepting bisexuals. Transgender people have been excluded from some gay organizations, and are only recently received more notice and acceptance throughout the country.
Stigma & risk factors • Additionally, most LGBTQ people are not raised by people who identify as LGBTQ. (support & understanding? ? ) • LGBTQ persons struggle with higher rates of anxiety, affective disorder related conditions, and substance use disorders; • Alarmingly, LGBTQ people also have a nearly three time higher risk of suicide or suicidal behavior.
Stigma & risk factors • LGBTQ people also face disparities in the physical medical context, including increased tobacco use, HIV and AIDS, and weight-related problems. • LGBTQ people are also at greater risk for discrimination, verbal abuse, physical assaults and violence, and perhaps even childhood sexual abuse.
Stigma & risk factors • Though legal protections have been increasing dramatically, many places do not protect sexual or gender minorities in the workplace, housing, or access to health care. • Fears of potential discrimination contribute to some LGBTQ people not seeking the help they need—medically or psychiatrically—in a timely manner if at all. • Studies have shown that many are afraid to be open about their sexual orientation or feelings with their mental health providers.
Homosexuality • Not considered a mental illness (it was until 3 decades ago!!) • 4 to 10% of all males, 1 to 3% of all females • Issue is partner preference, not behavior – Behavioral patterns of homosexuals are as varied as those of heterosexuals – Same level and variations in sexuality as for heterosexuals
Homosexuality • Male-male relationships are less stable than female-female relationships • Over 50% of homosexuals have children • Increasing evidence of biologic contribution – Higher concordance rates for MZ twins (52%) than for DZ (22%)
Homosexuality • Distinguish between ego-syntonic and egodystonic homosexuality: – Ego-syntonic: agrees with sense of self, person is comfortable – Ego-dystonic: disagrees with sense of self, makes person uncomfortable – If ego-dystonic: sexual orientation distress. NOT considered pathologic unless ego-dystonic
Homosexuality • Preference well established by adolescence: – Feelings of preference emerge 3 or more years before first encounter – Describe duration of feelings with “As long as I can remember”
Homosexuality • Similar number of heterosexual experiences reported in childhood and adolescence: – Report experiences as “ungratifying” – 30 to 40% of all people report at least 1 same-gender sexual experience
QUESTIONS