aminimmums ac ir ASTHMA AND PREGNANCY CASE HISTORY



















 daytime symptoms No limitations of activity No")








 You treat patient's symptom, but")
 You treat your patient's disease,")
 Salbutamol Atrovent Controllers (Mainly anti-inflammatory) Inhaled corticosteroids LABA cromolyn")

 Inhaled corticosteroids")


 >5 y Age <5 y Medium Daily Dose")
 >5 y Age <5 y Medium Daily Dose")
 >5 y Age <5 y Medium Daily Dose")
 >5 y Age <5 y Medium Daily Dose")


 asthma Allergens, especially indoor")





 Allergic rhinitis (AD)")



 Allergen avoidance")












- Slides: 65
aminim@mums. ac. ir ASTHMA AND PREGNANCY
CASE HISTORY
A 20 yr old lady presented with Hx of cough and dyspnea for 6 months 2 weeks of drug discontinuation 1 week cough, sputum and dyspnea She is 3 mo pregnant She is concerned about her chest disease during pregnancy
Is it really asthma? Why me? I had no family history. Does pregnancy cause my asthma to be exacerbated? Can my asthma be cured? Can moisturizers help me to improve? How does asthma affect my fetus? Are asthma drugs risky for my fetus? Is my child more prone to asthma? Can heartburn cause my asthma? Should I get flu shot? What should I do in the case of asthma attack? Can I do NVD for termination of pregnancy?
IS IT REALLY ASTHMA?
Recurrent episodes of wheezing Troublesome cough at night Cough or wheeze after exercise Cough, wheeze or chest tightness after exposure to airborne allergens or pollutants Colds “go to the chest” or take more than 10 days to clear
Pregnancy dyspnea Increased tidal volume Decreased ERV and FRC Intact FEV 1 Less than normal PCo 2 Above normal PO 2 The presence of cough and wheezing suggests asthma
WHY ME?
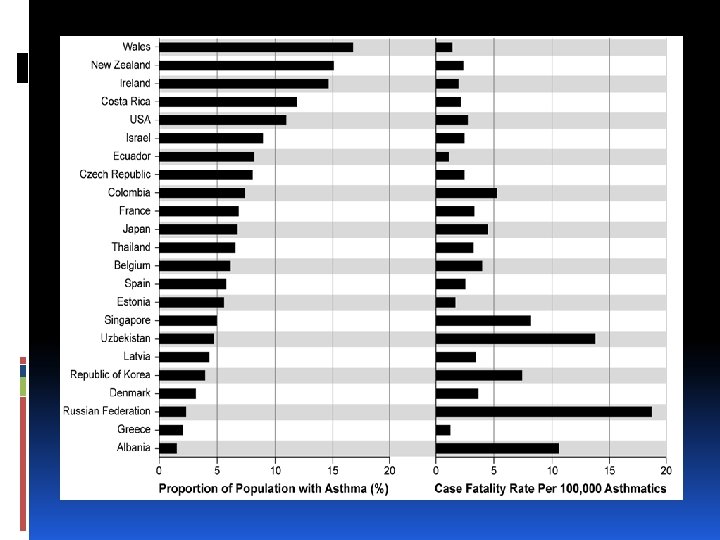
Asthma is a common disease Even more than diabetes mellitus In some countries 1 out of every 4 children has asthma
Asthma affects 4 to 8% of all pregnant women
I HAD NO FAMILY HISTORY
Asthma occurs more commonly in those with atopic history In themselves or Their 1 st degree relatives A person with allergic rhinitis has 5 times more chance of asthma
Asthma is a polygenic disease Asthma occurs in a genetically susceptible person, who exposed to specific etiologic factors It occurs more common in identical twins
DOES PREGNANCY CAUSE MY ASTHMA TO BE EXACERBATED?
Pregnant women have different courses of their asthma 1/3 aggravate 1/3 improve 1/3 does not change
The most common cause of asthma exacerbation Discontinuation of drugs Viral infections Well controlled asthma has favorable outcome in pregnancy
Poor controlled asthma has been associated with 15 to 20 % increase in Preterm delivery Preeclampsia Growth retardation Need for C/S Maternal morbidity Maternal mortality
These risks are increased 30 to 100 % those with more severe asthma Asthma is not associated with risk of congenital malformations
What is “well control”? No (or minimal) daytime symptoms No limitations of activity No nocturnal symptoms No (or minimal) need for rescue medication Normal lung function No exacerbations
In pregnant asthmatics you should confirm control by Spirometry Monthly Peak flow metry Twice daily Upon awakening After 12 hr
FEV 1 < 80% in pregnancy associated with poor pregnancy outcomes moderate to severe asthmatics Serial ultrasound examination Early in pregnancy Regularly after 32 wk After an asthma exacerbation
CAN MY ASTHMA BE CURED?
Asthma is a chronic disease We have very few diseases with such a good response to therapy as asthma Quality of life improved markedly after treatment
ARE ASTHMA DRUGS RISKY FOR MY FETUS?
As asthma is an inflammatory disease limited to lung airways Treatment of this disease in a topical form is More effective Less harmful
You can choose one of these categories for your asthmatic patient Relievers Controllers
If you choose the 1 st one (reliever) You treat patient's symptom, but Relievers do not work on inflammation! Your patient is prone to Asthma attack Airway remodeling
If you choose the 2 nd one (controllers) You treat your patient's disease, and You can control inflammation You reduce the risk of Asthma attack Airway remodeling in your patient
Relievers (No anti-inflammatory action) Salbutamol Atrovent Controllers (Mainly anti-inflammatory) Inhaled corticosteroids LABA cromolyn Theophylline Leukotrene antagonists
When should I start controllers? >3 times/ wk day salbutamol need >3 times/ mo night awakening >3 times/ yr salbutamol prescription >3 times/ yr exacerbation >3 times/ yr short-term corticosteroid
Safety profile of common anti-asthma drugs Drug Safety Salbutamol Safe, inhaler (labor) Inhaled corticosteroids Category B, Budesonide Cromolyn Safe Theophylline Safe (5 -12 mcg/ml) ↓ clearance in 3 rdtrimester Cord blood level the same Load 5 -6 mg/kg Maintenance 0. 5 mg/kg/hr Delayed labor
Drug Safety LABA Not reassuring Adrenaline Not for asthma Systemic steroids Pre-eclampsia, GDM Atroent Leukotrene antagonists Prematurity, LBW Safe Ziluten not assessed Zafirleukast, monteleukast probably safe
Mild intermittent PRN Salbutamol Mild persistent Inhaled corticoteroid Moderate persistent Inhaled corticoteroid + LABA Severe persistent Inhaled corticoteroid + LABA
Drug Low Daily Dose ( g) >5 y Age <5 y Medium Daily Dose ( g) >5 y Age <5 y Beclomethasone 200 -500 100 -200 >500 -1000 >200 -400 Budesonide 200 -600 100 -200 600 -1000 >200 -400 Budesonide-Neb Inhalation Suspension Ciclesonide 250 -500 80 – 160 High Daily Dose ( g) >5 y Age >1000 >500 -1000 <5 y >400 >1000 80 -160 >160 -320 >320 -1280 >320 Flunisolide 500 -1000 500 -750 >1000 -2000 >750 -1250 >2000 >1250 Fluticasone 100 -250 100 -200 >250 -500 >200 -500 >500 Mometasone furoate 200 -400 100 -200 > 400 -800 >200 -400 >800 -1200 Triamcinolone acetonide 400 -1000 400 -800 >1000 -2000 >800 -1200 >2000 >400 >1200
Drug Low Daily Dose ( g) >5 y Age <5 y Medium Daily Dose ( g) >5 y Age <5 y Beclomethasone 200 -500 100 -200 >500 -1000 >200 -400 Budesonide 200 -600 100 -200 600 -1000 >200 -400 Budesonide-Neb Inhalation Suspension Ciclesonide 250 -500 80 – 160 High Daily Dose ( g) >5 y Age >1000 >500 -1000 <5 y >400 >1000 80 -160 >160 -320 >320 -1280 >320 Flunisolide 500 -1000 500 -750 >1000 -2000 >750 -1250 >2000 >1250 Fluticasone 100 -250 100 -200 >250 -500 >200 -500 >500 Mometasone furoate 200 -400 100 -200 > 400 -800 >200 -400 >800 -1200 Triamcinolone acetonide 400 -1000 400 -800 >1000 -2000 >800 -1200 >2000 >400 >1200
Drug Low Daily Dose ( g) >5 y Age <5 y Medium Daily Dose ( g) >5 y Age <5 y Beclomethasone 200 -500 100 -200 >500 -1000 >200 -400 Budesonide 200 -600 100 -200 600 -1000 >200 -400 Budesonide-Neb Inhalation Suspension Ciclesonide 250 -500 80 – 160 High Daily Dose ( g) >5 y Age >1000 >500 -1000 <5 y >400 >1000 80 -160 >160 -320 >320 -1280 >320 Flunisolide 500 -1000 500 -750 >1000 -2000 >750 -1250 >2000 >1250 Fluticasone 100 -250 100 -200 >250 -500 >200 -500 >500 Mometasone furoate 200 -400 100 -200 > 400 -800 >200 -400 >800 -1200 Triamcinolone acetonide 400 -1000 400 -800 >1000 -2000 >800 -1200 >2000 >400 >1200
Drug Low Daily Dose ( g) >5 y Age <5 y Medium Daily Dose ( g) >5 y Age <5 y Beclomethasone 200 -500 100 -200 >500 -1000 >200 -400 Budesonide 200 -600 100 -200 600 -1000 >200 -400 Budesonide-Neb Inhalation Suspension Ciclesonide 250 -500 80 – 160 High Daily Dose ( g) >5 y Age >1000 >500 -1000 <5 y >400 >1000 80 -160 >160 -320 >320 -1280 >320 Flunisolide 500 -1000 500 -750 >1000 -2000 >750 -1250 >2000 >1250 Fluticasone 100 -250 100 -200 >250 -500 >200 -500 >500 Mometasone furoate 200 -400 100 -200 > 400 -800 >200 -400 >800 -1200 Triamcinolone acetonide 400 -1000 400 -800 >1000 -2000 >800 -1200 >2000 >400 >1200
Choice of drug categories in pregnancy Category Drug of choice SABA Salbutamol LABA Salmetrol ICS Budesonide
CAN MOISTURIZERS HELP ME TO IMPROVE?
About 80 % of asthma patients have allergic (extrinsic) asthma Allergens, especially indoor allergens Mites Fungi Can cause asthma or allergic rhinitis to become worse Room humidity of > 50% speed up growth of mites and fungi
Avoidance from allergens, irritants and air pollution Is necessary for any asthmatic pregnant woman
Allergen immunotherapy can be continued during pregnancy But, should not be started for the 1 st time in a pregnant woman
IS MY CHILD MORE PRONE TO ASTHMA?
There is no association to mother asthma during fetal period and development of asthma in childhood period. Albeit asthma is a genetic disease
CAN HEARTBURN CAUSE MY ASTHMA?
Comorbid conditions in asthma Gastro-esophageal reflux disease (GERD) Allergic rhinitis (AD)
Be suspicious to GERD if Your asthmatic patient become poorly controllable Your asthmatic patient is worse at night Your asthmatic patient has symptoms when lies down Patient complains of GERD symptoms
Treatment of heartburn can improve asthma symptoms Continue anti GERD drugs for at least 2 -3 months
Be suspicious to AD if Your asthmatic patient complains of seasonal nose or sinus symptoms
Treat AD with Intranasal corticosteroids Antihistamines (2 nd generation in pregnancy) Allergen avoidance
SHOULD I GET FLU SHOT?
Influenza vaccination is necessary for Pregnant women with 2 nd and 3 rd trimester In cold months
WHAT SHOULD I DO IN THE CASE OF ASTHMA ATTACK?
Treatment of asthma attack is the same as non-pregnant woman Aggressive monitoring of mother and fetus Oxygen 3 -4 l/min by cannula Goal of Po 2 > 70 Sat > 95
Pco 2 > 35 mm. Hg Po 2 < 70 mm Hg Are abnormal during pregnancy IV fluid (dextrose) initially 100 ml/hour Seated position Fetal monitoring
Dosage of glucocorticoids is not different IV aminophylline NOT generally recommended IV Mg sulfate may be beneficial Concomitant hypertension Preterm contraction
Respiratory infections in asthmatic patients Usually viral If indicated in a pregnant woman I V Ceftriaxone Erythromycin
LABOR: C/S OR NVD?
No difference PG F 2 analogues should not be used in asthmatics for termination of pregnancy Morphine and meperidine should be avoided Fentanyl is an appropriate alternative
In the case of emergency cesarean section Epidural anesthesia is the favoured anesthesia Decreses O 2 consumption and minute ventilation If general anesthesia required Ketamine is preferred Ergot derivatives for pertiprtum bleeding, headache, should be avoided
Summary Careful assessment and monitoring Avoidance and controll of triggers Maintenance rather than symptomatic therapy Aggressive treatment of exacerbations
THANK YOU