ASTHMA Definition of asthma 2 Definition The guidelines




















")













 • High Rate Of Persistence")


 It is not definitely known which")

")




















")

")
 including: – insects and insect")

")















 and asthma commonly occur together")









: 839 -44")












")






 > Men childhood asthma")






- Slides: 119
ASTHMA
Definition of asthma 2
Definition The guidelines define asthma as: a chronic inflammatory disease of the airways many cells play a role (mast cells, eosinophils, and T lymphocytes)
Definition recurrent episodes of: • Wheezing • Breathlessness • chest tightness • Cough particularly at night and/or in the early morning
Definition widespread but variable airflow limitation at least partially reversible either spontaneously or with treatment
Definition increase in airway hyperresponsiveness to a variety of stimuli
Definition • Chronic Inflammation • Bronchial Hyperresponsivenes s • Reversible Airway Obstruction
Pathophysiologic Mechanism 8
Pathophysiologic Mechanism • Asthma is caused by a complex interaction of: – cells – Mediators and cytokines • that results in inflammation
Pathophysiologic Mechanism Inflammatory cells mediators Effects pathophysiolo gic changes
pathophysiologic changes
1 -airway smooth-muscle contraction
2 -microvascular leakage
3 -activation of airway neurons
4 -stimulation of mucus-secreting cells
5 -disruption of the ciliated epithelium
airway remodeling • fixed airway narrowing in patients with severe asthma • The airway epithelium becomes an important source of mediators, growth factors, and chemokines
Thickening of the reticular basement membrane • increased release of fibroproliferative and fibrogenic growth factors • deposition of type III and V collagen and fibronectin beneath the basement membrane
increased bronchial smooth-muscle mass
Mucus gland hyperplasia
increased levels of vascular endothelial growth factor (angiogenesis)
Physiologic Mechanisms • Neurogenic Influences • BHR • Airway Obstruction
Physiologic Mechanisms Neurogenic Influences There is growing evidence that the neural control of the airways is abnormal in patients with asthma
Physiologic Mechanisms Neurogenic Influences autonomic dysfunction is a secondary defect caused by inflammation inflammatory mediators can modulate the release of neurotransmitters from airway nerves
Physiologic Mechanisms Neurogenic Influences The autonomic nervous system regulates many aspects of airway function, such as: • airway tone • airway secretions • blood flow • microvascular permeability • and the release of inflammatory cells
Physiologic Mechanisms BHR an exaggerated bronchoconstrictive response by the airways to a variety of stimuli such as aeroallergens, histamine, methacholine, cold air, and environmental irritants
Physiologic Mechanisms BHR Airway inflammation is thought to be a factor in producing BHR, which is a cardinal feature of asthma
Physiologic Mechanisms BHR It is not clear whether bronchial hyperreactivity is acquired or is present at birth and genetically
Physiologic Mechanisms Airway Obstruction Causes of Airflow Limitation in Asthma • Acute bronchoconstriction • Mucus plugging of airways • Bronchial wall edema • Inflammatory cell infiltration • Airway wall remodeling (fibrosis) • Smooth-muscle hypertrophy • Uncoupling of elastic recoil forces
Atopic Asthma non-atopic Asthma
Atopic Asthma Is more common than non-atopic Asthma
Atopic Asthma • extrinsic asthma • asthma that is triggered by exposure to inhaled aeroallergens Nonatopic Asthma • intrinsic asthma • unidentified antigen “self-antigens”
Atopic Asthma Nonatopic Asthma • features of atopy including: – positive family history of allergy and asthma – positive immediate hypersensitivity reactions to skin-prick tests after exposure to a variety of aeroallergens – an increased serum Ig. E leve and blood eosinophilia – Evidence of atopy, such as eczema and hay fever • patients who have NONE of the typical features of atopy
Atopic Asthma • The prevalence of atopy increases throughout childhood and adolescence and peaks in the second decade of life Nonatopic Asthma • Usually, such patients are older than atopic asthmatic patients and have a later onset of asthma
Atopic Asthma Nonatopic Asthma In children • (School Aged) • High Rate Of Persistence Into Adulthood (Preschool Children) • Improve or Resolve in a few years •
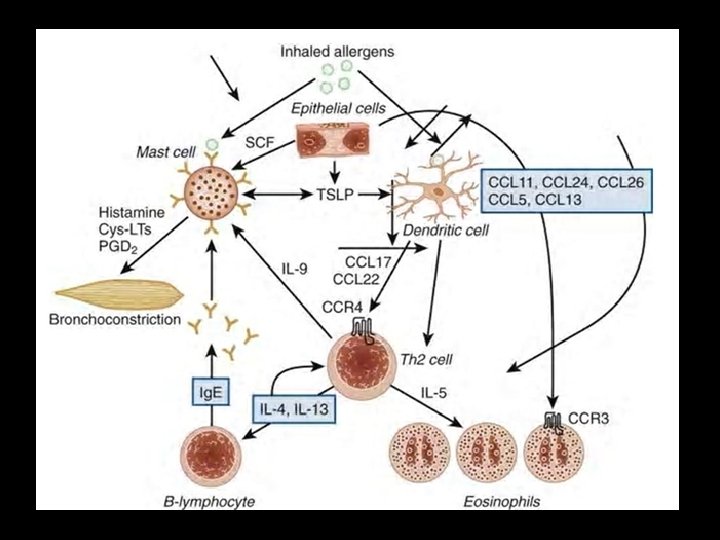
Atopic Asthma type 1 hypersensitivity reaction Ig. E-mediated inflammatory response
Allergen excessive response caused by large amounts of antigen (environmental allergens such as dust mites, animal proteins, pollens, and fungi)
Allergen Antigen presenting cell antigen presenting cells (APCs) It is not definitely known which cells are the APCs
Allergen Antigen presenting cell antigen penetrates beneath the mucosa and enters the lymphatic system
Allergen Th 2 cell Antigen presenting cell lymphocyte activation (Activation of Th 2 -cells) (CD 4+/CD 25+ state)
Allergen IL-4 IL-13 Th 2 cell IL-5 Antigen presenting cell TH 2 release of specific ILs and cytokines responsible for episodic and chronic allergic reactions
Ig. E B cell Allergen IL-4 IL-13 Th 2 cell IL-5 Antigen presenting cell IL-4 enhances the synthesis of Ig. Es by antigen stimulated B lymphocytes (plasma cells)
Ig. E Fce. RI B cell Allergen Mast cell IL-4 IL-13 Th 2 cell Histamine Leukotrienes Prostaglandins Cytokines Atopic disease IL-5 Antigen presenting cell Ig. E binding to receptors on mast cells mast cell activation and the release of inflammatory mediators
Ig. E Fce. RI Immediate Phase B cell Allergen Mast cell IL-4 IL-13 Th 2 cell 15 – 30 min Histamine Leukotrienes Prostaglandins Cytokines IL-5 Antigen presenting cell acute allergic response Atopic disease
Ig. E Fce. RI Immediate Phase B cell Allergen Mast cell IL-4 IL-13 Th 2 cell Antigen presenting cell 15 – 30 min Histamine Leukotrienes Prostaglandins Cytokines Atopic disease IL-5 Eosinophil IL-5 plays an important role in the recruitment of eosinophils to the site of inflammation
Ig. E Fce. RI Immediate Phase B cell Allergen Mast cell IL-4 IL-13 Th 2 cell Antigen presenting cell 15 – 30 min Histamine Leukotrienes Prostaglandins Cytokines Atopic disease 6 – 8 hours IL-5 Delayed Phase Eosinophil the eosinophil releases mediators with a range of tissue-destructive effects
Nonatopic Asthma There is a more intense inflammatory cell infiltrate in the bronchial mucosa macrophages, and CD 3 and CD 4 cells
Risk Factors for Asthma
1. Genetics of Asthma • Although it is generally agreed that there is a major hereditary contribution to the etiology of asthma • the inheritance patterns are complex, and asthma cannot be simply classified as having an autosomaldominant, autosomalrecessive, or sex-linked mode of inheritance
1. Genetics of Asthma • However, genetic studies have discovered multiple chromosomal regions that may contain genes that contribute to asthma
1. Genetics of Asthma • Chromosomes 2 q, 3 p, 5 q, 6 p, 12 q, 13 q, 19 q, and 21 q are likely to contain genes for allergy and asthma
1. Genetics of Asthma • One mutation (the substitution of glycine for arginine at position 16) was associated with more severe asthma and especially with more severe nocturnal symptoms
1. Genetics of Asthma • Another mutant at position 27 renders the receptor more resistant to βagonist and has been associated with less intense BHR in patients with asthma
1. Genetics of Asthma • IL 4 RA gene have been associated with severe exacerbations and poor lung function
1. Genetics of Asthma • the ADAM 33 gene is associated with an accelerated decrease in lung function
2. Sex and Race > Before Puberty 6 versus 3. 7 percent = After Puberty • Childhood asthma is more prevalent in boys, but this prevalence is reversed in puberty and adulthood
2. Sex and Race • The overall prevalence, therefore, is greater in female individuals
2. Sex and Race • Black race/ethnicity is associated with a greater risk of asthma death, independent of socioeconomic status and education
2. Sex and Race • The greater incidence of asthma that has been observed with urbanization suggests that environmental factors may be as important as genetic and racial factors
3. Environmental Factors • Allergens and occupational factors are considered to be the most important causes of asthma
Indoor allergens • animal allergens (eg, cats, dogs, and rodents)
Indoor allergens • cockroach allergen
Indoor allergens Aspergillus Alternaria and Cladosporium • fungi (Alternaria, Aspergillus, Cladosporium, and Candida sp)
Indoor allergens House dust (several organic and inorganic compounds) including: – insects and insect feces – Mold – Pollen – Fibers – mites
Social Factors 66
Outdoor allergens • Outdoor allergens include: – pollens (mainly from trees, weeds, and grasses) – Fungi – Molds – and yeasts
4. Air Pollution • Both outdoor and indoor pollutants contribute to worsening asthma symptoms by triggering bronchoconstriction, increasing BHR, and enhancing responses to inhaled aeroallergens
4. Air Pollution Sulfur Dioxide • outdoor pollutants – industrial smog (sulfur dioxide particulate complex) – photochemical smog (ozone and nitrogen oxides) Ozone (O 3)
4. Air Pollution • indoor air pollution – Modern construction techniques have been suspected of causing greater indoor air pollution – there is 50% less turnover of fresh air
4. Air Pollution • Indoor pollutants include: – – – cooking heating fuel exhausts insulating products Paints and varnishes that contain formaldehyde and isocyanates
4. Air Pollution • Smoking and exposure to environmental Tobacco: – Active smoking – Secondhand smoke – Prenatal exposure to maternal smoking
4. Air Pollution • The effect of cleaning solutions and sprays in the home
5. Respiratory Infections • It has been established that viral respiratory infections are common precipitators of asthma
5. Respiratory Infections § Viral and bacterial respiratory infections are triggers that can cause exacerbations in children and adults with asthma
5. Respiratory Infections • There are strong data to suggest that some of the atypical bacteria, such as Chlamydia pneumoniae and Mycoplasma pneumoniae, also may be involved
5. Respiratory Infections • Therapy with the macrolide antibiotic clarithromycin improved lung function and decreased tissue expression of IL-5
5. Respiratory Infections • This finding suggests that antibiotic use in some patients with persistent asthma may help to control the disease
5. Respiratory Infections § The frequent respiratory infection during infancy may protect against the later development of – Asthma – Hay fever – Eczema
6. atopy / Allergic Rhinitis 1. Allergic Rhino Sinusitis 2. Atopic Dermatitis 3. Allergic conjunctivitis
Percentage patients with comorbidity Allergic rhinitis is often accompanied by comorbidities
6. atopy / Allergic Rhinitis • Nasal and sinus diseases are common comorbidities in patients with asthma
6. atopy / Allergic Rhinitis • Allergic rhinitis (AR) and asthma commonly occur together • > 40% of children with AR have asthma • the presence of AR in a child < 7 years of age predicts future asthma
6. atopy / Allergic Rhinitis • smokers with AR have a threefold increased risk for developing asthma
6. atopy / Allergic Rhinitis • patients with AR, despite the paucity of pulmonary symptoms, have abnormal lung function • And when tested with methacholine or histamine, demonstrate BHR
Other Factors
Stress
Obesity • underweight and being overweight are both associated with an increased risk of the development of asthma
Obesity • Increased BMI may also be associated with increased asthma severity
Obesity • There is some evidence that weight loss in obese asthmatic patients is associated with improved symptoms and lung function, especially PEFR variability
Family history • Children with one asthmatic parent are 2. 6 times more likely to have asthma
Family history • Children with two asthmatic parents, the odds ratio rises to 5. 2
Family history • Mama > Baba Clin Exp Allergy. 2004 Jun; 34(6): 839 -44
The presence of positive skin test results in infants of allergic parents correlates with: the onset of asthma in later childhood the number of positive skin test results shows a correlation with: the severity of asthma
Studies indicate a reverse relationship between family size and asthma This finding suggest that the exposure of young children to older children at home or to children at day-care centers protects against the development of asthma
Medication Use • Use of paracetamol in the first year of life was associated with a small increase in risk of asthma at age 6 to 7
Medication Use • mothers taking regular acetaminophen during pregnancy
Medication Use • Exposure to antibiotics during infancy has been associated with the development of asthma in later childhood • The “microflora hypothesis”
Pre- and Perinatal Factors v Maternal age • Infant mortality due to respiratory illnesses is inversely related to maternal age • children born to mothers younger than 20 years had the highest risk of developing asthma
Pre- and Perinatal Factors v Maternal diet during pregnancy • maternal diet in pregnancy, in particular intakes of the antioxidant vitamin E and zinc, may modulate the risk for wheezing and asthma in young children Vit etam c a r pa E ol Ant ibio Zin tics c
Pre- and Perinatal Factors v Breastfeeding • • Breastfeeding was associated with a decreased risk of wheeze in the first two years of life by age six this effect was not significant
Pre- and Perinatal Factors v Breastfeeding • in the subset of children with atopy and an asthmatic mother, breastfeeding was associated with an increased risk of asthma
Pre- and Perinatal Factors v Breastfeeding • we encourage this approach for at least 4 to 6 months following delivery, regardless of the child's risk of atopy or the presence of maternal asthma
Pre- and Perinatal Factors v Prematurity • Prematurity was a significant risk factor for both recurrent wheezy bronchitis and asthma
Pre- and Perinatal Factors v Mode of delivery • Delivery by Cesarean section may increase the risk of childhood asthma compared with vaginal delivery
"The Hygiene Hypothesis” • The microbial exposure and infections during early childhood (ie, postnatally) protect against the development of asthma and other allergic disease
Pre- and Perinatal Factors v Head circumference at birth
The Natural History of Asthma
childhood The peak prevalence of asthma 10% of the population adolescence and early adulthood This rate decreases 5 to 6% later adulthood The prevalence increases again 7 to 9%
30 to 50% of children with asthma during childhood will outgrow it by early adulthood more likely in male patients than in female patients
The following three features of childhood asthma may predict those who are more likely to have persistent symptoms into adulthood: severe atopy determined by skin testing a marked degree of bronchial reactivity and difficult-tocontrol asthma
In adulthood there is a steady incidence of new-onset asthma through patients of all ages, even in elderly patients
22 years New onset Women (Twice) > Men childhood asthma
65 years New onset Women = Men 4 -8%
In adulthood Many patients begin with recurrent wheezing after respiratory viral infections This pattern may gradually or abruptly develop into persistent wheezing and often severe, poorly responsive disease
In adulthood remission is much less common in older age groups although it still may be as high as 20 to 30% • severe symptoms • reduced ventilatory function • and a concomitant diagnosis of COPD
In adulthood Asthma may also result from exposure to occupational hazards Remission usually occurs when the patient is removed from the offending environment, but unfortunately, this is not always the case
1. Triggers