BRAIN TUMORS Epidemiology 82100000 20 of malignancies of15

BRAIN TUMORS: Epidemiology: 82/100000 20% of malignancies of<15 years Incidence peak in childhood increase from 20 to 70 years decease>70 Glioma M>F Meningioma F>M

In childhood: Medulloblastoma& Astrocytoma In adults: Glioma&Meningioma In childhhod: 70% infratentorial In adult: 70% supratentorial Survival in children is better

Risk factors: stroke, menopose, breast cancer, farmacotics EBV CNS lymphoma JCV PML Astrocytoma Radiation Antioxidants----preventive

Clinical Diagnosis: Mass effect-Edema-IICP Negative &Positive Signs Headache Vomiting Facial pain
-focal Changes of conciousness(frontal) Frontal SOL: silent-personalitydisorder Abulia-Judjment dis-incontinency. Primitive reflexes Occiputal SOL:")
Seizure(30 -70%)-focal Changes of conciousness(frontal) Frontal SOL: silent-personalitydisorder Abulia-Judjment dis-incontinency. Primitive reflexes Occiputal SOL: Visual field changes

Temporal SOL: Seizure-Aphasia. Visual field disturbance Parietal SOL: Cortical sensoryloss Neglect-Anosognosis. Hemiparesis-Visuospatial D Thalamic SOL: Hemisensoryloss

Brain stem SOL: Cranial nerve palsy Hicough-Vomiting-Hemiparesis Pineal SOL: Parinaud syn. -Premature Puberty-Hydrocephalus Cerebellar SOL; Headache-Vomiting Neck stiffness-Ataxia

Acoustic neuroma; Deafness-Facial weakness-vertigo Pituitary adenoma: Bitemporal hemianopia Neuroophthalmologic signs: Parinaud syn. -Ptosis-papiledema. Optic atrophy-Foster kennedy syn.

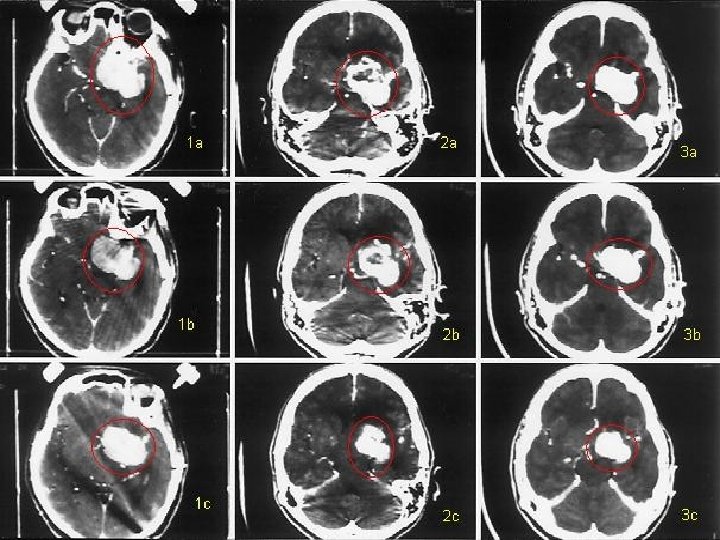
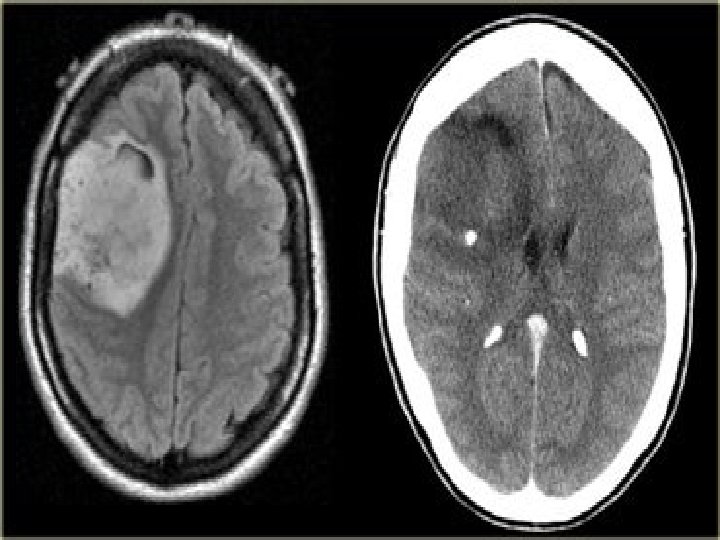
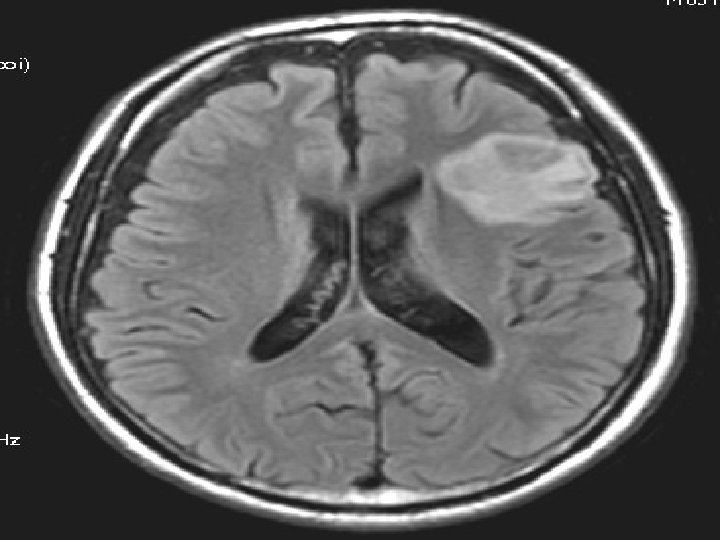
Laboratory Findings: Skull x ray-Brain CT scan&MRIAngiography-MRA-PET&SPECT Evoked potentials-EEG D. D: Stoke-Infection-MS-Sarcoidosis
-90% intracranial Ethiology; Radiation-Trauma? progestrone-Viral Clinical Manifestations: Seizure. Hemiparesis-cranial palsy-IICP")
meningiomas: F>M-6 th&7 th decadechildhood(rarely)-90% intracranial Ethiology; Radiation-Trauma? progestrone-Viral Clinical Manifestations: Seizure. Hemiparesis-cranial palsy-IICP
-AEDs Gliomas: 60%primary brain tumors")
Imaging: x ray-CT-MRI-MRA Treatment: Resection-Radiothrapy. Proton beam- Mifepristone(RU 486 -Chemothrapy(Ifosfamide)-AEDs Gliomas: 60%primary brain tumors low grade- high grade
 Symptoms: Seizure-focal")
<25 years 67% infratentorial >25 years 90% supratentorial Location: white matter (frontaltemporal-frontoparietal) Symptoms: Seizure-focal deficits. Memmory& personality disturbance Treatment: Resection-radiationchemotherapy (carmustin& procarbazin)

Oligodendroglioma: Sensitive to chemothrapy-5% SOL-50 YEARS Symptoms: Seizure-focal deficit Imaging: Hypodensity-calcification Treatment: Resection –Radiation. Chemothrapy(PCV-CCNU)

Ependymoma: 3 -5 years-vomiting Hydrocephalus Location: Ventricles-spinal cord Treatment: Resection-Radiation PNET: Childhood-Mitosis-Invasive Medulloblastoma: Vermis Treatment: Mixed thrapy

Brain Metastasis The most common direct neurological complication of Systemic cancer BM>primary malignant brain tumor times 10 Prostate cancer 1%BM 3% BM ovarian cancer Melanoma 18 -90%BM lung cancer 18 -

Breast cancer 20 -30%BM 20 -40% dying with cancer have BM BM causes : lung(40 -50%)-breast(15 -20%)-melanoma& GI and renal (every one 5 -10

BM 80% supratentorial Pelvic &GI cancer infratentorial Initial manifestation of unknown systemic tumor 10 -30% Lung cancer: the most common cause of BM presentig Without a known primary (66%) NSCLC –GI(10%) Intratumoral hemorrhage; melanoma-choriocarcinomathyroid &renal cell carcinoma

Clinical presentation may arise as long as 20 years after discovery of the primary tumor (breast-melanoma) may antedate discovery primary tumor (lung) progressive over days or weeks (occasionally acute seizure or stroke like) Headache 50%-mental status changes 33% tension like –classic brain tumor headache is uncommon

Headache without other symptoms compatible With multiple metastasis Nausea- vomiting-drowsiness- unilateral weakness- gait disturbance- seizure Signs : hemiparesis &mental status changes (the most common 60%)- IICPpappiledema(10%)

D D : primary SOL-abcess- MS- stroke PML- radiation therapy Neuroimaging: T 2 MRI detect >1 cm diameter MRI with gadolinium improved sensivity multiple metastasis (70 -75%)

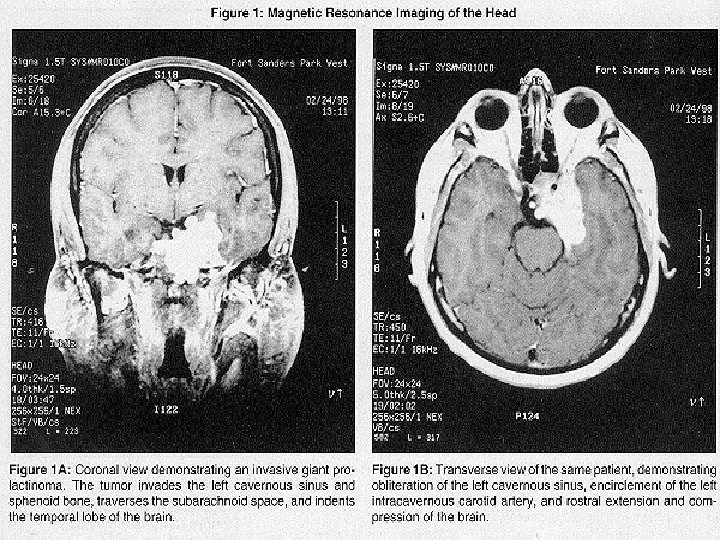
Pituitary tumors: 2/7 -27% M=F 3&4 DECADE-Sporadic-10% inchildhood Secratory&Nonsecratory Prolactinoma; Most common Mixed: 10% Microadenoma---Macroadenoma

Pituitary tumors: 2/7 -27% M=F 3&4 DECADE-Sporadic-10% inchildhood Secratory&Nonsecratory Prolactinoma; Most common Mixed: 10% Microadenoma---Macroadenoma
papilledema(rare Dysfunction of ocular nerves-IICP -DI-Seizure-hemiparesis-dementia")
Adenocarcinoma: Rarely Clinical Manifestations: Mass effect(headache&visual loss &hypopituitarism)papilledema(rare Dysfunction of ocular nerves-IICP -DI-Seizure-hemiparesis-dementia

Management: Evaluation of endocrine-thyroid& adrenal replacement-Bromocriptin -Resection-Radiothrapy Pituitary apoplexy: sever headache-vomiting-nausea
intramedullary 2)intradural 3)extradural intramedullary are rare 10%")
SPINAL TUMORS : Divided by location : 1)intramedullary 2)intradural 3)extradural intramedullary are rare 10% intradural” menengioma-neurofibroma benign encapsulated 65% IM more common in childhood EM are more common in adults The most common primary sites of metastasis : a)lung b) breast c)prostate d)GI, lymphoma, melanoma, renal, ….

M=F SPINAL/BRAIN= 25% meningioma F>M ependymoma M>F pinal tumors occur prodominant in young or middle aged and are less common in childhood or after age 60 years most often ln thoracic region
-ultimately complete loss of function below the level")
Symptoms : Intradural : compression nerve roots-(dorsal)-ultimately complete loss of function below the level of the lesion 1)focal pain &paresthesias 2) sensory loss weakness, wasting 3)cord compression(spastic weak impairment of sensation-impaired control of bladder and rectum

Symptoms continued: overactive DTR –Babinsky sign loss of superficial abdominal reflex Spinal Metastasis : 5 -10%of all cancer patients Epidural spinal cord compression treatment of cord compression does not prolong survival but may relieve pain and prevent disability

Neck or back pain persists when the patient lies in bed even if the pain relieved by analgesics. Limb weakness –paresthiasis in the distribution of nerve rootor bladder dysfunction Rarely the only manifestation of cord compression is a gait disorder (sensory ataxia or spinocerbellar)

Lung-breast-GI-prostate-melanoma =>80% of original site Treatment is palliative Loss of bladder or bowel is an Ominous prognostic sign and is Usually irreversible Radiotherapy is treatment of Choice melanoma_surgical T

Intramedullary metastasis: The most common sites : lung or breast 60% multiple metastasis Death 3 months of diagnosis 80% Primary intramedullary tumors: usually extend over many segments- if restricted to 1 -2 the syndrome is similar to that of an extramedullary tumor sacral sparing- syringimyelia

Intradural tumors neurofibroma: the most common meningioma- schwannoma




- Slides: 42