Hypertension In The Stroke Patient Manas Upadhyaya MD

, aka “high blood pressure, ” is a medical")
 is one of the most major independent risk factors for")







- Slides: 14
Hypertension In The Stroke Patient Manas Upadhyaya, MD Vascular Neurology Fellow, UICOMP Stroke Summit April 28, 2017
WHAT IS HYPERTENSION? • Hypertension (HTN), aka “high blood pressure, ” is a medical condition in which the blood pressure in the arteries is elevated • Can be primary (no identifiable cause, 90 -95%) or secondary (ie: thyroid dysfunction, renal artery stenosis, 5 -10%) • Measured as the systolic BP/diastolic BP • Different classifications and grades, but typically “normal” BP is <120/80; HTN when >140/90
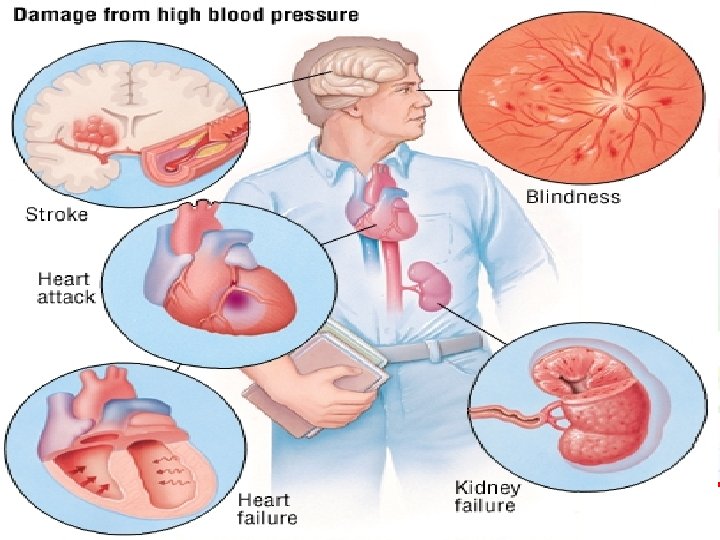
EPIDEMIOLOGY • Hypertension (HTN) is one of the most major independent risk factors for CAD, stroke, heart failure, and renal failure • Almost 1 in every 3 Americans has HTN! • Americans >55 yo have a 90% lifetime risk of developing HTN • HTN related healthcare costs exceeds $50 billion every year (Hernandez-Vila, 2015)
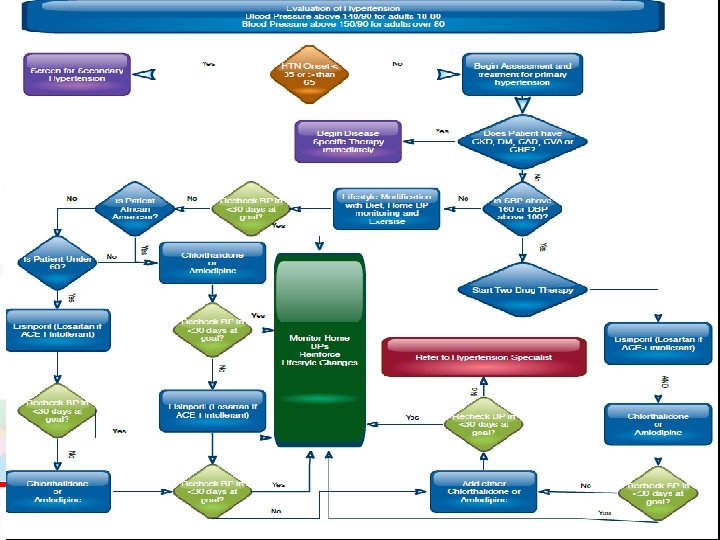
UPDATED JNC 8 GUIDELINE FOR THE MANAGEMENT OF HIGH BP IN ADULTS • Recommendation 1. The guideline recommends the initiation of drug therapy in order to lower a systolic BP (SBP) of ≥ 150 mm. Hg or a diastolic BP (DBP) of ≥ 90 mm. Hg for the general population at 60 years of age or older (Grade A). A corollary recommendation is that patients whose achieved SBP on pharmacologic therapy is lower than the new guideline recommendation can be continued at that level of therapy, if well tolerated (Grade E). • Recommendation 2. The target DBP to start pharmacologic therapy for subjects younger than 60 years of age is ≥ 90 mm. Hg. On the basis of available evidence, the recommendation for patients aged 30 to 59 years is strong (Grade A). For those between the ages of 18 and 29, the recommendation is on the basis of expert opinion (Grade E).
JNC 8 GUIDELINES CONT. • Recommendation 3. The target SBP to start pharmacologic therapy for subjects younger than 60 years of age is ≥ 140 mm. Hg (Grade E). • Recommendation 4. In the population aged 18 years or older with chronic kidney disease, initiate pharmacologic treatment to lower BP at SBP ≥ 140 mm. Hg or DBP ≥ 90 mm. Hg and treat to a goal of SBP <140 mm. Hg and a goal of DBP <90 mm. Hg (Grade E). • Recommendation 5. The target blood pressure in beginning pharmacologic therapy for the diabetic population aged 18 years or older is <140 mm. Hg for SBP and <90 mm. Hg DBP (Grade E). • Recommendation 6. Initial drug therapy for nonblack patients (including diabetic patients) should include a thiazide-type diuretic, a calcium channel blocker, an angiotensin-converting enzyme (ACE) inhibitor, or an angiotensin receptor blocker (Grade B).
JNC 8 GUIDELINES CONT. • Recommendation 7. Initial drug therapy for black patients should include a thiazide-type diuretic or a calcium channel blocker. This includes patients with diabetes mellitus (Grade B; for diabetic black patients, Grade C). • Recommendation 8. For patients 18 years and older with chronic kidney disease, initial or additional therapy should include an ACE inhibitor or angiotensin receptor blocker, regardless of race or diabetic status (Grade B). • Recommendation 9. An algorithm for managing patients who do not achieve control within one month is recommended. If the goal is not achieved, increase the dose of the initial drug or add a 2 nd drug from one of the classes in recommendation 6. A 3 rd drug should be added if the goal is not achieved with 2 drugs. Drugs from other classes can be used if the target is not achieved with the recommended classes, or if there is a contraindication to one of the recommended drug classes. ACE inhibitors should not be combined with angiotensin receptor blockers in the same patient. Referral to an HTN specialist should be considered in complicated cases or in the event of inability to control BP (Grade E). 5
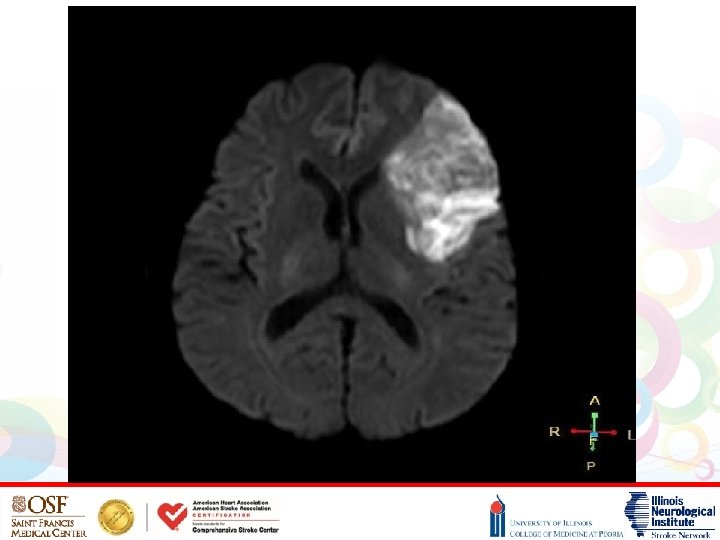
HYPERTENSION AND STROKE • HTN is one of the most modifiable risk factors in stroke neurology • Uncontrolled blood pressure can lead to a 4 -6 x increase in risk for stroke! • In the long term, HTN causes atherosclerosis (hardening of the arteries), which can cause blockage of the small blood vessels in the brain • 75% of patients w/ acute ischemic stroke have elevated BP at the time of presentation!
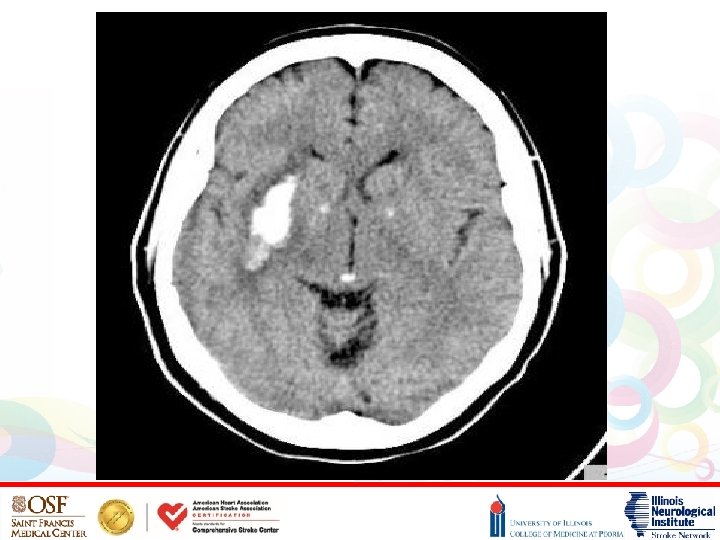
HYPERTENSIVE INTRACEREBRAL HEMORRHAGE • HTN is also the most common cause of intracerebral hemorrhages • Patho-physiologically, long-standing poorly controlled HTN leads to formation of microaneurysms of perforating arteries (Charcot-Bouchard aneurysms) • These small penetrating arteries can leak or rupture leading to hemorrhagic strokes • The most common locations for hypertensive hemorrhages include the basal ganglia (particularly the putamen), thalamus, pons, and cerebellum (Di. Muzio, Radiopedia, 2017)
HTN MANAGEMENT IN THE ACUTE STROKE PATIENT • BP goals: -maintain SBP<220 in acute ischemic stroke -maintain SBP<180 in acute ischemic stroke when given IV thrombolytics or w/ IV anticoagulation -maintain SBP<140 in acute hemorrhagic stroke • Medications: -hold home anti-hypertensives -nicardipine or clevidipine as titratable drips -labetalol and hydralazine as prn IV medications • Over the next 24 -72 hrs, begin to relax BP parameters depending on etiology of stroke and re-start home anti-HTNs • Best way to prevent recurrent strokes is long-term tight control of BP!
REFERENCES • Di. Muzio, Bruno, Frank Gaillard, et al. In Radiopedia. Retrieved April 26, 2017. • Grotta, James, et al. Stroke: Pathophysiology, Diagnosis, and Management. 2015; 242, 283 -285, 471. • Hernandez-Vila E. A Review of the JNC 8 Blood Pressure Guideline. Texas Heart Institute Journal. 2015; 42(3): 226 -228. doi: 10. 14503/THIJ-15 -5067. • Hypertension. (2017, April 26). In Wikipedia, The Free Encyclopedia. Retrieved 10: 55, April 26, 2017, from https: //en. wikipedia. org/w/index. php? title=Hypertensi on&oldid=777277379