Brain Tumors Ainshams University Neurosurgery department Classification Brain

Brain Tumors Ainshams University Neurosurgery department

Classification Brain tumors Supratenrorial Primary Intraxial Secondary Extraxial Infratentorial

 Tymours of neuroepithelial tissues: 1)")
WHO classification • WHO Classification of CNS Tumors A) Tymours of neuroepithelial tissues: 1) Astrocytoma G 1 Pilocytic G 2 Fibrillary gemistocytic protoplasmic mixed G 3 Anaplastic G 4 Glioblastoma multiform ( the most malignant Astrocytoma)

 Tumors of neuroepithelial tissue: (Cont. ) 2) oligodendroglioma 3) ependymomas 4)")
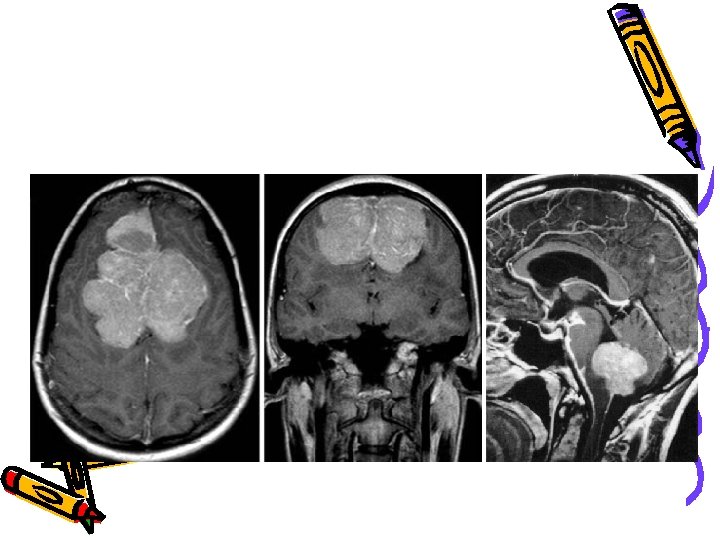
WHO classification A) Tumors of neuroepithelial tissue: (Cont. ) 2) oligodendroglioma 3) ependymomas 4) Choriod plexus: Papilloma Carcinoma 5) Embyronal tumors: primitive neuroectodermal tumors PNET may be either cerebellar ( supratentoral) or Medulloblastoma (infratentoral)
 Tumors of meninges: 1) Tumors of meningiothelial cells: *Benign meningioma: Meningothelial")
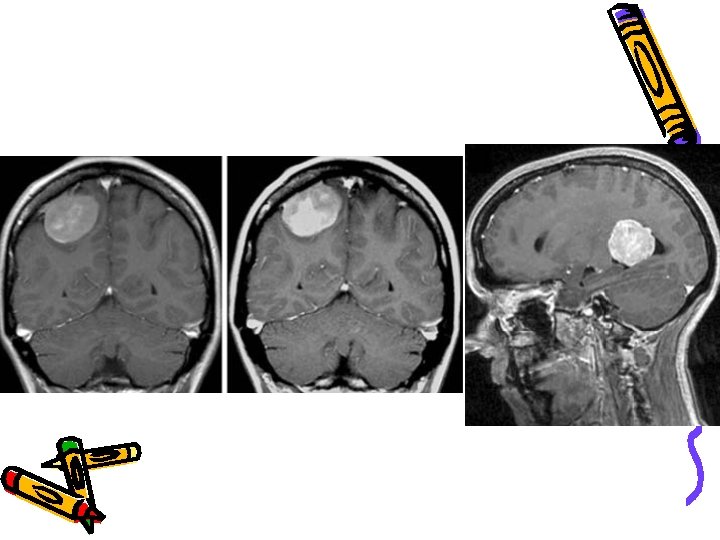
WHO classification B) Tumors of meninges: 1) Tumors of meningiothelial cells: *Benign meningioma: Meningothelial Fibroblastic Transitional Psammomatous *Atypical meningoma *Anaplastic (malignant) meningioma Site Olfactory groove meningioma Sphenoid ridge meningioma Parasaggital meningioma
 Tumours of meninges : (cont. ) 2)Mesencymal( nonmeningothelial) *Benign e. g")
WHO classification B) Tumours of meninges : (cont. ) 2)Mesencymal( nonmeningothelial) *Benign e. g Lipoma *Malignant e. g hemangiopericytoma *Primary melanocytic lesions either diffuse melanosis or malignant melanoma
 Tumors of cranial nerves: *schwanoma (neuroma) e. g Acoustic neuroma *Neurofibroma")
WHO classification C) Tumors of cranial nerves: *schwanoma (neuroma) e. g Acoustic neuroma *Neurofibroma D) Lyphoma: Primary or secondary malignant lyphoma E)Germ cell tumors: *Teratoma: Immature or Mature or Teratroma with malignat transformation
 Cysts or tumor like lesions: *Rathke’s cleft cyst *Epidermoid cyst *Dermoid")
WHO classification F) Cysts or tumor like lesions: *Rathke’s cleft cyst *Epidermoid cyst *Dermoid cyst *Colloid cyst G) Tumors of sellar regoins *Pitutary adenoma *Pitutary carcinoma *Crainopharyngiomas either Adamantious or Papillary H) Local extension from regional tumors *paraganglioma *choedoma *Chordosarcoma
 Metastasis: Brain metastasis is the most common brain tumor seen clinically")
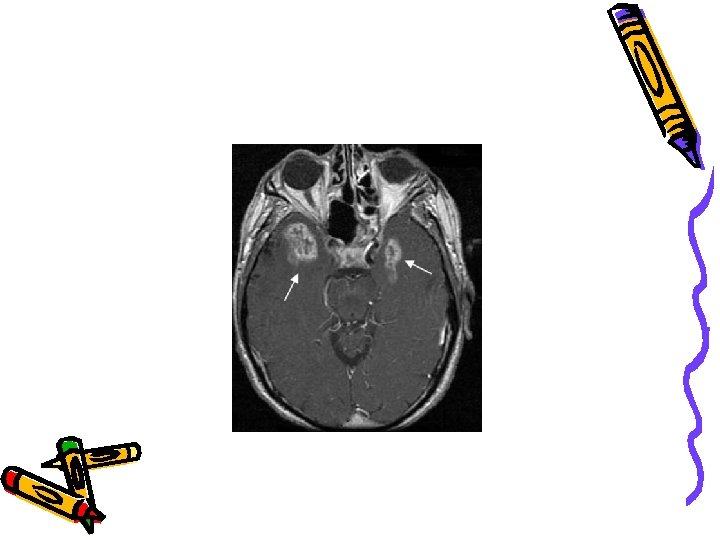
WHO classification I) Metastasis: Brain metastasis is the most common brain tumor seen clinically (more than 50%) It is either *Solitary mass, where surgical resection is possible *Multiple metastasis N. B. most of primary brain tumor does not tend to send systemic metastasis, but metastasis through csf spread is more common

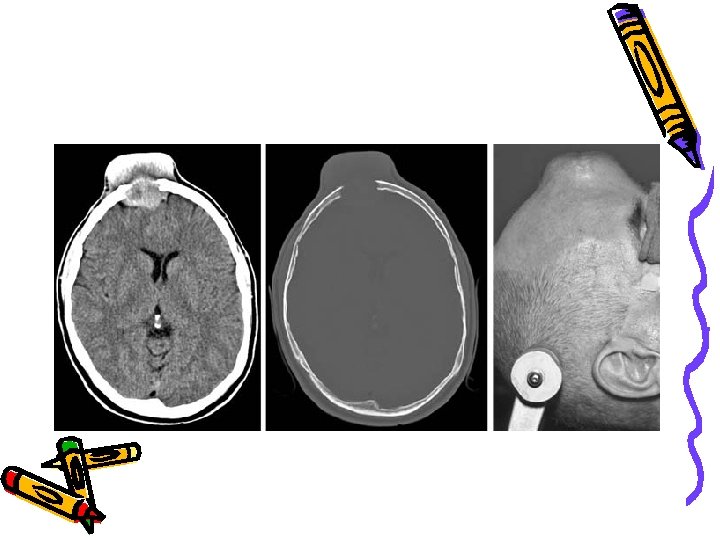
WHO classification Skull tumors Benign *Osteoma *Hemangioma *Dermoid and Epidermoid *Chondroma *Anuerysmal bone cyst Malignant *Metastatic: Prostatic Thyroid Breast Lung *Chondrosarcoma *Fibrosarcoma
")
Clinical presentation • • • Progressive neurological deficit (most common presentation 68 % ) Convulsion ( 26% ) Headache ( 54 % ) Etiology of tumor headache: A) Increasded intracranial pressure: *Tumor mass itself *hydrocephalus *Associated oedema *Associated hemorrhage B) Invasion or compression of pain sensitive structures: *Dura *Blood vessel *Periosteum C) secondary to difficulty in vision D) Extrem hypertension from increased ICP ( cushing’s traid) E) Psycogenic from stress from loss of functional capacity

Clinical presentation Supra tentorial • Increased intracranial tension *Headache *Nausea, vomiting either due to increased ICP or direct pressure to vagal nucleus or the area postrema( vomiting center) *Papilloedema *Gait disturbance *Diplopia, due to 6 th nerve palsy as it have long intracranial course, it is a false localization sign
 • Focal deficit, include weakness or dysphasia • Convulsions,")
Clinical presentation Supratentorial (cont. ) • Focal deficit, include weakness or dysphasia • Convulsions, tumors should be suspected in an idiopathic first time seizure in a patient> 20 years • Mental status changes, depression or confusion or lethargy • In cases of pituitary tumors *Visual affection *Symptoms due to endocrinal disturbance *Pituitary apoplexy

Clinical presentation Infratentorial • Signs and syptoms of increase intracranial pressure • Signs and syptoms of mass effect A) Lesions in cerebellar hemispheres Ataxia of extremities, dysmetria B) Lesion in cerebellar vermis Truncal ataxia, broad based gait C) Brain stem involvement Multiple cranial nerve affection, long tract abnormalities, nystagmus


Investigations of brain tumors • General: • Full labs, CBC, PTT, Blood chemistry • Chest X_Ray • ECG if more than 30 years • Special – Radiological • • C. T. Scan with and without contrast MRI (magnetic resonance imaging) Cerebral angiography if suspecting vascular SOL Skull X_Ray: show enlarged sella turcica or calcified pineal gland or calcification in meningioma • Bone scan
 – Endocrinal: pituitery hormone survey (Growth")
Investigations of brain tumors • Special (Cont. ) – Endocrinal: pituitery hormone survey (Growth hormone, Prolactine, TSH, ACTH, FSH, LH) – Visual: • Fundus examination • Visual field • visual evoked potential


Treatment of Brain tumors • Conservative: • Medical – Only applied for small benign tumors with no sign or symptoms – Should be with closed follow up clinically and radiologically – Treatment to decrease associated oedema • • Mannitol 20% 1 gm/kg/day Lasix 0. 1 mg/kg Decadrone (steroids) 0. 5 -1 mg/kg Glycerine oral – Antiepeleptics • Epanutin (available in I. V. form) – Loading dose 15 mg/kg/dose – Maintance dose 7. 5 mg/kg on 3 divided doses • Depakine • Tegretol
 – Supportive measures • Zantac and")
Treatment of Brain tumors • Medical (Cont. ) – Supportive measures • Zantac and proton pumb inhibitors to avoid stress ulcer • Fluids • Analgesic pre and postoperative – Endocrinal treatment: either replacement therapy if hypopituitarism or suppressant therapy if over functioning adenoma

Treatment of Brain tumors • Surgical treatment – Steriotactic brain tumor, it is either CT or MRI guided • Indications – – – Tumors in elouquent or inaccessible area of the brain Small timors with minimal deficit Patient with general condition precluding general anathesia To ascertian diagnosis when it is not definatly established Catheter placement either for drainage or injecting radioactive material – Steriotactic crainotomy
 – Surgical resection • Attempt")
Treatment of Brain tumors • Surgical treatment (cont. ) – Surgical resection • Attempt for radical resection is more with benign tumors, surfacing, in non eloquent area • Where debulking of tumor is more with malignant tumors with illdefined edges or near eloguent area – Radiosurgery • Use steriotactic localization to focus large dose of radiation onto a lesion – CSF diverting procedure: V_P Shunt

Treatment of Brain tumors • Chemotherapy or radiotherapy – Most of chemotherapy agent does not cross blood brain barrier so limis use of systemic chemotherapy and instead the use of intrathecal chemotherapy is used – Conventional radiotherapy is limited in children to avoid growth retardation
- Slides: 30