Intracranial Tumors Department of Neurosurgery Faculty of Medicine




 Nerve sheath tumors (8%)")
 Oligodendroglioma Oligoastrocytoma")
. Malignant")







")








 -")





 n Evoked potential")

 Surgery: -")
 3106023")






. Majority are located supratentorial though")



: Most common on 8 th nerve and 5")









 usualy present with a triad of hearing loss, disequilibrium")


. 15% of all intracranial")
. Intrasellar: A large")









 3106023")


- Slides: 81
Intracranial Tumors Department of Neurosurgery Faculty of Medicine, Alexandria University
Intracranial tumors Intracranial Tumors Epidemiology: Incidemce: - 8 -10/100, 000 per year - 1 -2% of all cancer deaths - 20% of all paediatric tumors Hereditary Implicated in a few brain tumors such as: • Multiple neurofibromatosis. • Cerebellar hemangiomas. Age: Brain tumors occur at any age.
Intracranial tumors Intracranial Tumors Etiology: 1. 2. 3. 4. 5. 6. Chromosomal abnormalities Environmental carcinogens Viral Immunosupression Electromagnetic radiation Others (trauma, organic solvents)
Intracranial tumors Intracranial Tumors Classification: I. II. Neuroepithelial tumors (52%) Nerve sheath tumors (8%) III. Meningeal tumors IV. Pituitary tumors V. Germ cell tumors VI. Lymphoma VII. Tumor-like malformations VIII. Metastatic tumors IX. Local extension from regional tumors (15%) (8%) (15%)
Intracranial tumors Intracranial Tumors Neuroepithelial tumors: a. Gliomas Astrocytoma (grade 1 -4) Oligodendroglioma Oligoastrocytoma Ependymoma Choroid plexus tumor b. Pineal tumors c. Neuronal tumors Ganglioma Gangliocytoma Neuroblastoma d. PNET (primitive neuroectodermal tumors) Medulloblastoma
Intracranial tumors Intracranial Tumors Nerve sheath tumors: a. b. c. d. Schwanoma (neurinoma). Malignant neurinoma. Neurofibroma. Malignant neurofibroma. Meningeal tumors: a. b. c. Meningioma. Malignant sarcoma. Melanotic ® meningeal melanomatosis Pituitary tumors: a. b. Pituitary adenoma. Pituitary carcinoma.
Intracranial tumors Intracranial Tumors Germ cell tumors: a. b. Germinoma. Teratoma. Tumor like malformations: a. b. c. Craniopharyngioma. Colloid cyst of third ventricle. Dermoid and epidermoid. Local extension form regional tumors: I. II. Glomus jugulare turnours. Chordoma.
Intracranial tumors Intracranial Tumors Incidence of most frequent tumors: Neuroepithelial tumors Astrocytoma Ependymoma Oligodendroglioma Medulloblastoma Meningiomas Metastases Pituitary adenoma Neurinoma 52% 44% 3% 3% 3% 15% 8% 8%
Intracranial tumors Clinical manifestations of brain tumors: 1 - Supratentorial tumors 2 - Infratentorial tumors
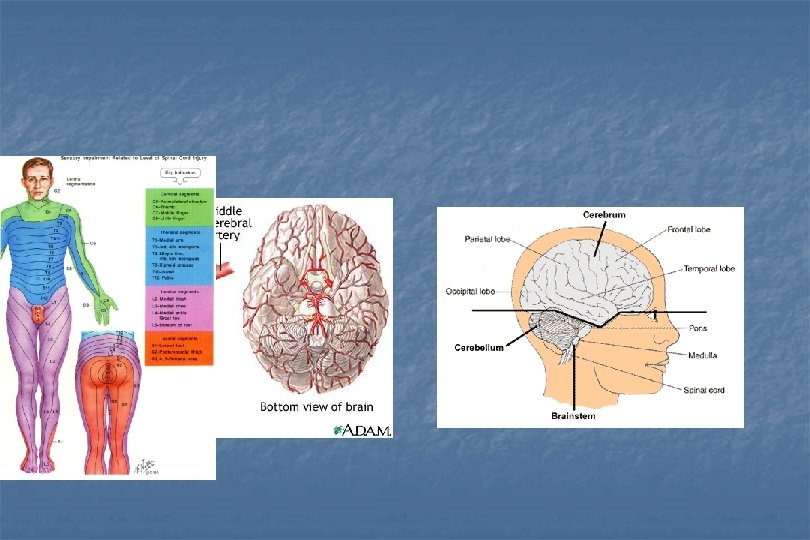
Intracranial tumors Clinical manifestations of brain tumors: 1 - Supratentorial tumors 1 -Manifestations of increased ICP - headache, vomiting, blurring of vision - drowsiness - ataxia, vertigo - diplopia 2 - Focal neurological deficit depends upon the site of the tumor: - frontal - temporal - parietal - occipital 3 - Epilepsy 4 - Special presentation for pituitary tumors
Focal neurological deficit
Intracranial Tumors Focal neurological deficit 1 - Frontal tumor - contralateral hemiparesis - expressive dysphasia (dominant hemisphere) - faecal and urinary incontinence - personality changes and dementia
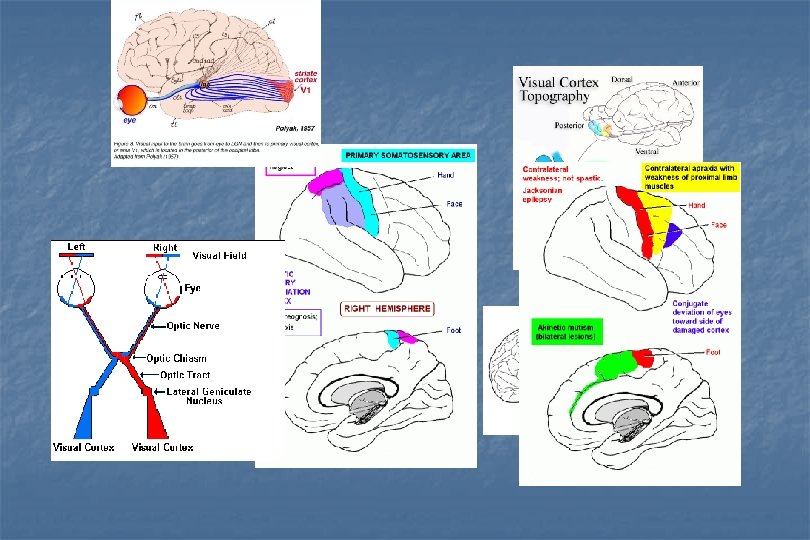
Intracranial Tumors Focal neurological deficit 2 - Parietal tumor - contralateral sensory impairment - homonymous hemianopia - Gerstmann's s syndrome (dominant hemisphere) - apraxia (non dominant hemisphere)
Intracranial Tumors Focal neurological deficit 3 - Temporal tumor - receptive dysphasia (dominant hemisphere) - homonymous hemianopia - auditory problems - olfaction, behaviour and memory affection
Intracranial Tumors Focal neurological deficit 4 - Occipital tumor - homonymous hemianopia
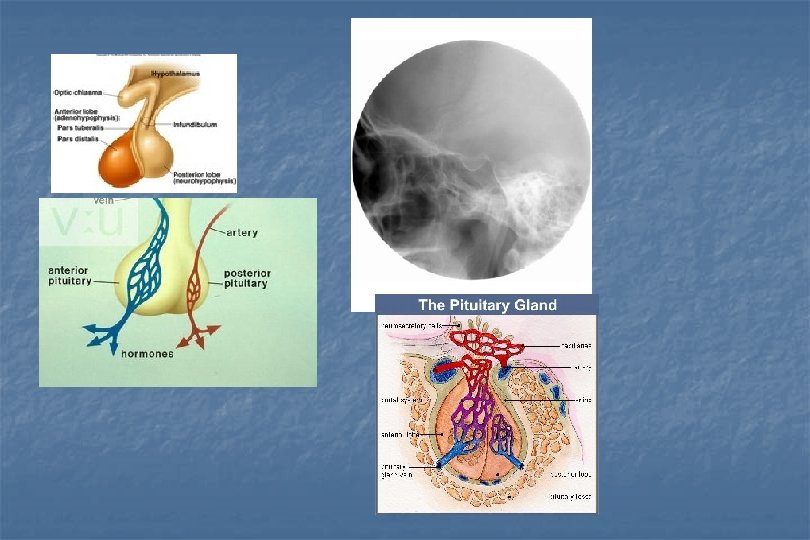
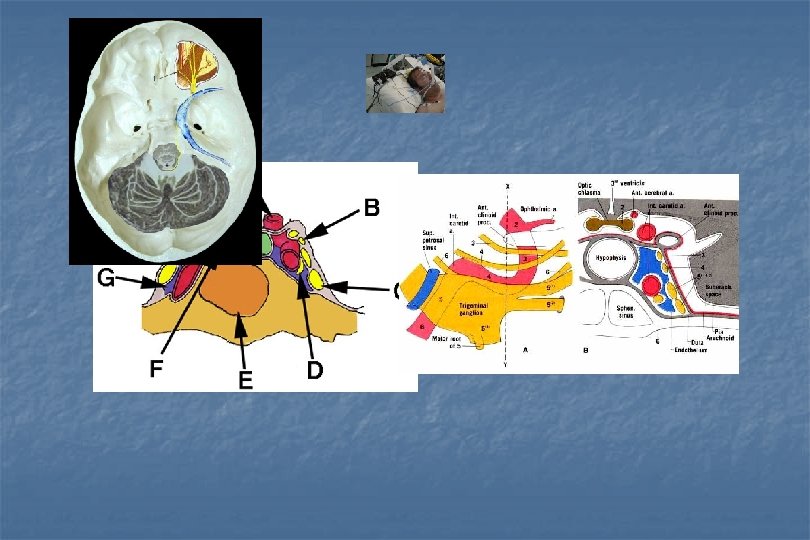
Intracranial tumors Clinical manifestations of Pituitary tumors: 1 - Endocrinologic disturbances - hyperfunction - hypofunction 2 - Mass effect - Superior: - optic chiasm (bitemporal hemianopia) - third ventricle (hydrocephalus) - pituitary gland (hypopituitarism) - hypothalamus - anterior cranial fossa - Lateral: - cavernous sinus (CN affection III, IV, VI, V 1) - temporal lobe (temporal lobe dysfunction) - Inferior: - nasopharyngeal mass - CSF rhinorrhea 3 - Pituitary apoplexy 4 - CSF rhinorrhea
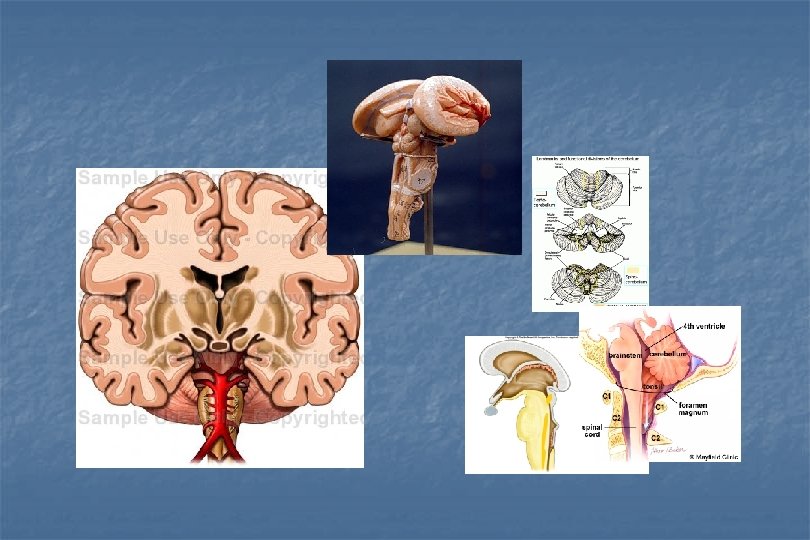
Intracranial tumors Clinical manifestations of brain tumors: 2 - Infratentorial tumors 1 -Manifestations of increased ICP (obstruction of the 4 th ventricle) 2 - Focal neurological deficit
Intracranial tumors 2 - Focal neurological deficit: - Cerebellar hemisphere: limb ataxia, dysmetria, intentional tremors - Cerebellar vermis: truncal ataxia, broad based gait, titubation - Brain stem: lower cranial nerve affection, motor and sensory tracts affection, nystagmus - Neck stiffness and head tilt
Intracranial tumors Pituitary Tumors Pituitary adenoma Arising from anterior pituitary gland. Usually they are benign. Microadenoma (less than 1. cm). Macroadenoma (more than 1 cm).
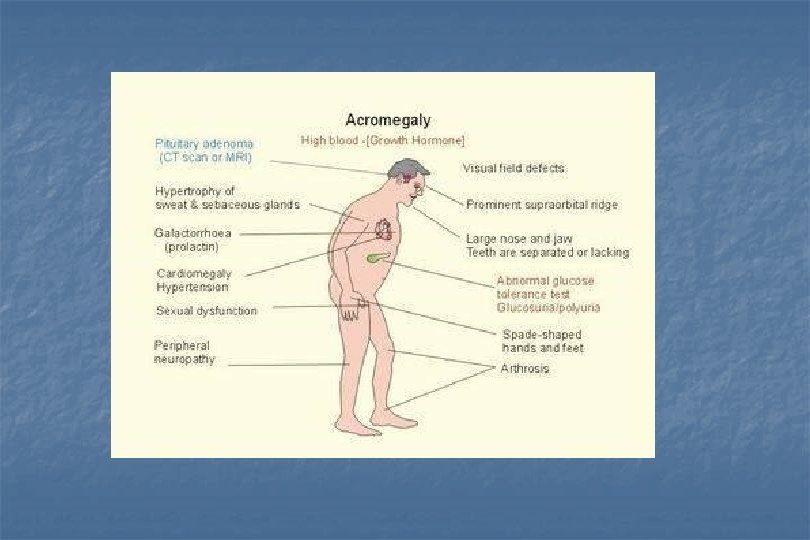
Intracranial tumors Pituitary Tumours Classification of pituitary adenomas: I. Secreting adenomas: (present with endocrinological manifestations) - Somatotropin (growth hormone) secreting adenoma: Acromegaly, gigantism). - Prolactin secreting adenoma (prolactinoma): Amenorrhea galactorrhea syndrome - ACTH secreting adenoma: Cushing's disease. - Thyrotropin (TSH)) secreting adenoma: Gonadotropin( FSH, LH) secreting adenoma: II. Non secreting pituitary adenoma: (present with mass effect) - Hypopituitarism
Intracranial tumors Clinical manifestations of Pituitary tumors: 1 - Endocrinologic disturbances - hyperfunction - hypofunction 2 - Mass effect - Superior: - optic chiasm (bitemporal hemianopia) - third ventricle (hydrocephalus) - pituitary gland (hypopituitarism) - hypothalamus - anterior cranial fossa - Lateral: - cavernous sinus (CN affection III, IV, VI, V 1) - temporal lobe (temporal lobe dysfunction) - Inferior: - nasopharyngeal mass - CSF rhinorrhea 3 - Pituitary apoplexy 4 - CSF rhinorrhea
Intracranial tumors Clinical manifestations of Pituitary tumors: 1 - Endocrinologic disturbances - hyperfunction - hypofunction
Intracranial tumors 2 - Mass effect - Superior: - optic chiasm (bitemporal hemianopia) - third ventricle (hydrocephalus) - pituitary gland (hypopituitarism) - hypothalamus - anterior cranial fossa - Inferior: - nasopharyngeal mass - CSF rhinorrhea
Intracranial tumors 2 - Mass effect - Lateral: - cavernous sinus (CN affection III, IV, VI, V 1) - temporal lobe (temporal lobe dysfunction)
Intracranial tumors Pituitary apoplexy
Investigations of Brain Tumors Laboratory investigations Visual assessment and audiometry Hormonal assay Plain X-ray CT scan and CTA MRI, MRA and MR spectroscopy: Cerebral angiography SPECT and PET scan Evoked potential
Investigations of Brain Tumors Plain X-ray CT scan and CTA
Investigations of Brain Tumors MRI, MRA and MR spectroscopy: show site, size, edema, ventricular enlargement, and displacement. SPECT and PET scan
Investigations of Brain Tumors n Cerebral angiography shows tumor vasculature (meningiom) n Evoked potential
Intracranial tumors Treatment of brain tumors 1. Conservative treatment: - measures to decrease the ICP - antiepileptic treatment - hormonal therapy 2. Biopsy: - open - stereotactic 3. Surgery 4. Radiotherapy: - Conventional radiotherapy - Stereotactic radiosurgery 5. Chemotherapy
Intracranial tumors Pituitary Tumors Treatment: 1. Conservative treatment: - 2. Bromocriptine (prolactinoma) Surgery: - In large tumors and if medical treatment fails. a. Transsphenoidal approach: - Sublabial - Transnasal b. Transcranial approach: 3. Radiotherapy: - If failed medical and surgical treatment a. Conventional radiotherapy b. Stereotactic radiosurgery
Data show design & preparation by : Dr. El-Sayed Amr - (012) 3106023
Intracranial tumors Intracranial Tumors Astrocytoma: Most frequent brain tumors. All grades of anaplasia may occur. Cysts filled with clear yellow fluid. In the cerebellum, these tumors are benign, total resection with cure is possible.
Intracranial tumors Intracranial Tumors Oligodendroglioma: Occur in middle age, localized mainly in the brain's hemisphere. Calcification is common. Epilepsy is the most common symptoms.
Intracranial tumors Intracranial Tumors Ependymoma: It is common in childhood. Occur in the lateral ventricle. Calcification may occur.
Intracranial tumors Intracranial Tumors Choroid plexus papilloma: Benign tumor of childhood. Reddish in color. Provokes hydrocephalus.
Intracranial tumors Intracranial Tumors Glioblastomas: Occurs most frequently in age 40 60 years. In frontal and temporal lobes. Extends through corpus callosum. Areas of necrosis hemorrhage and cysts are common.
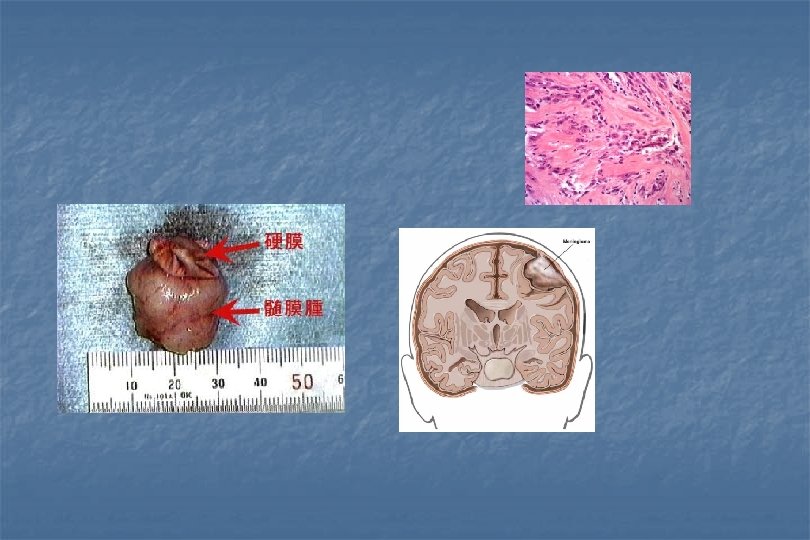
Intracranial tumors Intracranial Tumors Meningiomas: Females> males (2: 1). Majority are located supratentorial though 10% are located infratentorial. Bony reaction (hyperostosis) occurs in adjacent bone.
Intracranial tumors Intracranial Tumors Meningiomas: Foramen magnum meningioma Jugular foramen meningioma
Intracranial tumors Intracranial Tumors Metastatic tumors: 20 -30% of all brain tumors. Carcinoma of, the bronchus is the most common then comes breast and GIT. Solitary or multiple.
Intracranial tumors Intracranial Tumors Medulloblastoma: The commonest tumor in childhood. Incidence 4 -6 years. Arises from vermis. May obstruct the fourth ventricle and cause obstructive hydrocephalus. Seedling occurs in subarachnoid space.
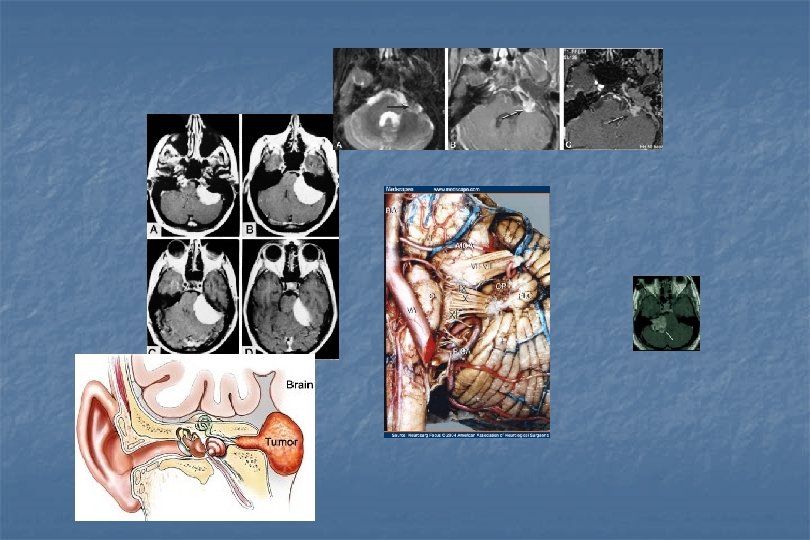
Intracranial tumors Intracranial Tumors Neurinoma (Schwannoma): Most common on 8 th nerve and 5 th nerve. Families with neurofibroma tend to develop bilateral acoustic neurinoma.
Intracranial tumors Treatment of brain hemispheric tumors Surgery is the basic method for treatment. Most meningioma are non invasive and total excision is possible. The use of microsurgical techniques, ultrasound aspiration helps greatly in surgery. Meningiomas in the cavernous sinus and clivus can not be totally removed.
Intracranial tumors Treatment of brain hemispheric tumors Surgical technique: Craniotomy flap with good access to the tumor. Protection of neighboring brain. The tumor removed using microsurgical technique. Invaded dura should excise, and graft is used (in cases of meningioma).
Intracranial tumors Treatment of brain hemispheric tumors Surgical technique: Surgery for glioma is less satisfactory if compared to meningioma, gliomas spread within the hemisphere thus total excision is therefore impossible. Partial removal is usually achieved to decrease intracranial pressure. Surgery for metastases is palliative solitary metastatic lesions can be removed.
Intracranial tumors Tumors of the lateral ventricle These tumors are arising most frequently form choroid plexus or ependymoma. Meningiomas and papillomas are usually pediculated tumors projecting into the ventricular cavity. Rarely epidermoids, dermoids or teratomas may be found.
Intracranial tumors Tumors of the lateral ventricle These tumors are already large when the diagnosis is made because they grow slowly within the ventricular cavity. Signs and symptoms are usually secondary to a mass effect or ventriculomegaly. Complete removal of meningiomas and papilloma of the lateral ventricle is possible despite their large size because they are well limited from the ventricular wall.
Intracranial tumors Tumors of the lateral ventricle Ependymomas have wide bases which infiltrate the brain hemisphere, they commonly be partly removed. So, surgical therapy is complemented by radiotherapy and chemotherapy.
Intracranial tumors Tumors of the third ventricle Anterior third ventricle: Craniopharyngioma and colloid cyst and ependymal cyst and choroid plexus papilloma. Growths obstruct the foraminae ot'Monro ® producing obstructive hydrocephalus. Posterior third ventricles: Arising from pineal gland, 10% of these tumors are benign including lipomas, cyst, pineocytomas, and meningiomas. Another group is relatively benign (10%); low grade astrocytoma and dermoid cysts.
Intracranial tumors Tumors of the third ventricle Posterior third ventricles: Pineal tumors occlude the aqueduct of sylivus causing obstructive hydrocephalus. Characteristically "Paranoid syndrome" consisting of upward gaze paralysis. Total excision is possible for meningioma, papilloma, colloid cyst. Hydrocephalus is treated by a shunt operation. Radiation therapy for malignant tumors.
Intracranial tumors Posterior fossa tumors Metastases in patients above 50 years. Brain stem tumors. Cerebellopontine angle tumors e. g. acoustic neuroma. In children; medulloblastoma and astrocytoma are the most common tumors. Medulloblastoma arises from the vermis, it grows quickly, invading the fourth ventricle, it disseminate via CSF into spinal canal. Cerebellar astrocytoma in a child is benign and frequently contains a large cyst with fluid high in protein contents.
CP angle tumors (acoustic neurinomas) usualy present with a triad of hearing loss, disequilibrium and tinnitus.
Intracranial tumors Posterior fossa tumors Treatment Surgical removal followed in some cases by additional radiotherapy and chemotherapy. The control of hydrocephalus by ventriculo peritoneal shunt. Tumors (astrocytomas, medulloblastoma, ependymomas) should be removed as total as possible (except those invading the brain stem). Then radiotherapy instituted including the spinal cord in cases of medulloblastomas. CP angle tumors can be removed totally.
Intracranial tumors Tumours of Sellar & Parassellar Regions Those include: Pituitary adenomas. Craniopharyngiomas. Supra and parasellar meningiomas. Gliomas of optic nerve.
Intracranial tumors Craniopharyngioma Arise from squamous epithelial remnants (Rathke's pouch). 15% of all intracranial tumors in children and 5% of adults. Usually the largest part of the tumor is cystic with a small part being solid.
Intracranial tumors Craniopharyngioma Sites: Suprasellar (prechiasmatic and subchiasmatic of third ventricle). Intrasellar: A large tumor extends retrosellar, subfrontal, subtemporal and posterior fossa.
Intracranial tumors Craniopharyngioma Clinically: Increased ICP. Visual disturbances. Endocrinal manifestations: - Hypogonadism. Diabetes insipidus.
Intracranial tumors Craniopharyngioma Treatment: Radical surgical excision is possible in some cases using transcranial approaches. When removal is incomplete, radiotherapy is advisable.
Intracranial tumors Supra and para sellar meningiomas Arises from tuberculum sellae and diaphragm sellae. Compress the optic nerves and chiasma. On examination: - Diminished visual acuity in one eye. - Field defect.
Intracranial tumors Supra and para sellar meningiomas CT: densely enhancing round mass in the midline and extending anteriorly. Meningiomas of the anterior clinoid, medial sphenoid using involves the internal carotid artery, compress and surround the optic nerve and may be the cavernous sinus is involved by the tumor.
Intracranial tumors Supra and para sellar meningiomas Treatment: Suprasellar and parasellar tumors may be totally removed except for the part involving the cavernous sinus and internal carotid artery.
Intracranial tumors Tumors of the orbit The most common are: - Optic nerve glioma. - Optic nerve meningioma.
Intracranial tumors Tumors of the orbit Clinical picture: 1. Exophthalmia is a common feature: - Painless in benign tumors. Painful in malignant tumors. 2. The globe may be displaced according to the site of the tumor. 3. Eye movements limited by mechanical factors or affection of III, IV, & VI cranial nerves in orbital fissure. 4. Visual acuity is affected. 5. Pulsations indicate vascular lesion.
Intracranial tumors Tumors of the orbit Investigations: 1. X ray orbit: Extension and erosion of malignant tumors. - Dilatation of optic foramen. Local osteosclerosis (in meningiomas). 2. CT and MRI.
Intracranial tumors Tumors of the orbit Treatment: Orbital tumors need surgical excision. Surgical approach: 1. Anterior orbitotmy. 2. Lateral orbitotmy. 3. Frontal transcranial approach. Malignant tumors ® partial excision and radiotherapy.
Data show design & preparation by : Dr. El-Sayed Amr - (012) 3106023
Akher haga khales lebanon