By f rezaei NEUROMUSCULAR DISEASES Cerebrovascular Disease cerebrovascular

By: f. rezaei NEUROMUSCULAR DISEASES
, or complete stroke, is a sudden impairment in cerebral")
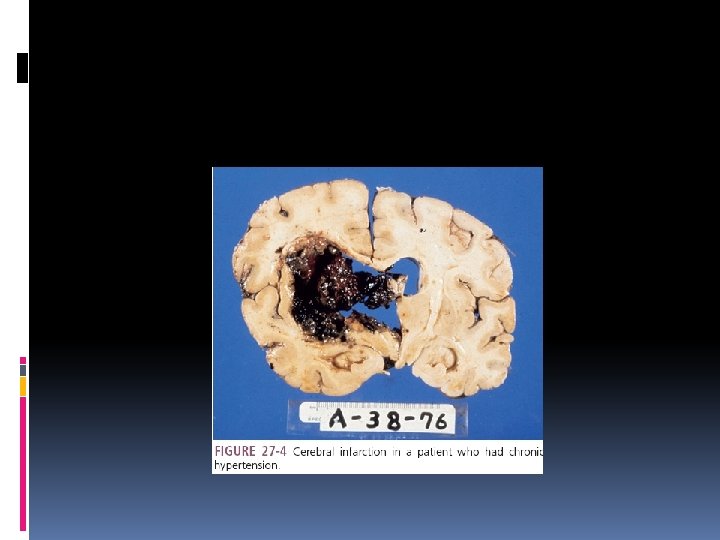
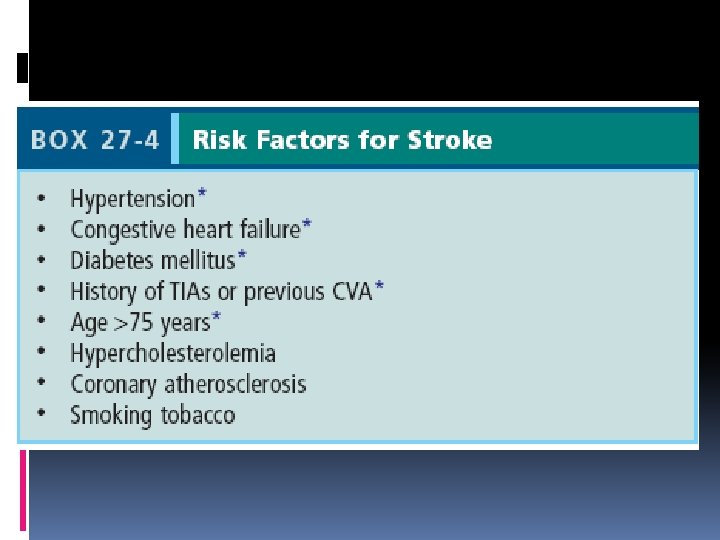
Cerebrovascular Disease cerebrovascular accident (CVA), or complete stroke, is a sudden impairment in cerebral circulation. TIA(transient ischemic attack), RIND(reversible ischemic nuerologic defect) 15% : hemorrhagic events du to hypertension, truma, subestance abuse, 85%: ischemia due to atherosclerotic disease, thromboembolic events, and occlusion of cerebral blood vessels Hypertension is the most important risk factor
 in extraocular muscles and eye movements,")
Clinical Manifestations Sensory and motor deficits, changes (paresis) in extraocular muscles and eye movements, visual defects, sudden headache, altered mental status, dizziness, nausea, seizures, impaired speech or hearing, and neurocognitive deficits such as impaired memory, reasoning, and concentration.

Diagnosis treatment MRI and CT CBC, comprehensive metabolic panel, urinalysis, coagulation profile, and, when indicated, blood culture, echocardiography, and lumbar puncture. Reduce bleeding or thromboembolic occlusion, to reduce brain edema and neurotoxicity/nerve injury, and surgical interventions (revascularization, hemorrhage control). Thrombolysis with intravenous tissue plasminogen activator (t-PA) within 3 hours of a stroke can improve reperfusion

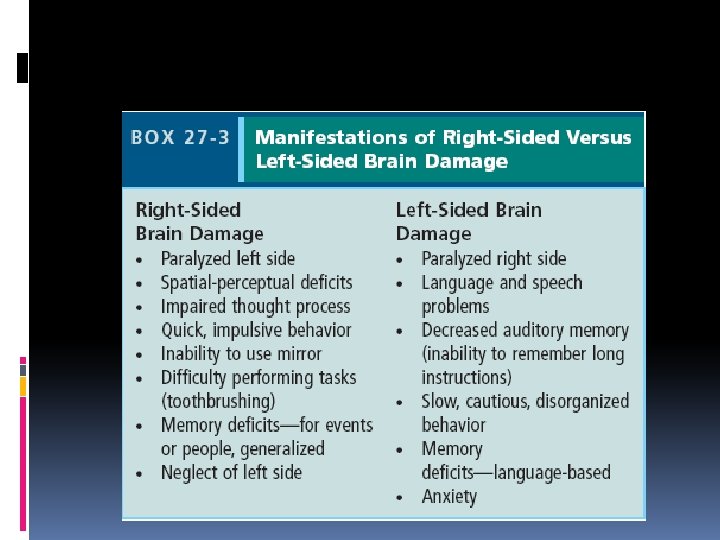
Oral Health Considerations Patients with right sided brain damage may neglect the left side(caries , periodontal disease and halitosis) Calcified atherosclerotic plaques in carotid arteries of elderly, and diabetic on panoramic films, indicates a risk for stroke ……referral to physician for evaluation Exact causative relationship between periodontal disease and stroke remain to be define

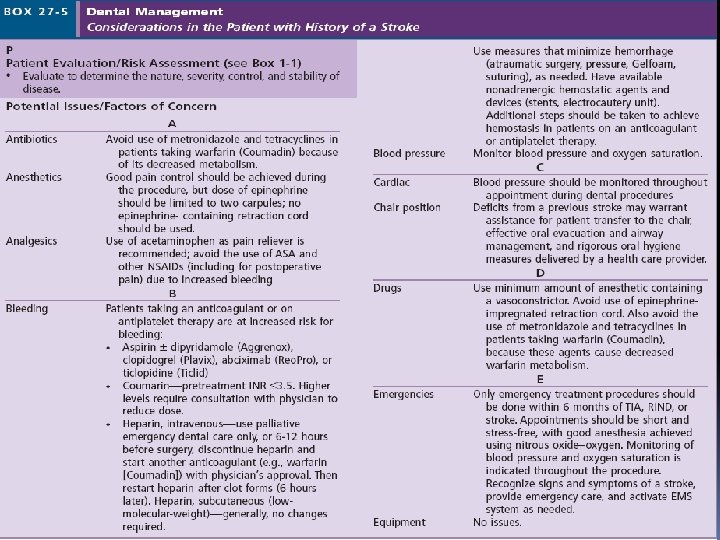
Oral Health Considerations masticatory and facial muscle paralysis, impaired or lost touch and taste sensation, diminished protective gag reflex, and dysphagia. poor oral hygiene: risk for caries and periodontal disease. Creative and effective use of adjuvant oral hygiene techniques and devices (oral antimicrobial rinse, oral irrigation, floss holders) antiplatelet and anticoagulant medications(ticlopidine, clopidogrel, aggrenox )
 may increase the risk for bleeding, metronidazole, erythromycin, and tetracycline,")
Oral Health Considerations (NSAIDs) may increase the risk for bleeding, metronidazole, erythromycin, and tetracycline, which may alter the bioavailability of warfarin. Stress reduction (inhalation N 2 O-O 2 or oral anxiolytic medication) Use of epinephrine-containing local anesthetics is not strictly contraindicated
")
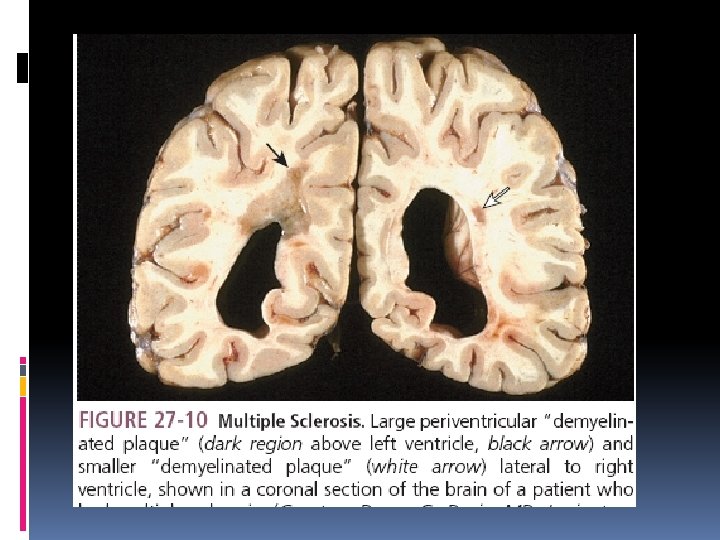
Multiple Sclerosis Etiology MS is characterized by multiple areas of central nervous system (CNS) white matter inflammation, demyelination. The age at onset is typically between 20 and 40 years MS lesions or “plaques” vary in size and are characterized by perivenular cuffing with inflammatory mononuclear cells, predominantly macrophages and T cells,

Clinical Manifestations sudden onset of optic neuritis : first symptom of MS. Limb weakness is characteristic of MS and can manifest as loss of strength or dexterity, fatigue, or gait disturbances. muscle spasms is often observed in the legs scanning speech Bladder dysfunction and bowel dysfunction paresthesia and hyperesthesia, depression, and cognitive dysfunction relapsing/remitting

Clinical Manifestations exacerbation of neurologic symptoms in response to an elevation of the body’s core temperature. This is referred to as Uhthoff’s symptom and is often seen in response to increased physical activity. electric shock–like sensations that are evoked by neck flexion and radiate down the back and into the legs. This is referred to as Lhermitte’s symptom. Myokymia

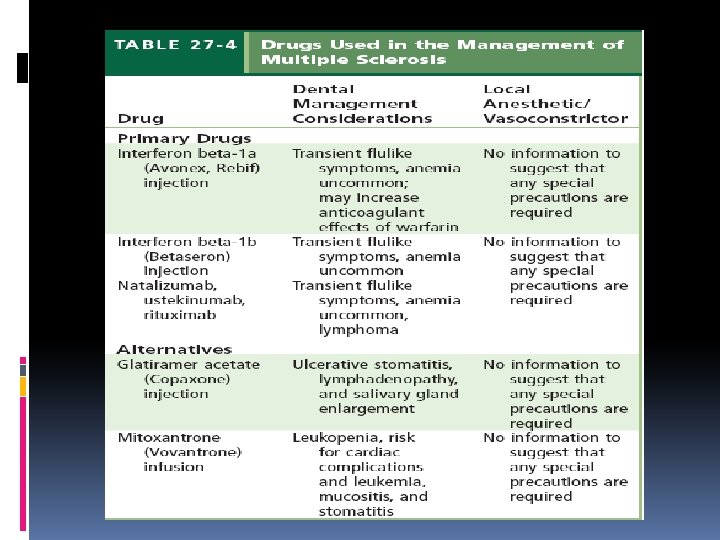
Diagnosis treatment NO definitive diagnostic test MRI Analyze of CSF Therapy for MS divided into three categories: (1) treatment of acute attacks, (2) treatment that reduces the biologic activity of MS, and (3) symptomatic therapy.

Oral Health Considerations TGN: absence of trigger zones and continuous pain with lower intensity. Medications often used to manage TGN are similar to those used for treatment of idiopathic TGN. Neuropathy of V 2, V 3 Facial weakness and paralysis dental treatment in an operating room under general anesthesia

Oral Health Considerations Optimal time for treatment is remission period Anticholinergic and TCA cause BMS: salivary substitutes, pilocarpine Immunosuppressants drug: opportunestic infection, cancer

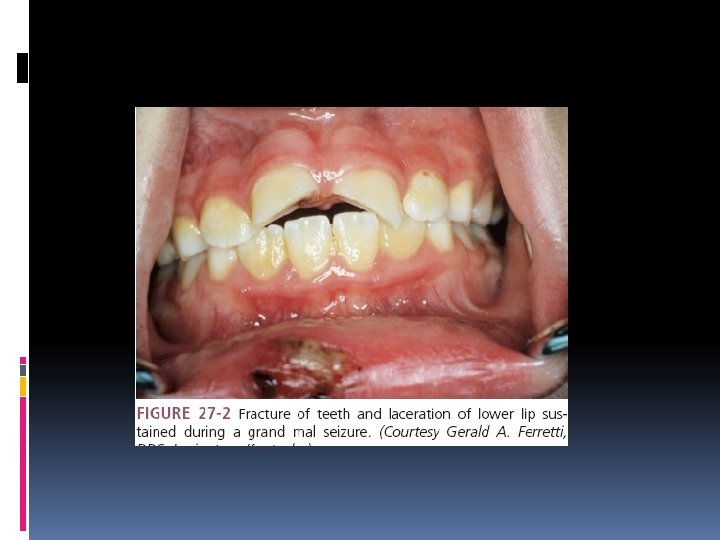
Seizure Disorders Etiology: seizure is a paroxysmal event due to abnormal, excessive, hypersynchronous discharges from neuronal aggregates in the CNS. epilepsy : condition in which a person has recurrent seizures due to a chronic, underlying process. Tonic-clonic (grand mal) seizures are generalized seizures that present with dramatic clinical features, tonic contracture and uncoordinated clonic muscular movements.

etiology Idiopatic in more than half of all Cerebrovascular disease, cavernous malformation , intracranial neoplasms(glioma), head trauma(35%) Hypoglycemiam, drug withdrawal, infection, febrile illness(meningitis, encephalitis), hypotension, Down syndrome

Clinical Manifestations Photosensitivity epilepsy is characterized by seizure activity induced by visual stimuli Aura (unusual smell or visual disturbance) precedes convulsion in 1/3 patients Epileptic cry(spasm of diaphragmatic muscles) Tonic phase(muscle rigidity, rolling eyes upward breating may stop) Clonic phase(uncoordinated movements of limbs and head, jaw closing) Urinary incontinence

Diagnosis CT, MRI CBC, electrolytes, glucose, magnesium, and calcium complete neurologic examination EEG is mandatory for patients with suspected seizures is critical for classifying seizure disorders as well as helping to determine the type of anticonvulsant medication, if indicated.

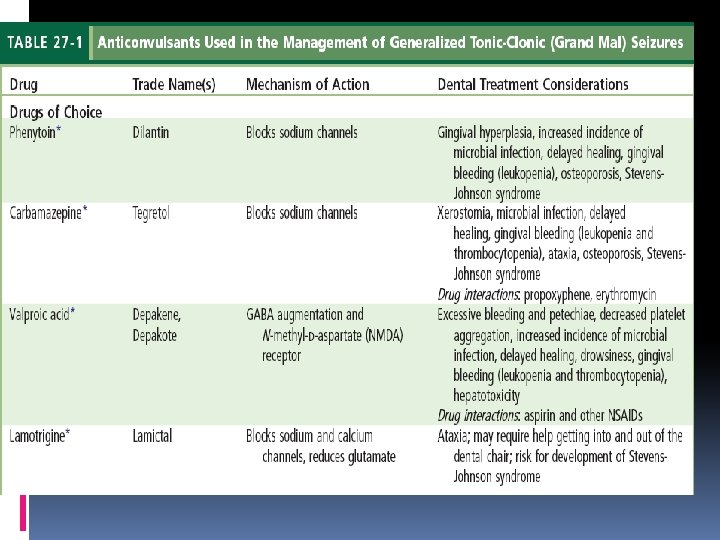
treatment Lamotrigine, carbamazepine, or phenytoin Phenytoin is associated with gingival overgrowth, hirsutism, and coarsening of facial features. Carbamazepine can cause hepatotoxicity, leukopenia, and aplastic anemia, whereas lamotrigine has been associated with skin rash. Valproic acid may cause bone marrow suppression and hepatotoxicity, requires laboratory monitoring,

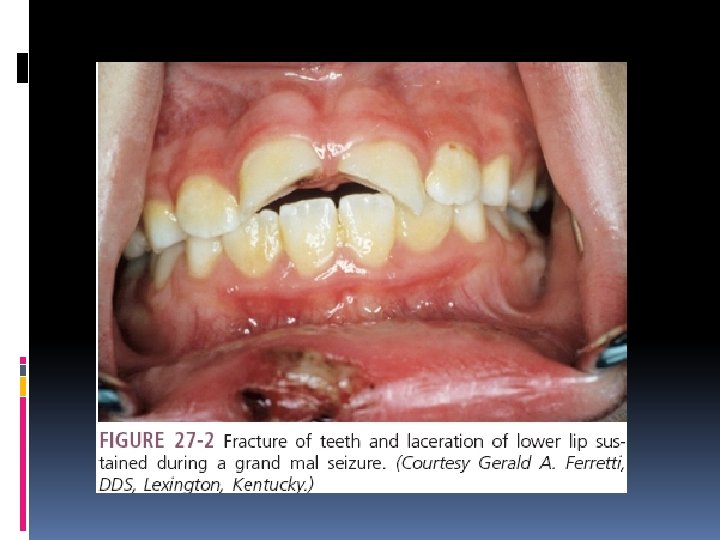
Oral Health Considerations Important features for the clinician to assess include the type of seizures, etiology of seizures, frequency of seizures, known triggers of seizure activity, presence of aura prior to seizure activity, and history of injuries related to seizure activity. avoid any known triggers of the patient’s seizure activity. Anticonvulsant medications can induce significant blood dyscrasias resulting in an increased incidence of microbial infection, delayed healing, and both gingival and postoperative bleeding. Hepatotoxicity,

Oral Health Considerations Gingival overgrowth: (The anterior labial surfaces of the maxillary and mandibular gingivae are most commonly affected and may be seen within 2 to 18 months after starting the medication) phenytoin alters molecular signaling pathways that control collagen degradation by gingival fibroblasts and accumulation of collagen leads to clinically evident gingival overgrowth. Inflammation can exacerbate this condition Occurs in youngesters than in adults

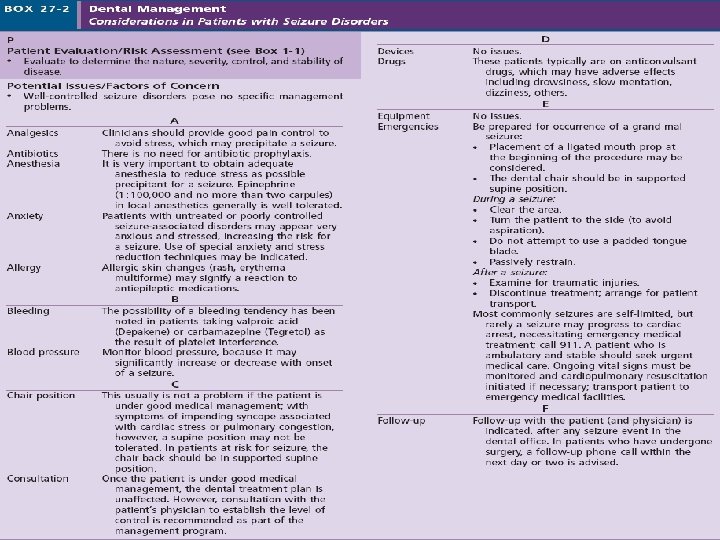

Seizure Management Premedication: 0. 5 to 2 mg of lorazepam can be given sublingually, or diazepam 2 to 10 mg can be given intravenously. In the event that a seizure becomes prolonged (status epilepticus) or is repeated, intravenous lorazepam (0. 05 to 0. 1 mg/kg) 4 to 8 mg, or 10 mg diazepam, generally is effective in controlling it.

Treatment planning consideration Optimal level of oral hygiene Missing teeth should be replaced Fixed prosthesis or implant is preferable to removable one All metal unit is preferable to PFM to minimize fracture In removable prostheses metallic plates and base are preferable to all acrylic ones


- Slides: 36