Acute coronary syndromes DR G SWARNA LATHA DEVI





: typical acute chest pain and persistent (>20 min) ST-segment elevation")

: acute chest pain without persistent ST-segment elevation persistent or transient ST")











 2. Non-atherosclerotic aetiology: (type 2 -5) arteritis")


 pain at rest - retrosternal pressure or")
 Typical chest pain 2) Nauzea 3) Sweating")



 RV failure - ↑")










 creatinine kinase (CK)")

























- Slides: 66
Acute coronary syndromes DR. G. SWARNA LATHA DEVI. M. D. PROF. MEDICINE
ACS - introduction an umbrella term for any condition where the blood supplied to the heart muscle is reduced the most feared complications of coronary artery disease (CAD) are associated with high mortality and morbidity Cardiovascular diseases (CVD) - presently the leading causes of death in industrialized countries
Definition The clinical presentations of CAD include: silent ischaemia stable angina pectoris heart failure unstable angina myocardial infarction (MI) sudden death
Acute coronary syndromes ACS are usually divided into: Unstable angina - only ischemia, lack of necrosis STEMI - ST - elevation MI NSTEMI - non-ST elevation MI Sudden death - due to cardiac arrhythmias
Acute coronary syndromes
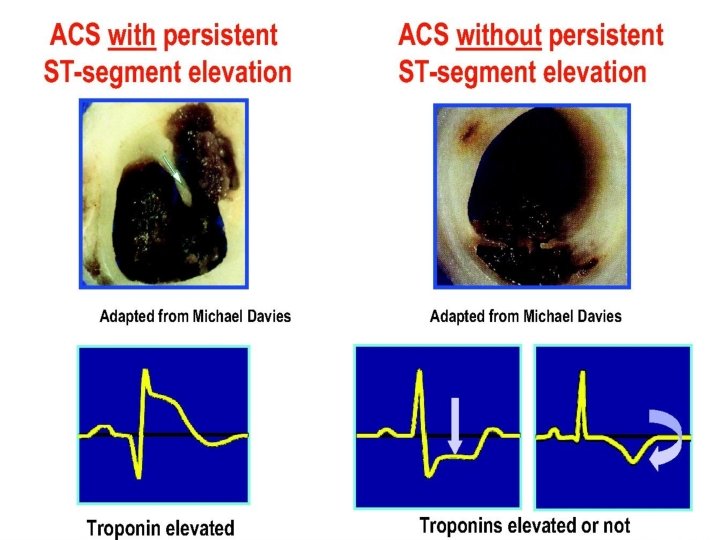
Definition ST-elevation ACS (STE-ACS): typical acute chest pain and persistent (>20 min) ST-segment elevation generally reflects an acute total coronary occlusion most will ultimately develop an STelevation MI (STEMI).
ST elevation on the ECG
Definition non-STE-ACS (NSTE-ACS): acute chest pain without persistent ST-segment elevation persistent or transient ST segment depression or T-wave inversion further qualified into non-ST elevation MI (NSTEMI) or unstable
ST depresion on the ECG
Pathophysiology of ACS Atherothrombosis Atherosclerosis - a fixed and barely reversible process of gradual luminal narrowing (slowly over decades) Thrombosis - a dynamic and potentially reversible process causing rapid complete or partial occlusion of the coronary artery
Vulnerable plaque a large lipid core a low density of smooth muscle cells a high concentration of inflammatory cells a thin fibrous cap covering the lipid core acute thrombosis induced by a plaque rupture
Vulnerable plaque
Vulnerable plaque Hamm, Cardiovascular Medicine 2006
Vulnerable patient Multiple sites of plaque rupture with or without intracoronary thrombosis Elevated levels of various systemic markers of inflammation, thrombosis and coagulation system activation Hypercholesterolaemia Tobacco smoking
Epidemiology The annual incidence of NSTE-ACS is higher than STEMI The annual incidence of hospital admissions for NSTE-ACS is in the range of 3 per 1000 inhabitants sex differences - men account for more than 90% of patients with AMI at the age under 40 y. (a hormonal profile of woman has a protective effect) age differences - in patients aged under 40 y. only one heart artery is affected
Prognosis of STE vs. NSTE-ACS Hospital mortality - higher in patients with STEMI than among those with NSTE-ACS (7 vs. 5%) 6 months mortality - the mortality rates are very similar in both conditions (12 vs. 13%) Long-term follow-up - death rates higher among those with NSTE-ACS than with STE-ACS
Prognosis of STE vs. NSTE-ACS The causes of the higher death rates of NSTE-ACS than of STE-ACS pts. during long-term follow-up are: older pts. more co-morbidities (diabetes and renal failure). a greater extent of coronary artery and vascular diseases persistent triggering factors such as inflammation
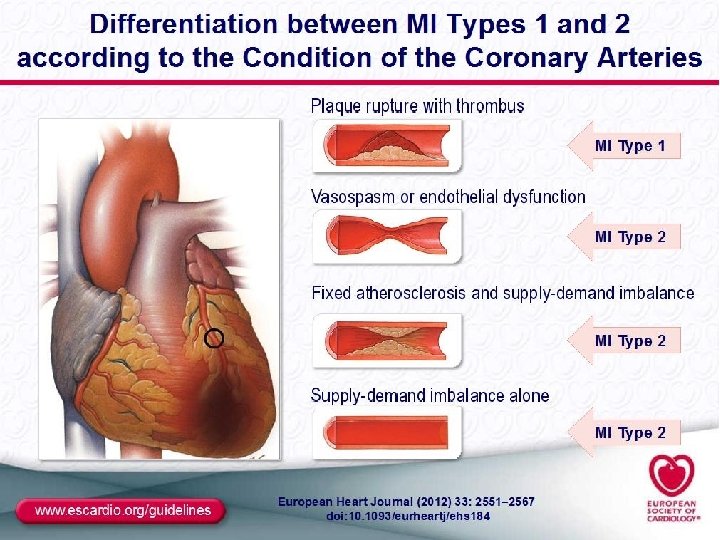
Classification of MI Type 1 – spontaneous MI related to ischemia due to a primary coronary event such as plaque erosion and/or rupture, fissuring, or dissection Type 2 – MI secondary to ischemia due to either increased oxygen demand or decreased supply, e. g. coronary artery spasm Coronary embolism, Anemia, arrhythmias , Hypertension, or hypotension
Classification of MI Type 3 – sudden unexpected cardiac death, including cardiac arrest but death occurring before blood samples could be obtained Type 4 – associated with PCI: Type 4 a – MI associated with the procedure of PCI Type 4 b – MI associated with stent thrombosis Type 5 – MI associated with CABG
Myocardial infarction 1. Atherosclerotic aetiology (type 1) 2. Non-atherosclerotic aetiology: (type 2 -5) arteritis trauma dissection congenital anomalies cocaine abuse complications of cardiac catheterization, CABG
Diagnosis of acute MI 2 from 3 criteraia must be fulfilled : • Clinical symtoms – Chest pain • ECG changes – ST elevation or depression – negative T wave • Elevated cardiac biomarkers – Troponin I or T – CK-MB – myoglobin
Diagnosis of ACS Clinical presentation History of patient Physical examination Electrocardiogram Biochemical markers - troponin Non-invasive imaging - Echo Imaging of coronary arteries - coronary angiography
Clinical presentation STE/NSTE-ACS: Intense prolonged (20 min) pain at rest - retrosternal pressure or heaviness (‘angina’) radiating up to the neck, shoulder and jaw and down to the ulnar aspekt of the left arm May be accompanied by other symptoms such as diaphoresis, nausea, abdominal pain, dyspnoea, … Unstable angina: New onset severe angina (class III of CCS) Post-MI angina.
Clinical presentation 1) Typical chest pain 2) Nauzea 3) Sweating
Clinical presentation Atypical presentations are not uncommon epigastric pain recent-onset indigestion stabbing chest pain with some pleuritic features increasing dyspnoea - often can be observed in younger (25 -40 y. ), older (75 y. ), in women, in pts. with diabetes, chronic renal failure, or dementia.
Clinical presentation The presence of tachycardia, hypotension, or heart failure needs rapid diagnosis and management, often indicating a poor prognosis of this patient with ACS It is important to identify the clinical circumstances such as anaemia, infection, inflammation, fever, and metabolic or endocrine (in particular thyroid) disorders (may exacerbate or precipitate ACS)
Physical examination Frequently normal Signs of heart failure or haemodynamic instability Dif. dg. : - nonischaemic cardiac disorders: pulmonary embolism, aortic dissection, pericarditis, valvular heart disease) - extra-cardiac causes: pulmonary diseases - pneumothorax, pneumonia, pleural effusion)
Physical examination Heart failure Tachycardia, tachypnoe Pulmonary rales (pulmonary congestion) RV failure - ↑ jugular congestion, hepatomegaly Hypotension ↓ 100/60 mmhg cardiac shock (tachycardia) ↑ vagal nerve activity (bradycardia - inferior IM) Bradycardia AV block Inferior IM - non-serious, frequent Anterior IM - serious, rare
Electrocardiogram The resting 12 -lead ECG is the first-line diagnostic tool in the assessment of patients with suspected ACS. STE-ACS… ST-elevation NSTE-ACS…ST-segment shifts and Twave changes A completely normal ECG does not exclude the possibility of ACS.
Ischemia • T wave inversion, ST segment depression • Acute injury: ST segment elevation • Dead tissue: Q wave
ST-Segment Elevation
Q Waves Non Pathological Q waves of less than 2 mm are normal Pathological Q waves of more than 2 mm indicate full thickness myocardial damage from an infarct Late sign of MI (evolved)
Pericarditis
Location of MI
Location of MI ST elevation only: Anteroseptal - V 1 -V 3 Anterolateral - V 1 -V 6 Inferior wall - II, III, a. VF Lateral wall - I, a. VL, V 4 -V 6 Right ventricular - RV 4, RV 5 Posterior- R/S ratio >1 in V 1 and T wave
Location of MI
Location of MI
Location of MI
Biochemical markers Markers of myocardial injury: cardiac troponins (I and T) creatinine kinase (CK) CK isoenzyme MB (CK-MB) Myoglobin repeated blood sampling and measurements are required 6– 12 h after admission and after any further episodes of severe chest pain
Biochemical markers in ACS
Biochemical markers Non-coronary condition with Troponin elevation • Severe congestive heart failure • Aortic dissection, valve disease • Myocarditis • Hypertrophic CMP, Stress CMP • Hypertesive crisis • Acute and chronic renal failure • Acute neurological disease
Other biomarkers C-reactive protein - inflamation long-term prognosis Natriuretic peptides - heart failure shor-term prognosis Serum creatinine - renal function Short and long-term prognosis N o role for the diagnosis of ACS, but effect on short- or long-term prognosis and dif. Dg.
Non-invasive myocardial imaging Echocardiography - to evaluate LV systolic function, aortic stenosis, aortic dissection, pulmonary embolism, or hypertrophic cardiomyopathy - should be routinely used in emergency units for the risc stratification Stress echocardiography, stress scintigraphy evidence of ischaemia or myocardial viability (in stabilized patients)
Imaging of the coronary anatomy The imaging of the coronary anatomy is the most importat diagnostics method in evaluation of acute coronary syndrome The gold standard of patients with ACS is conventional invasive coronary angiography
Treatment of MI while STEMI is an urgent situation with turbulent symptomatology, NSTEMI may have symptoms much milder and above its immediate prognosis is better Pts. should stay on coronary care unit - 2 -3 days, than standard cardiology department the total length of hospitalization is around 1 week even after leaving the CCU patients are able to move around the room and in the following days rehabilitate and before discharge they are able to walk up the stairs return to job possible approximately one month after
Treatment of STEMI Open the occluded artery as soon as possible to restore blood flow for the heart ‘‘Time is muscle“ Check for complication of myocardial infarction and treat them: arrhythmia heart failure bleeding
Process of the percutaneous coronary intervention
Process of the implantation of stent
Aspiration trombectomy elimination of trombus to prevent embolisation
Pre-hospital management Antiplatelet therapy Acetylosalicid acid 400 -500 mg (i. v. or p. o. ), Clopidogrel 600 mg or ticagrelor 180 mg or prasugrel 60 mg Antithrombin therapy Heparin 5 000 - 10 000 IU i. v. or enoxaparine Resolve pain and fear analgesic drugs benzodiazepine
Pre-hospital management Nitrate - pain, hypertesion, heart failure Isosorbide dinitrate 1 -5 mg i. v. Monitoring vital function and ECG ventricular fibrilation terminated by cardioversion
Pre-hospital management Betablockers - tachycardia, hypertension Metoprolol - dose 25 -50 mg oral or 2 mg i. v. ACE inhibitors - hypertension Perindopril - dose 5 mg oral Diuretic - heart failure Furosemide 20 - 40 mg i. v. Anti-arrhythmic drugs -no prophylaxis Mesocain 1% 10 m. L i. v. Amiodarone 150 mg i. v. bolus
Hospital and discharge therapy Antiplatelet therapy Acetylosalicid acid - dose 100 mg p. o. Clopidogrel 75 mg or ticagrelor 90 mg twice a day or prasugrel 10 mg Statins - benefit for all patients with IM Atorvastatin 40 - 80 mg, rosuvastatin 20 - 40 mg ACE inhibitors - benefit for all patient with IM, more expressed in left ventricular dysfunction perindopril - dose 5 -10 mg oral Betablockers - 1 - 3 years after MI, longer for pts. With left ventricular dysfunction, tachyarrhythmia
Complications of MI Early complications Heart failure, cardiogenic shock Mechanical complications : - rupture of free wall of left ventricle - ventricular septal defect - acute mitral regurgitation Arrhythmia - ventricular (up to 48 h) - bradycardia (9 -25% of pts) Late complications pericarditis Aneurysm of left or right ventricle
Tamponade
VSD
VSD
Aneurysm
Treatment of NSTEMI Risk short-term factors: - repeated ischemia - ST depresion - dynamic changes of ECG (ST and wave T) - troponin positivity - trombus during CAG sk i r g s e ass n i d e Risk factors for long-term prognosis: e l b d - older age (≥ 75 years) n a e. MI r - previous o c s sc - diabetes Ri - CRP - 3 -vessels or left main disease - left ventricular dysfunction t n me
Treatment of NSTE-ACS To immediate examination are indicated patients with: history of CAD or previous revascularization severe recurrent angina left ventricular dysfunction, heart failure or ventricular arrhythmias
Treatment of NSTE-ACSvs. STE thrombolysis is not at NSTEMI used the base of treatment is again antithrombotic therapy and revascularization - mostly via PCI in patients with multiple coronary disease more frequently to surgery revascularization
Stenosis of LMCA
CABG - LIMA ad RIA, SVG ad RMS
Thank you for your attention