Cerebrovascular accident DR Gheith A Bugaila MD cerebrovascular

Cerebrovascular accident DR. Gheith. A. Bugaila, MD

cerebrovascular accident • stroke is a sudden focal neurological – deficits wich is persisit for more than 24 hrs Transient ischemic attack is asudden focal – neurological deficits which lasting less than 24 hrs

Aetiology Ischemic stroke LARGE VESSEL THROMBOTIC: • Blood vessel injury - HTN, Atherosclerosis, Vasculitis • Stasis/turbulent blood flow - Atherosclerosis, A. fib. , Valve disorders • Hypercoagulable state

LARGE VESSEL EMBOLIC: • The Heart – Valve diseases, A. Fib, Dilated cardiomyopathy, Myxoma • Arterial Circulation – Atherosclerosis of carotid, Arterial dissection, Vasculitis • The Venous Circulation – PFO R to L shunt, Emboli

• Large Vessel: – Look for cortical signs , weakness, hypertonia , hyperreflexia, extensor planter • Small Vessel: – Lacunar • Posterior Circulation: – Crossed signs – Cranial nerve findings • Watershed: – Look for the watershed pattern – Think about reasons of hypo-perfusion • Hypotension • bleeding

• MCA: – Arm>leg weakness – LMCA cognitive: Aphasia – RMCA cognitive: Neglect, apraxia, constructional impairment • ACA: – Leg>arm weakness – Cognitive: , disinhibition • PCA: – Hemianopia – Cognitive: memory loss/confusion, alexia • Cerebellum: – Ipsilateral ataxia, hypotonia

• Broca’s – Expressive aphasia – Left posterior inferior frontal gyrus • Wernicke’s – Receptive aphasia – Posterior part of the superior temporal gyrus – Located on the dominant side (left) of the brain
 • Risk Factors – HTN – HLD –")
SMALL VESSEL (Lacunes <1. 5 cm) • Risk Factors – HTN – HLD – DM – Tobacco Use – Sleep apnea

Brainstem stroke • Usually a combination of cranial nerve abnormalities, and crossed motor/sensory findings such as: – – – – Double vision Facial numbness and/or weakness Slurred speech Difficulty swallowing Ataxia Vertigo Nausea and vomiting Hoarseness

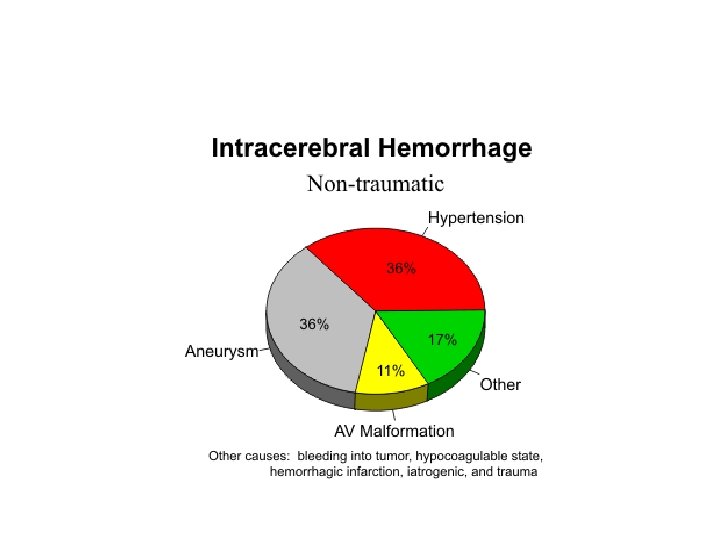
Intracranial Hemorrhages • Aetiology • Traumatic • Spontaneous – Hypertensive – Amyloid angiopathy – Aneurysmal rupture – Arteriovenous malformation rupture – Bleeding into tumor – Cocaine and amphetamine use

• Hypertensive ICH • Spontaneous rupture of a small artery deep in the brain • Typical sites – Basal Ganglia – Cerebellum – Pons

• Ganglionic hge • • • Contralateral hemiparesis Hemisensory loss Homonymous hemianopia Conjugate deviation of eyes toward the side of the bleed (stupor, coma)

• Cerebellar hge • Vomiting (more common in ICH than SAH or Ischemic CVA) • Ataxia • Eye deviation toward the opposite side of the bleed • Small sluggish pupils • Stupor, coma
 Abrupt onset")
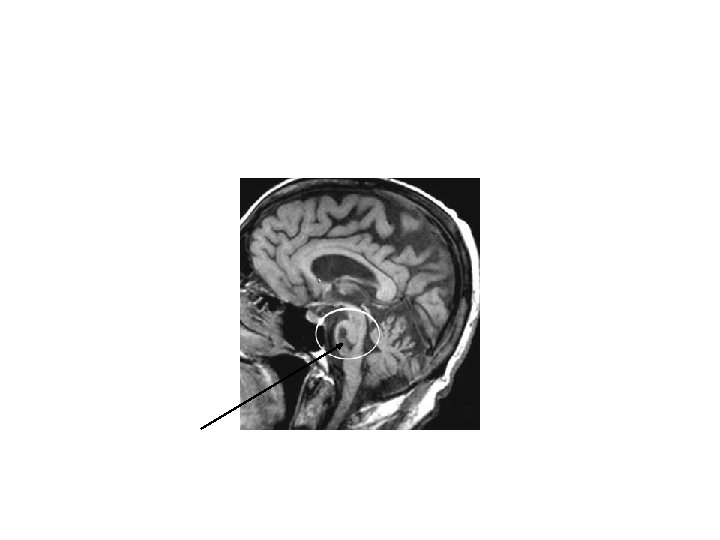
• Pontine hge • • Pin-point but reactive pupils(use magnifing lens) Abrupt onset of coma Decerebrate posturing or flaccidity Ataxic breathing pattern


• • D/D CNS infection CNS neoplasm, SOL Seizure Hypoglycemia Hemiplegic migraine functional

Management • ABCs • Airway • Respiratory rate , pattren of respiration, artificial denture, signs of cyanosis, auscultate for aspiration pneumonia, check ABG, pulse oximetry • Look for decreased level of consciousness (LOC) with daily GCS scoring • GCS < 8 – consider INTUBATION • Avoid Hyperventilation or Hypoventilation • NPO until swallow assessment completed- high aspiration risk, use NGT if needed • Perform generalized neurological examination, do not forget pupil exam and brainstem reflexes, meningeal signs, signs of trauma, stabilize the neck until exclude injury

• BP Management – The goal is to maintain cerebral perfusion!! – Higher BP goals with Ischemic stroke – ONLY treat high blood pressure in ischemic infarction if more than 220/120 – If blood pressure is less than 220/110 do not give antihypertensive drugs for first 2 -3 days, unless thrombolytic therapy is planning – Lower BP goals with Hemorrhagic stroke (avoid hemorrhagic expansion, especially in AVMs and aneurysms) – Keep blood pressure less than or equal 160/100 – Recent studies shows even keep it 140/90 is safe and gives good outcome
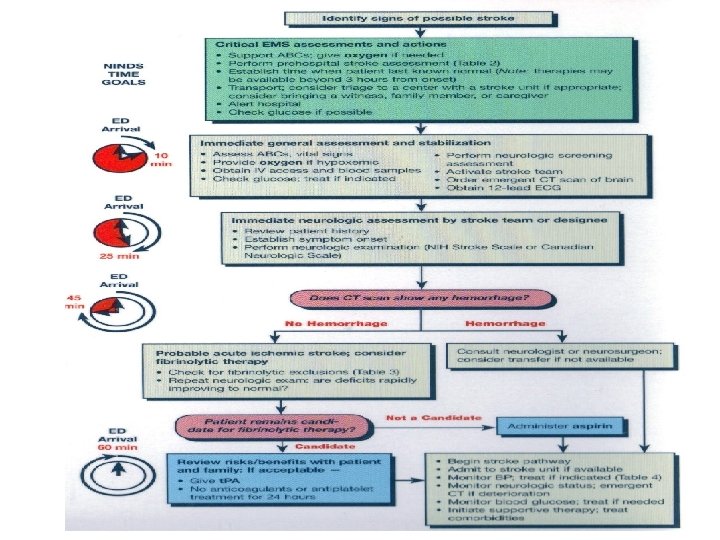

• Imaging CT scan • Non- contrast CT remains the gold standard as it is superior for early detect IVH and ICH • CT with contrast may help identify aneurysms, AVMs, or tumors • MRI • Superior for showing underlying structural lesions, • Also MRA, MRV R/I and coagulation profile, ECG , CXR, LIPID PROFILE, carotid a Doppler
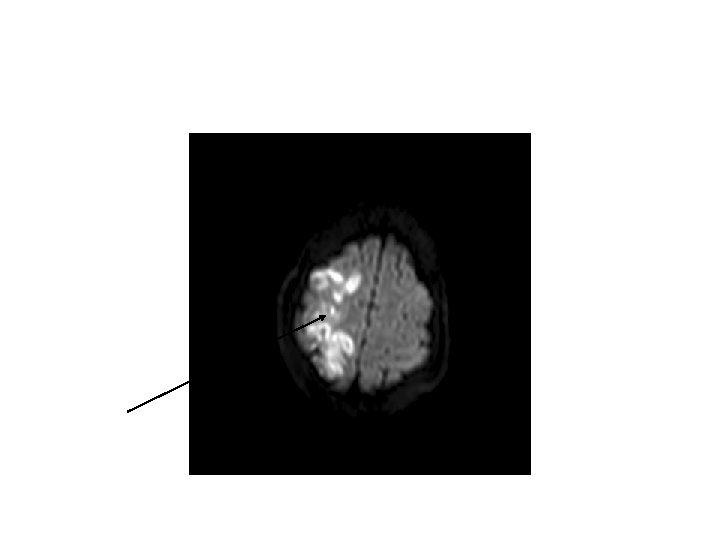
 Infarction R L Subtle blurring of gray-white junction & sulcal effacement")
Acute (4 hours) Infarction R L Subtle blurring of gray-white junction & sulcal effacement Subacute (4 days) Infarction L R Obvious dark changes & “mass effect” (e. g. , ventricle compression)

• THROMBLYTIC THERAPY TPA • • • Tissue plasminogen activator “clot buster” IV tpa window 3 hours IA tpa window 4. 5 hours Disability risk 30% despite ~5% symptomatic ICH risk • C/I • Hemorrhage • SBP > 185 or DBP > 110 • Recent surgery, trauma or stroke • Coagulopathy • Seizure at onset of symptoms • Age? SO IN SUCH CASES WE GIVE ONLY ANTIPLATELETS ASPIRIN , DIPYRIDAMOL, CLOPIDOGRIL

Mechanical Thrombolysis • Often used in adjunct with t. Pa • MERCI (Mechanical Embolus Removal in Cerebral Ischemia) • SUPPORTIVE CARE • Glucose Management – Infarction size and edema increase with acute and chronic hyperglycemia – Hyperglycemia is an independent risk factor for hemorrhage when stroke is treated with t-PA – Recent studies shows no benefit from iv insulin infusion for restrict blood glucose control

• Antiepileptic Drugs – Seizures are common after hemorrhagic CVAs ICH related seizures , a midline shift, and tend to predict poorer outcomes, better to use antiepileptic which not influence the degree of consciousness levetiracetam keepra is recently approved as agood choice Antiedema measures; iv mannitol used to decrease cerebral edema elevate pateint head hyperventilation is controversal ! avoid hypotonic saline DVT prophylaxis with low molecular heparin can be used even in hgic stroke Medical mattress and frequant changing position and skin care for prevent bed sores

• Treat fevers! – Evidence shows that fevers > 37. 5 C that persists for > 24 hrs correlates with ventricular extension and is found in 83% of patients with poor outcomes – If fever due to infection, Treat any evident infections, aspiration pneumonia, bed sores, UTI…

• In hgic stroke • In small hemorrhage treat conservative with control bp and antibrain edema mannitol • In hemorrhage in cerebellum or brainstem and large hemorrhage with midline shift need early neurosugical consultaions and evacuation or burr hole to decrease intracranial pressure to prevent herniation

• 67 yrs man presented with facial asymmetry, rt hemiplegia in early morning while he was sleeping, he is hypertensive BP 150/80, GCS 14/15, laboratory invx all within normal, CT brain shows ischemic infarction , no h/o seizure or recent surgery, • How to manage the pt in ER ? • What is the best treatment ?
- Slides: 30