Abnormal Psychology This is not a course about

Abnormal Psychology This is not a course about the problems of someone else. Mental illness touches all of us at some time during our lives; if we are not the ones afflicted, then it will be a family member, loved one, or close friend. The problem of abnormal behavior is personally relevant and emotionally charged, but in this course we will explore the problem from an objective and scientific point of view. Although we must be dispassionate in our study of the problem, it is important that we keep in mind the importance and the intense personal ramifications of what we are studying.

Psychopathology . . . beyond behavior 1. Thought: l 2. Emotion: l 3. problems in how and what we think problems in momentary mood and chronic temperament Conation: l problems in momentary motives and persistent needs. . . the “subject matter” and the “data base”

The Definition of “Psychopathology” Topics: The importance of the historical context A. Understanding: scientific description and Understanding explanation. . . the history of our curiosity B. Intervention: the change technologies Intervention. . . the history of our compassion

History . . . of understanding and intervention 3 broad perspectives on both: 1. Sociocultural: natural and supernatural 2. Biological: body and brain 3. Psychological: three theories of the mind

. . . and a narrow-minded tradition Understanding Theory Cause Intervention Therapy Cure/Care

Examples: 1. Biology: Biology from the four humors to the monoamines 2. Psychology: Psychology three “meta-theories” 3. A. Learning Theories: adaptation to the present and the behavior and cognitive therapies B. Phenomenological Theories: growth into the future and the directive and non-directive therapies C. Psychodynamic Theories: conflict from the past and the psychoanalytic therapies Sociocultural factors: Sociocultural factors natural and supernatural

People and their Problems People. . . the recurrent millennia of history Understanding problems, in the past the causes of problems Intervening with people, in the future the course of life
. . . focus")
Some comparisons. . . 1. Simple mechanical objects (cars and clocks). . . focus on cause 2. More complex situations (soups and sauces). . . focus on effect 3. The complexity of life (you and I). . . focus on resilience

Implication . . . “problems” as solutions to problems Factors in the. . cause (past) content (present) course (future)

Common confusions A. Theory Therapy example: “therapeutic nihilism” B. Therapy Theory example: “post hoc explanations”

History of psychopathology History. . . the myth and the reality “Those who don’t study history more carefully are condemned to repeat it. ” - George Santayana

History of psychopathology History. . . the myth and the reality 1. Ancient writings & archaeological evidence Ø Ø Homer The Hebrews Trephining Asclepius

History of psychopathology History. . . the myth and the reality 2. Biogenesis: Hippocrates and “the four humors” Sanguine Ø Choleric Ø Phlegmatic Ø Melancholic Ø e. g. , hysteria

History of psychopathology History. . . the myth and the reality 3. Psychogenesis: Plato and "the tripartite mind“ Ø Ø Affect Appetite Reason Self-management e. g. , catharsis

History of psychopathology History. . . the myth and the reality 3. The Roman Era and The Middle Ages Ø The Roman Era : Galen and beyond Ø The Middle Ages : “The Dark Ages” (450 – 1450 A. D) § § The Arab World : • Egypt and Avicenna The Western World : • France • Italy • Britian • Gheel • St. Augustine

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions A. The Return of the Supernatural View Witches . . . and the rise of the asylum

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions A. The Return of the Supernatural View Witches . . . and the rise of the asylum

History of psychopathology History. . . the myth and the reality Three Threats: 1. Physical: “The Black Death” 2. Religion: “The Reformation” 3. Social: “The Little Ice Age”

History of psychopathology History. . . the myth and the reality The Solution: Malleus Maleficarum: (and Thesaurus Exorcismorum) A witching trial during the Salem Witch Hunt

History of psychopathology History. . . the myth and the reality The Solution: Marvin Harris

History of psychopathology History. . . the myth and the reality The Asylum London: St. Mary’s of Bethlehem Paris: La. Bicêtre Salpêtrière St. Mary’s of Bethlehem

History of psychopathology History. . . the myth and the reality The Asylum London: St. Mary’s of Bethlehem Paris: La. Bicêtre Salpêtrière

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality The Challenge: – St. Thomas Aquinas, from the Middle Ages – Johann Weyer Deception of Demons Johann Weyer St. Thomas Aquinas

History of psychopathology History. . . the myth and the reality The Challenge: – Reginald Scot The Discovery of Witchcraft

History of psychopathology History. . . the myth and the reality The Challenge: – Teresa of Avila

History of psychopathology History. . . the myth and the reality The Challenge: – Teresa of Avila

History of psychopathology History. . . the myth and the reality The Challenge: – Paracelsus

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions B. The “Mental Hospital Movement” Paris: Philippe Pinel and Jean Baptiste Pussin Dorothea Dix

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions B. The “Mental Hospital Movement” London: William Tuke . . . and the York Retreat Dorothea Dix

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions B. The “Mental Hospital Movement” The York Retreat Dorothea Dix

History of psychopathology History. . . the myth and the reality 4. The Renaissance and the Revolutions B. The “Mental Hospital Movement” America: Dorothea Dix . . . and “moral management” Clifford Beers . Dorothea Dix . . and “the mental hygiene movement” Clifford Beers

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality 5. The Psychiatric Revolution: the return of biogenesis

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality 5. The Psychiatric Revolution: the return of biogenesis Louis Pasteur Benjamin Rush

History of psychopathology History. . . the myth and the reality 5. The Psychiatric Revolution: the return of biogenesis Ignaz Phillip Semmelweis Edward Jenner Louis Pasteur

History of psychopathology History. . . the myth and the reality 5. The Psychiatric Revolution: the return of biogenesis William Farr Paul Broca John Snow

History of psychopathology History. . . the myth and the reality 5. The Psychiatric Revolution: the return of biogenesis Korsakoff Alzheimer Wernicke

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality The Story of General Paresis Diagnosis. . . from cases to syndromes History. . . from correlates to causes Treatment. . . from causes to cures

History of psychopathology History. . . the myth and the reality Ehrlich’s “magic bullet”

History of psychopathology History. . . the myth and the reality Along the way. . Ø Ø Ø anti-sexualism degeneracy theory phrenology

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality The Medical View: Emil Kraepelin Wilhelm Griesinger Jean-Martin Charcot

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality 6. Psychodynamic theory and psychoanalysis: The return of psychogenesis Liebault & Bernheim: Freud & Breuer: “psychoneurosis” The case of Anna O

History of psychopathology History. . . the myth and the reality The case of Anna O

History of psychopathology History. . . the myth and the reality

History of psychopathology History. . . the myth and the reality 7. The “Mental Health Movement” Mental Health Movement the return of sociogenesis, again sociogenesis Ø Sociologists Ø Anti-Psychiatry Ø Clinical Psychology . . . and then, something happened. . .

History of psychopathology History. . . the myth and the reality 8. The “New Psychiatry” The return of biogenesis, biogenesis again Ø Drugs and the Drugs search for biological causes biological Ø The technologies and technologies an integrated approach Heinz Lehmann

The Lesson of History Lesson “The lessons of the past were obliterated by the aspirations of the present. ” - Alexander Leighton

The Lesson of History Lesson “It ain’t what you don’t know that gets you; it’s the things you know that ain’t so. ” - Mark Twain

The Lesson of History Lesson “Confusion now hath made his masterpiece. ” - Mac. Beth

The Lesson of History Lesson . . . Limitations to Progress 1. Understanding (finding causes): Ø post hoc explanations Ø correlates and causes Ø longitudinal and experimental research Ø the problem of base rates (BR)

The Lesson of History Lesson . . . Limitations to Progress 2. Intervention (finding cures): Ø placebo effects Ø spontaneous remission (SR) Ø superstitious behaviour Ø publication bias

The Lesson of History Lesson . . . Limitations to Progress Summary: 1. Understanding: it is hard to find out why something why happens when it doesn’t happen very often 2. Intervention: it is hard to find out if anything makes a difference to the course when that course is difference erratic and unpredictable erratic

Definitions 1. Theoretical/absolute criterion Ø demons Ø diseases Ø defects Making inferences and pathologizing the results inferences pathologizing

Definitions 2. Social/cultural criterion Ø deviance Ø difference Ø disgust Making discriminations and pathologizing the minority discriminations pathologizing

Definitions 3. Personal/subjective criterion Ø distress Ø dysphoria Ø despair Making introspections and pathologizing unhappiness introspections

Definitions The common-sense criterion: Maladaptation/symptoms Ø disorder Ø dysfunction Ø disability thoughts & perceptions emotions & feelings needs & motives
 Why diagnosis? . . . a present description .")
The Modern Diagnostic System (DSM) Why diagnosis? . . . a present description . . . with future implications “Diagnosis is prognosis”
 Ø DSM I (1952) and DSM II (1968) Ø")
The Modern Diagnostic System (DSM) Ø DSM I (1952) and DSM II (1968) Ø DSM III (1980) and DSM IV (1994). . . TR, now Ø ICD 1 (1948) to 10 (1992). . . CM, now
 What have we gained? 1. Research: no false positives")
The Modern Diagnostic System (DSM) What have we gained? 1. Research: no false positives Research 2. Practice: no false negatives Practice. . . communication – in principle. . . but research biases in practice biases
 Axis I - Clinical syndromes Axis II - Personality disorders")
Diagnosis of psychopathology (DSM) Axis I - Clinical syndromes Axis II - Personality disorders (and MR) Axis III - Medical conditions Axis III Axis IV - Stress Axis IV Axis V - Coping (GAF) Axis V -
 “Other conditions that may be the focus of clinical attention”,")
Diagnosis of psychopathology (DSM) “Other conditions that may be the focus of clinical attention”, including psychological factors affecting medical conditions, and the “V” code.
 Issues: 1. reliability & validity 2. categories, dimensions & prototypes")
Diagnosis of psychopathology (DSM) Issues: 1. reliability & validity 2. categories, dimensions & prototypes (“polythetic” classification) 3. comorbidity, artifactual & real 4. subjectivity & biases 5. the problem of labeling

Extent of psychopathology: . . . prevalence, incidence and life-time risk Some “ball-park” figures: (Canada) Axis 1 Axis II Disorder BR 12 Life-Time Risk Treatment Ratio Anxiety disorder 18% (12%) 30% (20%) 1 in 7 Affective disorder 9% (6+%) 17% (12+%) 1 in 4 Thought disorder 1% 1+% 1 in 2 Personality disorder 7% 9% unknown Totals 20 - 30% - 40+% 1 in 5

Extent of psychopathology: . . . prevalence, incidence and life-time risk Prevalence Life-Time Risk Drugs 6% (8%) 15% (20%) MR 2% 2%

Causal Factors and Viewpoints Causation in psychopathology 1. 2. 3. 4. Primary / necessary and sufficient causes Predisposing / contributory causes (and the concept of "relative risk") Precipitating / proximal and distal causes Perpetuating / reinforcing (maintaining) causes

Causal Factors and Viewpoints The nature of causal complexity . . . not necessarily the number of causes number. . . but the causal pattern i. e. , living systems are self-regulating

Causal Factors and Viewpoints An overall conception: Diathesis-Stress . . . the original additive model additive . . . the newer interactive model interactive i. e. , living systems are resilient

Theoretical Perspectives Why do we need them?

Theoretical Perspectives A. Biological: . . . from simplistic to sophisticated l The Psychiatric Revolution – l circular reasoning The New Psychiatry – – – technology conceptualization causation

Theoretical Perspectives A Modern Checklist: 1. Genes a. direct influence b. indirect (passive, evocative, active) influences c. interactive influence 2. Congenital Factors 3. Constitutional Factors a. the role of neurobiological inhibition b. the role of evolution c. aspects of temperament
 Anxiety, Depression Positive Affect")
Theoretical Perspectives TEMPERAMENT: CHILD Fearfulness Irritability/Frustration ADULT Negative Affect (“Neuroticism”) Anxiety, Depression Positive Affect Activity Level Positive Affect (“Extroversion”) Adventurousness, Dominance Attentional Persistence “Conscientiousness” “Agreeableness” Also: Sociability… Inhibition…. “Openness”

Theoretical Perspectives B. Psychological: The Three Meta-Theories I. Psychodynamic theory – Conflict and its management Psychoanalysis

Theoretical Perspectives Psychological: The Three Meta-Theories B. II. Learning theory Adaptation and its means a. b. Classical Conditioning & “experimental neurosis” Operant Conditioning & “superstitious behavior”
 SHOT RSTARTLE (reflex) CSWP - SHOT RSTARTLE CSWP")
Theoretical Perspectives 1. Classical conditioning (“aversion”) SHOT RSTARTLE (reflex) CSWP - SHOT RSTARTLE CSWP CRSTARTLE. . . and extinction 83
 R SHOT RJUMP - SHOT (reward) SHOT RJUMP.")
Theoretical Perspectives 2. Operant conditioning (“escape”) R SHOT RJUMP - SHOT (reward) SHOT RJUMP. . . and extinction 84
 3. CSWP RJUMP (reward? ) R CSWP RJUMP")
Theoretical Perspectives “Two factor” conditioning (“avoidance”) 3. CSWP RJUMP (reward? ) R CSWP RJUMP - SFEAR . . . and extinction? 85

Theoretical Perspectives c. Cognition & “negative sets” S R S O R Cognitive and behavior therapies e. g. Rational-emotive and other cognitive therapies 86
 theory Growth and")
Theoretical Perspectives B. Psychological: The Three Meta-Theories III. Phenomenological (and “humanistic”) theory Growth and its direction “client-centered” and directive therapies

Theoretical Perspectives Psychological theories and circular reasoning A. A Modern Checklist Psychological factors in psychopathology 1. Causes and correlates 2. The power of protective factors

Theoretical Perspectives C. Sociocultural: The Rise and Fall Examples of “culture bound disorders” culture bound disorders • Latah • Koro • Amok • Berserk • Kitsunetsuki • Pibloqtok • Lycanthropy • The Windigo Psychosis

Theoretical Perspectives C. Sociocultural: Sociocultural factors in psychopathology 1. Content : how & how much Content 2. Course : how long Course 3. Cause : why Cause

Theoretical Perspectives C. Sociocultural: Sociocultural theories and circular reasoning Example: the relation between “exit events” and clinical depression
 had an")
Theoretical Perspectives EXAMPLE: “ 25% of people experiencing Major Depressive Disorder (MDD) had an exit event. ” “Only 5% of the control group without MDD had an exit event. ” (“Exit Event”=physical departure of a significant person in the last six months”) Do exit events cause MDD? Base rate for MDD (point prevalence): 2% Take a population of 10, 000 adults. . . 200 MDD. . . 25% with exit events = 50 9800 not MDD. . . 5% with exit events = 490 So, we have 540 exit events, with fewer than 10% associated with MDD

Theoretical Perspectives C. Sociocultural: Social problems and the presumption of psychiatric causes Examples: suicide crime child molestation

Stress and the Adjustment Disorders Stress The General Adaptation Syndrome: How stressors are stressful in the diathesis-stress model
")
Stress and the Adjustment Disorders Measurement l DSM – l (Axes IV and V) Self-report procedures – (LCUs and beyond)
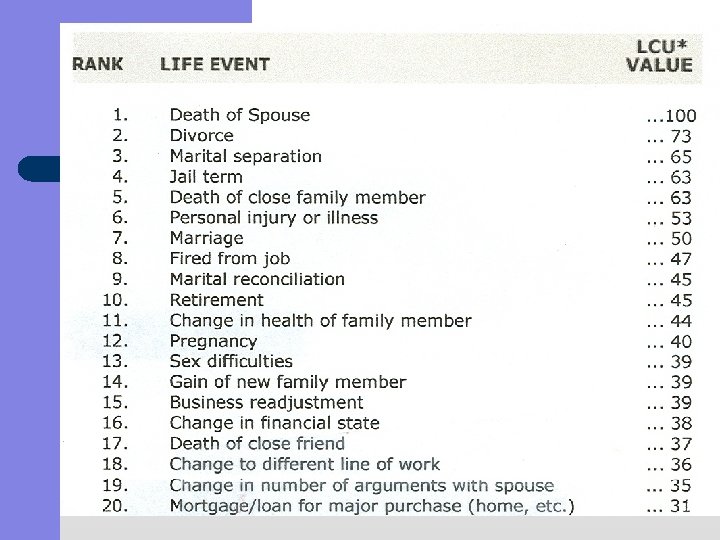
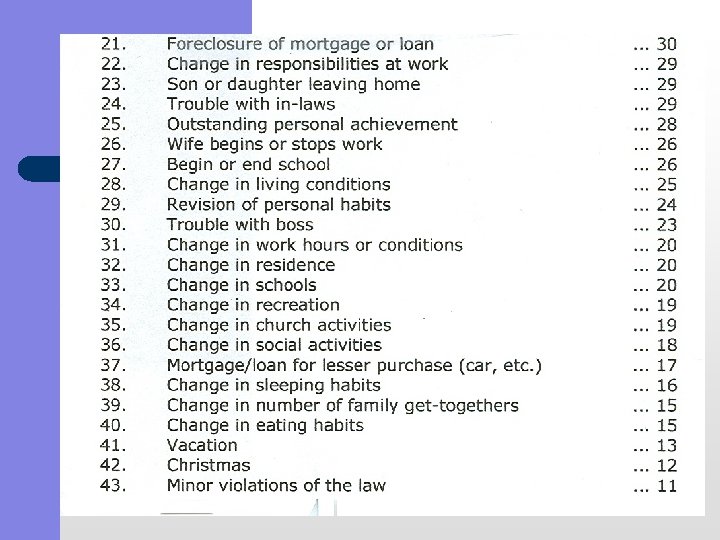

Stress and the Adjustment Disorders Results – – – Frustrations Conflicts Pressures e. g. the hassle list and stress-induced analgesia

Stress and the Adjustment Disorders Coping: 1. 2. Task-oriented, problem solving method Defense-oriented, emotion focused method “God grant me the serenity to accept the things I cannot change, the courage to change things I can, and the wisdom to know the difference” - Reinhold Niebuhr

Stress and the Adjustment Disorders Coping: The big factor in choosing: choosing “self –perceived competence” . . . and its ramifications The big factor in coping: coping social support . . . e. g. the Alberta Study

The Special Case of Extreme Stress Results: 1. 2. “transient decompensation” “residual fear” e. g. The Disaster Syndrome : shock, suggestibility and survival The conventional findings. . . and the caveat e. g the “allostatic load”
 1. 2.")
The Special Case of Extreme Stress Coping: The “Ur” defenses (“Positive illusions”) 1. 2. 3. Our immortality The omnipotent servant Our kindness to one another Also: The Polyanna Principle The Belief in a Just World

Adjustment Disorders Dx: inference of the causal importance of stress Types: – – – depressed anxious conduct disturbance. . . “mixed” types “N. O. S”
")
Anxiety Disorders Related to Extreme Stress Acute Stress Disorder and Post-Traumatic Stress Disorder (PTSD) Crucial for Dx: re-experiencing of an extremely traumatic event The demographics of PTSD: BR and SR Why do some people develop PTSD? – – – The nature of the trauma The nature of the person The nature of subsequent experience Implications for treatment: – – Social support, “debriefing”, exposure & stress-induced analgesia The crisis in “Crisis-Counseling”

Anxiety Disorders Note: Adjustment disorder with anxious mood Substance-induced anxiety disorder Anxiety disorder due to general medical condition

Anxiety Disorders Anxiety Normal vs. abnormal, Primary vs. secondary diagnoses An aspect of temperament (trait) and mood (state)…. …with biological components: GABA and the monoamines in “negative emotionality”

Anxiety Disorders Phobia: specific, social and 1. agoraphobia BR: irrational fears and phobias Treatment and SR

Anxiety Disorders Understanding phobias a. Learning theory: situational causes e. g. Little Albert

Anxiety Disorders Understanding phobias b. Psychodynamics: dispositional causes e. g. Little Hans

Anxiety Disorders Specific phobias: Traumas and dispositional factors e. g. “the immunization effect” Note: “preadaptation” and “the inflation effect”

Anxiety Disorders Social phobias: Experiential and dispositional factors e. g. “social sensitivity” & “automatic thoughts” Treatments Exposure: systematic desensitization (vs. flooding) and chemotherapies

Anxiety Disorders 2. Panic: with or without agoraphobia BR: with or without phobia Understanding panic a. Biology: monoamines in “the fear network” Nature and nurture b. Psychology: “anxiety sensitivity” Conditioning: “Fear of Fear Model” Cognition: “Cognitive Model” Treatments Chemotherapy and PCT
 BR: primary and secondary GAD Understanding GAD Psychodynamic")
Anxiety Disorders 3. Generalized Anxiety (GAD) BR: primary and secondary GAD Understanding GAD Psychodynamic theory: personality Learning theories: conditioning and cognitive Biology of negative emotionality Treatments Chemotherapies (from the beta-blockers to the benzodiazepines, Buspar & antidepressants) Psychotherapies (exposure and beyond)
 Descriptive features BR: OCD and “OCD Spectrum Disorders”")
Anxiety Disorders 4. Obsessive-Compulsive Disorder (OCD) Descriptive features BR: OCD and “OCD Spectrum Disorders” Understanding OCD Psychodynamic and Learning theories Modern cognitive psychology: thought suppression and its vicissitudes Modern neurobiology: monoamines and the caudate nucleus Treatments Chemotherapy and psychotherapy The special case

Anxiety Disorders Anxiety disorders and their comorbidities 1. Among anxiety disorders (e. g. , panic and phobia). 2. Between anxiety and other Axis 1 disorders (e. g. , depression) 3. Between anxiety and Axis II disorders (e. g. , “inhibited” personality disorders)
- Slides: 115