Asthma Dr Gerrard Uy Asthma Asthma is a












 – Measurements are made using")






 – Long acting")




 Dr. Gerrard Uy")

 • a disease state")


 – most")















- Slides: 48
Asthma Dr. Gerrard Uy
Asthma • Asthma is a serious health problem throughout the world, affecting people of all ages • When uncontrolled, asthma can place severe limits on daily life, and is sometimes fatal • In 1993, GINA was introduced
What is Asthma • Chronic inflammatory disorder of the airways • Associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, coughing, particularly at night or early in the morning • Clinical manifestations can be controlled with appropriate treatment
What is Asthma • Wheezing is the most common physical finding in asthma • Main physiological feature is episodic airway obstruction characterized by expiratory airflow limitation • Dominant pathological feature is airway inflammation, sometimes associated with structural changes • Strongly associated with atopy
Burden of Asthma • Asthma is a problem worldwide with an estimated 300 million affected individuals • Ranges for 1 – 18% of the population in different countries • Annual worldwide deaths from asthma have been estimated at 250, 000
Factors influencing the development and expression of asthma • Host Factors: – Genetics – Obesity (BMI > 30 kg/m 2) – Sex • Environmental Factors: – Allergens – Infections – Occupational sensitizers – Tobacco smoke – Outdoor/Indoor pollution – Diet
Mechanism of asthma • Airway inflammation – Remains to be a consistent feature – Persistent even though symptoms are episodic – Inflammation affects all airways but is most pronounced in medium sized bronchi – Inflammatory cells found in asthma • • • Mast cells Eosinophils T lymphocytes Dendritic cells Macrophages Neutrophils
Mechanism of asthma • Airway structural cells involved in asthma: – Airway epithelial cells – Airway smooth muscle cells – Endothelial cells – Fibroblast and myofibroblast – Airway nerves
Mechanism of asthma • Structural changes in asthma – Subepithelial fibrosis – Airway smooth muscle hypertrophy and hyperplasia – Blood vessels increase in number – Mucus hypersecretion
Pathophysiology • Airway narrowing is the common final pathway leading to symptoms and physiological changes in asthma • Airway hyperresponsiveness is the characteristic functional abnormality in asthma
Diagnosis • Episodic breathlessness, wheezing, cough, and chest tightness • History of atopy or allergic rhinitis • Symptoms occurring at night • Precipitation by exposure to certain allergens • Resolves/improves after appropriate asthma medication
Lung Function Test • Spirometry – Recommended method of measuring airflow limitation and reversibility – Measures FEV 1 and FVC – FEV 1/FVC is normally > 0. 75 – 0. 80 – The degree of reversibility in FEV 1 is generally accepted as 12% or 200 ml from the pre bronchodilator value
Lung Function Test • Peak Expiratory Flow Measurement (PEF) – Measurements are made using a peak flow meter – Relatively inexpensive, portable, ideal for patients in home settings – PEF can underestimate degree of airflow limitation – Most commonly, PEF is measured first thing in the morning before treatment is taken – 60 ml/L or 20% improvement from prebronchodilator suggests a diagnosis of asthma
Differential Diagnosis • Children 5 yrs and younger – Transient early wheezing – Persistent early onset wheezing – Late onset wheezing/asthma • Older children and adults – Hyperventilation syndrome – Foreign body aspiration – Vocal cord dysfunction – COPD – heartfailure
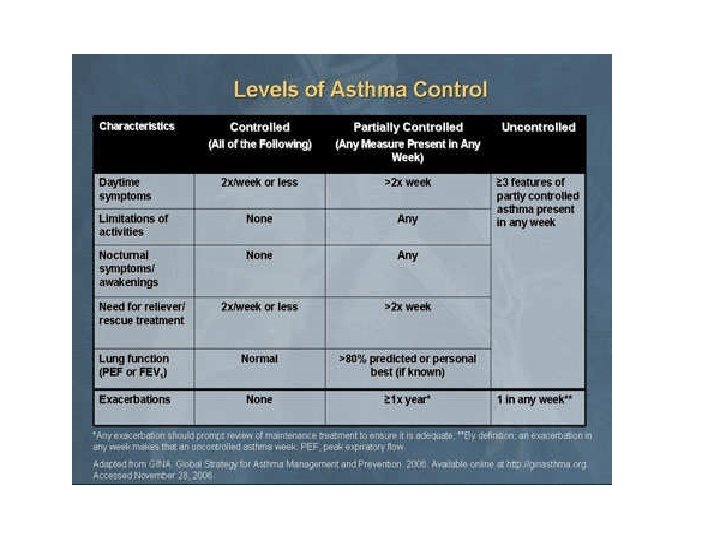
Treatment • The goal of asthma treatment is to achieve and maintain clinical control • Medications to treat asthma is divided into 2 – Controllers and relievers • Different routes of administration: – Inhaled, orally, parenterally (IV, SC, IM) – The major advantage of inhaled route is that the medication is delivered directly into the airways, producing higher local concentrations with less risk of systemic side effects
Controller Medications • Inhaled glucocorticoids – Currently the most effective anti-inflammatory medication for the treatment of persistent asthma – Budesonides, fluticasone, mometasone, etc. – To reach clinical control, add on therapy with another class of drug is preferred over increasing the dose of inhaled glucocorticoids – Side effects: • Oropharyngeal candidiasis • Dysphonia • Coughing from upper airway irritation
Controller Medications • Inhaled glucocorticoids – Systemic side effects of long term high dose glucocorticiods: • • • Easy bruising Adrenal suppression Decreased bone mineral density Cataracts/glaucoma *there is no evidence that the use of inhaled glucocorticoids increases the risk of pulmonary infections
Controller Medications • Leukotriene modifiers – Small and variable bronchodilator effect – Maybe used as an alternative treatment for patients with mild persistent asthma – Usually used as an add on therapy – Less effective compared to long acting B 2 agonist as an add on therapy – Montelukast, zileuton, etc
Controller Medications • Long acting inhaled B 2 agonist – Should not be used as monotherapy because they do not influence airway inflammation – Salmeterol, Formoterol, etc – Side effects: • Cardiovascular stimulation • Skeletal muscle tremor • hypokalemia
Controller Medications • Others: – Theophylline – Cromones (Sodium cromoglycate/Nedocromil Na) – Long acting oral B 2 agonist (Salbutamol, bambuterol, terbutaline) – Anti Ig. E (Omalizumab) – Systemic glucocorticoids
Reliever Medications • Rapid acting inhaled B 2 agonist – Medication of choice for relief of bronchospasm during acute exacerbations of asthma and for pretreatment of exercise induced bronchoconstriction – Salbutamol, formoterol, terbutaline, etc – Side effects: tremor and tachycardia
Reliever Medications • Systemic glucocorticoids – Important in the treatment of severe acute attacks – Prevent progression of the exacerbation, reduce the need for referral to emergency departments and hospitalization, reduce morbidity of the illness – Main effect are only evident after 4 -6 hrs – Prednisone, hydrocortisone, etc
Reliever Medications • Anti-cholinergics – Alternative bronchodilator in patients who experience side effects of B 2 agonist – Side effect: dryness of the mouth and bitter taste – Ipatropium bromide
Reliever Medications • Others – Theophylline – Rapid acting B 2 agonist – Alternative medicine
COPD (Chronic Obstructive Pulmonary Disease) Dr. Gerrard Uy
COPD • Major cause of chronic morbidity and mortality throughout the world • GOLD was created to increase awareness of COPD among health professionals, public health authorities, and the general public, and to improve prevention and management through a concerted worldwide effort
COPD • Global Initiative for Chronic Obstructive Lung Disease (GOLD) • a disease state characterized by airflow limitation that is not fully reversible • The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles and gases – Includes: • emphysema, chronic bronchitis, and small airways disease
COPD • Emphysema – an anatomically defined condition characterized by destruction and enlargement of the lung alveoli • Chronic Bronchitis – a clinically defined condition with chronic cough and phlegm • Small airways disease – a condition in which small bronchioles are narrowed
Symptoms of COPD • Cough • Sputum production • Dyspnea on exertion * chronic cough and sputum production often precede the development of airflow limitation by many years
Risk Factors • Cigarette/tobacco Smoking – Intensity: pack years (sticks/day for years) – most highly significant predictor of FEV 1 • Occupational Exposures – general exposure to dust at work – coal mining, gold mining, and cotton textile dust
Risk Factors • Indoor Air pollution – Biomass fuel used for cooking • Outdoor Air Pollution • Genetic Considerations (alpha 1 antitrypsin deficiency)
Natural History • Effect of cigarette smoking depends on intensity, timing during growth, basal function
Pathophysiology • Airflow obstruction – Determined by spirometry: FEV 1 and FVC – chronically reduced ratio of FEV 1/FVC – seldom shows large responses to inhaled bronchodilators • Hyperinflation – "air trapping“ – helps to compensate for airway obstruction
Pathophysiology • Gas Exchange – Nonuniform ventilation and ventilation-perfusion mismatching
Pathology • Large Airway – Cigarette smoking often results in mucous gland enlargement and goblet cell hyperplasia – proportional to cough and mucus production • Small Airways • major site of increased resistance in most individuals with COPD is in airways 2 mm diameter • goblet cell metaplasia and replacement of surfactantsecreting Clara cells with mucus-secreting and infiltrating mononuclear inflammatory cells
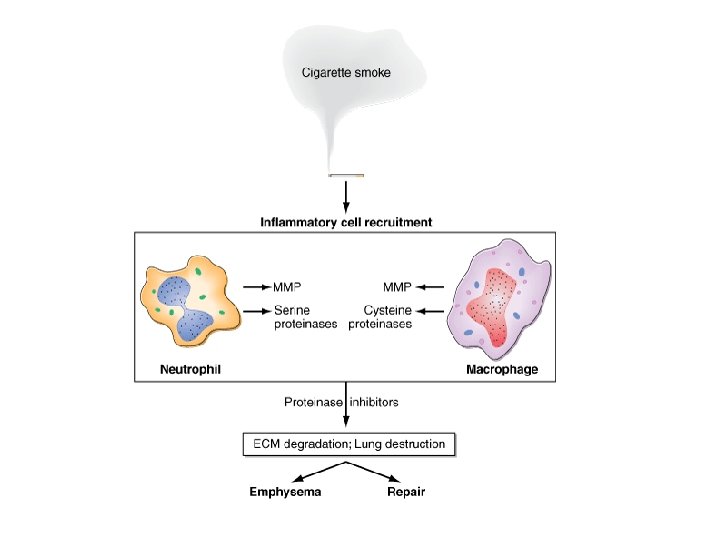
Pathology • Lung Parenchyma – destruction of gas-exchanging airspaces – walls become perforated and later obliterated with coalescence of small distinct airspaces into abnormal and much larger airspaces – Macrophages accumulate – Centriacinar emphysema- most frequently associated with cigarette smoking – Panacinar emphysema - usually observed in patients with alpha 1 AT deficiency
Diagnosing COPD • Considered in any patient who has dyspnea, chronic cough with or without sputum production and/or history of exposure to risk factors for the disease • Preform spirometry for confirmation
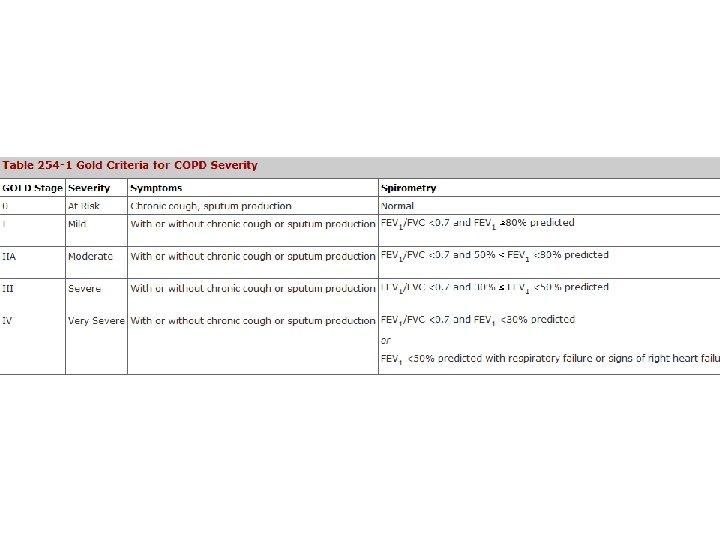
Stages of COPD • Stage 1: Mild COPD – Mild airflow limitation (FEV 1/FVC <70%, FEV 1 > 80% predicted) • Stage 2: Moderate COPD – Worsening airflow limitation (FEV!/FVC <70%, FEV 1 < 80% predicted) • Stage 3: Severe COPD – Further worsening (FEV 1/FVC <70%, FEV 1 < 50% predicted) • Stage 4: Very severe COPD – FEV 1/FVC <70%, FEV 1 < 30% predicted or < 50% with chronic respiratory failure
Clinical presentation • History • cough, sputum production, and exertional dyspnea • exertional dyspnea, often described as increased effort to breathe, heaviness, air hunger, or gasping, can be insidious • patient's ability to perform them has changed
Clinical presentation • Physical Findings – entirely normal physical examination – early – signs of active smoking, including an odor of smoke or nicotine staining of fingernails – prolonged expiratory phase and expiratory wheezing- more severe – signs of hyperinflation include a barrel chest and enlarged lung volumes
Laboratory Findings • hallmark of COPD is airflow obstruction • Pulmonary function testing shows airflow obstruction with a reduction in FEV 1 and FEV 1/FVC • lung volumes may increase
COPD Management • Goals: – Relieve symptoms – Prevent disease progression – Improve exercise tolerance – Improve health status – Prevent and treat complication – Prevent and treat exacerbations – Reduce mortality – Prevent or minimize side effects from treatment
COPD Management • In addition to spirometry, other test maybe considered for the assessment of stage 2 – 4 COPD – Bronchodilator reversibility testing • To rule out a diagnosis of asthma – Chest xray – Abg • Performed in patients with FEV 1 <50% – Alpha 1 antitrypsin deficiency • Performed in patients of caucasian descent under 45 y. o. with a strong family hx of COPD
Treatment • • SMOKING cessation Bronchodilators Anticholinergic agents Beta agonists Inhaled Glucocorticoids Oral Glucocorticoids Theophylline Oxygen
Treatment • • General Medical Care Pulmonary Rehabilitation Lung Volume Reduction Surgery Lung Transplantation