ERS Webinar COVID19 potential impact on asthma patients

ERS Webinar COVID-19: potential impact on asthma patients Prof Dr Guy BRUSSELLE Prof Dr Antonio SPANEVELLO Stephanie AYRE World Asthma Day, 05/05/2020

COVID-19 and asthma: take home messages Well-controlled asthma is not associated with an increased risk of (severe) COVID-19. Use of inhaled corticosteroids (ICS) in subjects with asthma prevents exacerbations, is associated with reduced expression of ACE 2 in sputum, and should be continued during the COVID pandemic. Smoking increases the risk of severe COVID-19, and is associated with increased expression of ACE 2 in airways and lungs. The COVID-19 pandemic impacts (severe) asthma care. Antiviral drugs and immunomodulatory treatments need to be tested in randomized controlled trials (RCT).

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

Conflict of interest disclosure: Guy Brusselle I have no real or perceived conflicts of interest that relate to this presentation. X I have the following real or perceived conflicts of interest that relate to this presentation: Affiliation / Financial interest Commercial Company Grants/research/speaker support Astra. Zeneca, Boehringer-Ingelheim, Chiesi, Glaxo. Smith. Kline, Novartis and Teva Honoraria or consultation fees: Astra. Zeneca, Boehringer-Ingelheim, Glaxo. Smith. Kline, Novartis, Sanofi/Regeneron and Teva Participation in a company sponsored NONE bureau: Stock shareholder: NONE Spouse / partner: NONE Other support / potential conflict of interest: NONE This event is accredited for CME credits by EBAP and EACCME and speakers are required to disclose their potential conflict of interest. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for audience members to determine whether the speaker’s interests, or relationships may influence the presentation. The ERS does not view the existence of these interests or commitments as necessarily implying bias or decreasing the value of the speaker’s presentation. Drug or device advertisement is forbidden.

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

COVID-19: clinical presentation Watch for symptoms People with COVID-19 have a wide range of symptoms – ranging from mild symptoms to severe illness. These symptoms may appear 2 -14 days after exposure to the virus: • Fever • Cough • Shortness of breath or difficulty breathing; • Chills • Repeated shaking with chills; • Muscle pain • Headache • Sore throat • New loss of taste or smell.

COVID-19: emergency warning signs When to Seek Medical Attention? If you have any of these emergency warning signs* for COVID-19 get medical attention immediately: • Trouble breathing • Persistent pain or pressure in the chest • New confusion or inability to arouse • Bluish lips or face *This list is not all inclusive. Please consult your medical provider for any other symptoms that are severe or concerning to you.

COVID-19: 3 disease stages H. Siddiqi and M. Mehra, J. of Heart and Lung Transplantation 2020 in press.

Early stage COVID-19 pneumonia Day 2 - GGO Day 5 – “crazy paving”

Advanced stage COVID-19 pneumonia Day 7 – GGO, consolidation & fibrotic streaks Day 8 – diffuse bilateral GGO, consolidation

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

Asthma Management and Prevention Program Goals of Long-term Management 1. Achieve and maintain control of symptoms 2. Maintain normal activity levels, including exercise 3. Maintain pulmonary function as close to normal levels as possible 4. Prevent asthma exacerbations 5. Prevent asthma mortality 6. Avoid adverse effects from asthma medications © Global Initiative for Asthma

H. Reddel et al, ERJ 2019.

GINA 2020, Box 3 -5 A

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Does asthma make COVID-19 worse? Treatment: asthma; COVID-19 Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

Potential steps in the development and evolution of SARS-Co. V-2 infection; effects of asthma and ICS D. Halpin et al, ERJ 2020.

TABLE 1. Reported outcomes among COVID-19 patients of all ages, by hospitalization status, underlying health condition, and risk factor for severe outcome from respiratory infection — United States, February 12–March 28, 2020 Underlying health condition/Risk factor for severe outcomes from respiratory infection (no. , %) Total with case report form (N = 74, 439) Missing or unknown status for all conditions (67, 277) No. (%) Not hospitalized Hospitalized, non-ICU admission Hospitalization status unknown 12, 217 5, 285 1, 069 55, 868 7, 074 4, 248 612 55, 343 5, 143 1, 037 457 525 1, 388 (27) 732 (71) 358 (78) 214 (41) 331 (6) 251 (24) 148 (32) 54 (10) 363 (7) 152 (15) 94 (21) 47 (9) 239 (5) 242 (23) 132 (29) 34 (6) 141 (3) 63 (6) 41 (9) 19 (4) 51 (1) 95 (9) 56 (12) 11 (2) 72 (1) 31 (3) 4 (1) 36 (7) 17 (0. 3) 25 (2) 7 (2) 3 (1) 24 (1) 9 (1) 7 (2) 1 (0. 2) 583 (11) 359 (35) 170 (37) 70 (13) 80 (2) 45 (4) 33 (7) 7 (1) Current smoker (96, 1. 3%) 61 (1) 22 (2) 5 (1) 8 (2) None of the above conditions¶ (4, 470, 62. 4%) 3, 755 (73) 305 (29) 99 (22) 311 (59) Total with completed information (7, 162) One or more conditions (2, 692, 37. 6%) Diabetes mellitus (784, 10. 9%) Chronic lung disease* (656, 9. 2%) Cardiovascular disease (647, 9. 0%) Immunocompromised condition (264, 3. 7%) Chronic renal disease (213, 3. 0%) Pregnancy (143, 2. 0%) Neurologic disorder, neurodevelopmental, intellectual disability (52, 0. 7%)† Chronic liver disease (41, 0. 6%) Other chronic disease (1, 182, 16. 5%)§ Former smoker (165, 2. 3%)

Advanced age and comorbidities make COVID worse TABLE 2. Hospitalization with and without intensive care unit (ICU) admission, by age group among COVID-19 patients aged ≥ 19 years with and without reported underlying health conditions — United States, February 12–March 28, 2020* Hospitalized without ICU admission, No. (% range†) ICU admission, No. (% range†) Underlying condition present/reported§ Age group (yrs) Yes No 19– 64 285 (18. 1– 19. 9) 197 (6. 2– 6. 7) 134 (8. 5– 9. 4) 58 (1. 8– 2. 0) ≥ 65 425 (41. 7– 44. 5) 58 (16. 8– 18. 3) 212 (20. 8– 22. 2) 20 (5. 8– 6. 3) Total ≥ 19 710 (27. 3– 29. 8) 255 (7. 2– 7. 8) 346 (13. 3– 14. 5) 78 (2. 2– 2. 4) § Includes any of following underlying health conditions or risk factors: chronic lung disease (including asthma, chronic obstructive pulmonary disease, and emphysema); diabetes mellitus; cardiovascular disease; chronic renal disease; chronic liver disease; immunocompromised condition; neurologic disorder, neurodevelopmental, or intellectual disability; pregnancy; current smoker; former smoker; or other chronic disease. MMWR Morb Mortal Wkly Rep 2020; 69: 382– 386.

SARS-Co. V-2 binds to ACE 2 M. Vaduganathan et al, NEJM 2020.

Sputum gene expression of ACE 2, TMPRSS 2 and ICAM 1 in asthma and healthy subjects ACE 2: TMPRSS 2: ICAM-1: M. Peters et al, AJRCCM 2020 in press.

Effect of ICS use on sputum gene expression in subjects with asthma M. Peters et al, AJRCCM 2020 in press.

ACE 2 expression in single-cell transcriptomics of bronchial epithelial cells from never and current smokers G. Cai et al, AJRCCM 2020 in press.

Smoking, COPD and ACE 2 expression in lung M. Jacobs, …, K. Bracke, submitted.

Smoking and COPD are associated with increased expression of ACE 2 in lung M. Jacobs, …, K. Bracke, submitted.

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

COVID-19 and asthma treatment Advise patients with asthma to continue taking their prescribed asthma medications, particularly inhaled corticosteroids (ICS). Asthma medications should be continued as usual. Stopping ICS often leads to potentially dangerous worsening of asthma. Smoking cessation! For patients with severe asthma: Ø Ø continue biologic therapy, and provide training to patients to self-administer (or homecare) do not suddenly stop OCS if prescribed.

Long-term use of OCS in uncontrolled severe asthma and COVID-19 , diabetes G. Brusselle, unpublished observations. hypertension risk factors for severe COVID-19.

COVID-19 and asthma action plans Make sure that all patients have a written asthma action plan with instructions about: – Increasing controller and reliever medication when asthma worsens – Taking a short course of OCS for acute asthma exacerbations if clinically indicated – When to seek medical help.

COVID-19 and asthma inhalers Avoid nebulizers where possible – Nebulizers increase the risk of disseminating virus to other patients AND to health care professionals. – Pressurized metered dose inhaler (p. MDI) via a large spacer is the preferred treatment during severe exacerbations, with a mouthpiece or tightly fitting face mask if required.

COVID-19: targeted therapies ~ disease stage H. Siddiqi and M. Mehra, J. of Heart and Lung Transplantation 2020 in press.

COVID-19: targeted therapies ~ disease stage RCTs are crucial to demonstrate efficacy and safety of antiviral drugs and immunomodulatory treatments! H. Siddiqi and M. Mehra, J. of Heart and Lung Transplantation 2020 in press.

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

Conflict of interest disclosure: Antonio Spanevello I have no real or perceived conflicts of interest that relate to this presentation. X I have the following real or perceived conflicts of interest that relate to this presentation: Affiliation / Financial interest Commercial Company Grants/research/speaker support GSK, NOVARTIS, BOEHRINGER ASTRAZENECA , CHIESI, , MENARINI, LUSOFARMACO Honoraria or consultation fees: GSK, , SANOFI, ASTRAZENECA, CHIESI Participation in a company sponsored bureau: NONE Stock shareholder: NONE Spouse / partner: NONE Other support / potential conflict of interest: NONE This event is accredited for CME credits by EBAP and EACCME and speakers are required to disclose their potential conflict of interest. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for audience members to determine whether the speaker’s interests, or relationships may influence the presentation. The ERS does not view the existence of these interests or commitments as necessarily implying bias or decreasing the value of the speaker’s presentation. Drug or device advertisement is forbidden.

For patients with asthma, viral respiratory tract infections can have a profound effect on the expression of disease or loss of control.

Among infectious agents, human rhinoviruses are. the most prevalent in regard to asthma exacerbations. Coronavirus has not a higher frequency in AAE than control group

In a study of 49 adults presenting to the emergencies with AAE Coronavirus was found in 4% of induced sputum samples. Coronavirus seem to have minor contribution to AAE.

No asthmatic patient was identified in this report.

A total of 549 patients with COVID-19 were enrolled, of whom 548 cases were included in the study. The prevalence of asthma in COVID-19 patients was only 0. 9% It has been speculate that Th 2 immune response in asthmatic patients could counter the inflammation process induced by Co. V-2 infection.

A prospective case series involving patients with immuno-mediated inflammatory disease (rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, psoriasis……. ) and confirmed or highly suspected COVID – 19 disease
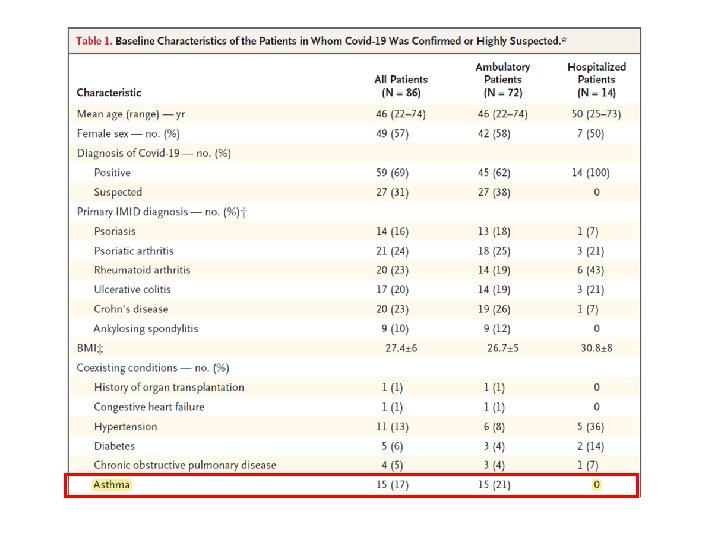
")
Twenty-four patients from nine Seattle-area hospitals who were admitted to Intensive Care Unit (ICU) with confirmed infection with severe acute respiratory syndrome Coronavirus -19
 had asthma, and all 3 had recently received, as an outpatients,")
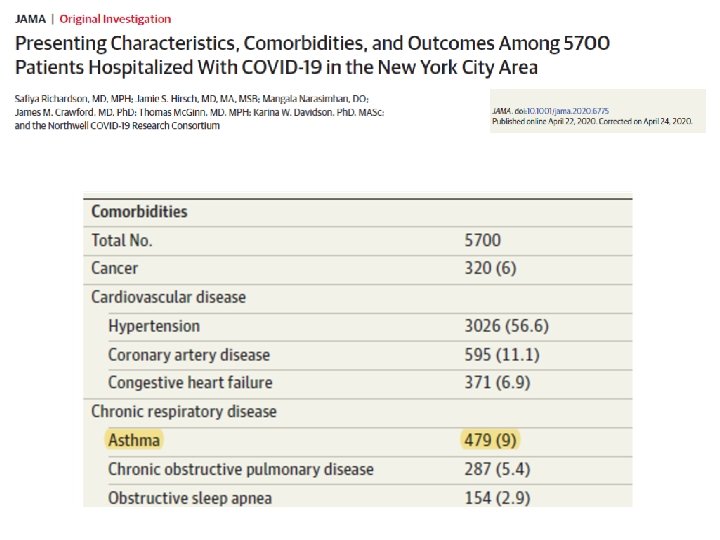
3 patients (14%) had asthma, and all 3 had recently received, as an outpatients, systemic glucocorticoids for a presumed asthma exacerbation

The present report describes characteristics of 23188 SARS-Co. V-2 patients dying in Italy. Asthma was not reported

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session
 Blood 30 25 20 15 10 5 0 Selected Sputum Entire Sputum")
Eosinophils (%) Blood 30 25 20 15 10 5 0 Selected Sputum Entire Sputum

150 hospitalized adult patients comprising 50 patients with rhinovirus infection, and 100 patients with influenza virus infection (A and B) Some virus (RV) induce increase of blood eosinophils.
 had eosinopenia (eosinophil counts < 0.")
More than half of the patients (52. 9%) had eosinopenia (eosinophil counts < 0. 02 x 10 9 /l)

Male, 84 -year-old, non smoker Comorbidities: hypertension, atrial fibrillation 11/03/2020 Admitted to hospital for femur osteosynthesis 20/03/2020 Admitted to the Rehabilitation Unit After a few days: fever, leukocytes and neutrophils increase, CRP 7. 59 mg Paracetamol Hydroxychloroquine O 2 10 -15 L/min 23/03/2020 SARS-Co. V-2 negative nasopharyngeal swab 29/03/2020 SARS-Co. V-2 negative nasopharyngeal swab 03/04/2020 SARS-Co. V-2 positive nasopharyngeal swab Blood eosinophils rapidly decreased during the infection and their increase is a mark of viral infection resolution

Epidemiologic and Clinical Characteristics of 91 Hospitalized Patients With COVID-19 in Zhejiang, China: A Retrospective, Multi-Centre Case Series Guo-Qing Qian 1, Nai-Bin Yang 1, Feng Ding 2, Ada Hoi Yan Ma 3, Zong-Yi Wang 4, Yue-Fei Shen 5, Chun-Wei Shi 5, Xiang Lian 6, Jin-Guo Chu 1, Lei Chen 1, Zhi-Yu Wang 1, Da-Wei Ren 7, Guo-Xiang Li 1, Xue-Qin Chen 8, Hua-Jiang Shen 2, Xiao-Min Chen 1 QJM 2020 Mar 17; online ahead of print Eosinopenia could be due to the sequestration of eosinophils by chemokines into the inflammation sites

To report findings of two complete autopsies of severe acute respiratory syndrome coronavirus 2 positive individuals who died in Oklahoma (United Statees) in March 2020. There was interstitial chronic inflammation composed mainly of lymphocytes. No eosinophils or neutrophils were identified. Sequestration of eosinophils does not seem occorring in post mortem analysis
 in COVID is due to secundary hemophagocytosis:")
Hypotesis The decrease of blood eosinophils (eosinopenia) in COVID is due to secundary hemophagocytosis: due to the cytokine storm (IL-6, IL-1 and TNF) in severe COVID. Macrophages are too strongly activated and eat (phagocytose) eosinophils and neutrophils In contrast, lymphocytes and monocytes decrease in the blood in COVID due to massive migration into the lungs.

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session
 pages 17 -18 Available from:")
GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION (2020 Update) pages 17 -18 Available from: www. ginasthma. com

The purpose of this guideline is to maximise the safety of adults and children with severe asthma during the COVID-19 pandemic, while protecting staff from infection. The recommendations are based on evidence and expert opinion.

Comunicate with patients, help to alleviate any anxiety and fear they may have about COVID-19

Tell all patients or their parent or carer, to continue taking their regular medicines Tell patients to continue using inhaled corticosteroids because stopping can increased the risk of asthma exacerbation. If the patient usually attends hospital to have biological treatments, think about if they can be trained to selfadminister, or could be treated at a community clinic or at home

Tell patients not to share their inhalers and devices with anyone else Tell patients or their parent ora carer to clean equipment such as spacers and peak flow meter regularly

Only carry out Bronchoscopy and most Pulmonary Function Tests for urgent cases and if the results will have a direct impact on patient care, because these tests have the potential to spread COVID-19.

Minimise face-to-face contact If patients are having a face-to-face appointment, on the day of the appointment first screen them by telephone to make sure they have not developed symptons of COVID-19 Ask patients to attend appointments with no more than 1 family member Minimise time in the waiting area
 pages 17 -18 Available from:")
GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION (2020 Update) pages 17 -18 Available from: www. ginasthma. com Interim guidance on asthma management during the COVID – 19 pandemic Advice patient with asthma to continue taking their prescribed asthma medications, particurarly ICS (alone or in combination with LABA), and OCS if prescribed Make sure that all patients have a written asthma action plan Where possible, avoid use of nebulizers due to the risk of trasmitting infection to other patients and to healthcare workers
 pages 17 -18 Available from:")
GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION (2020 Update) pages 17 -18 Available from: www. ginasthma. com Interim guidance on asthma management during the COVID – 19 pandemic Avoid spirometry in patients with confirmed or suspected COVID Follow infection control recommendations if other aerosolgenerating procedures are needed (oxygen therapy, sputum induction, NIV, Intubation) Follow local healthadvice about hygiene strategies and use of personal protective equipment, as new information becomes available in your country or region

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

Questions from patients with asthma How can I tell if it is my asthma or COVID-19? How do I know when to take prednisolone if I can't tell the difference? I have had COVID-19 and I am experiencing breathing difficulties afterwards. What should I do? Does COVID-19 cause permanent lung damage and breathlessness? Will it reduce my lifespan if I recover?

Questions from patients with asthma I have 'severe' asthma; do I have a greater risk for (severe) COVID than someone with 'moderate' or 'mild' asthma? Am I more at risk because I am on biologic treatment?

COVID-19 and Asthma: overview COVID-19: clinical presentation Asthma: management in 2020 Are asthma patients at increased risk of COVID-19? Treatment: asthma; COVID-19 Epidemiology Eosinophilic inflammation in asthma and COVID-19 Guidelines on COVID-19 and severe asthma Patients perspectives Q & A session

COVID-19 and asthma: take home messages Well-controlled asthma is not associated with an increased risk of (severe) COVID-19. Use of inhaled corticosteroids (ICS) in subjects with asthma prevents exacerbations, is associated with reduced expression of ACE 2 in sputum, and should be continued during the COVID pandemic. Smoking increases the risk of severe COVID-19, and is associated with increased expression of ACE 2 in airways and lungs. The COVID-19 pandemic impacts (severe) asthma care. Antiviral drugs and immunomodulatory treatments need to be tested in randomized controlled trials (RCT).

Acknowledgements: Department of Respiratory Medicine ‘Laboratory for Translational Research in Obstructive Pulmonary Diseases’ ‘Clinical Research Unit’ Guy Joos Guy Brusselle Eric Derom Guy Joos Bart Lambrecht Ken Bracke Greet Barbier Tania Maes Indra De Borle Evy Blomme Katleen De Saedeleer Merel Jacobs Anouck Goethals Anja Delporte Sara Wijnant Ann Neesen Stefanie Vermeersch Hannelore Van Eeckhoutte Eva Van Braeckel Sven Verschraegen Benedicte Demeyere

COVID-19: potential impact on asthma patients Back-up slides

BMJ 2020.
 recommendations for")
Resources for COVID-19 Information for health professionals – World Health Organization (WHO) recommendations for infection control www. who. int/publications-detail/infection-prevention-and-control-duringhealth-care-when-novel-coronavirus-(ncov)-infection-is-suspected 20200125 – Centers for Disease Control and Prevention (CDC) www. cdc. gov/coronavirus/2019 -n. Co. V/hcp/index. html – European Respiratory Society (ERS) https: //www. ersnet. org/the-society/news/novel-coronavirus-outbreak-update-and-information-for-healthcare-professionals

Resources for COVID-19 Information for patients – CDC: https: //www. cdc. gov/coronavirus/2019 -ncov/index. html. Information for health systems – www. who. int/emergencies/diseases/novel-coronavirus-2019/technicalguidance Follow local health advice about hygiene strategies and use of personal protective equipment as new information becomes available in your country or region
- Slides: 73