XEROSTOMIA Physiology Etiology Epidemiology Pathogenesis Diagnosis and Treatment





 Begins development at 6")












 o Typically")









 n Anticholinergic (dicyclomine, mepenzolate)")
 n Antiparkinsonian (biperiden, selegiline)")
 Diet pills Diuretic (spironolactone,")
















- Slides: 50
XEROSTOMIA Physiology, Etiology, Epidemiology, Pathogenesis, Diagnosis, and Treatment
XEROSTOMIA After studying this lecture, students should be able to: n n n describe the oral anatomy and physiology related to salivary function as well as the role of saliva in the oral cavity. discuss the etiology and epidemiology of xerostomia. relate treatment options for xerostomia.
XEROSTOMIA n DEFINITION u “Xero” = Dry & “Stomia” = Mouth Xerostomia can be defined as the subjective sensation of oral dryness that may or may not be associated with a reduction in the amount of saliva and the chemical composition of saliva u Have a deleterious effect on oral function and general well being u
XEROSTOMIA n Complications u Decrease taste sensation and impair chewing ability thereby altering regular eating pattern u Tend to avoid dry foods (bread) and sticky foods (peanut butter) as unable to chew or swallow effectively u Impair speech, causes cracks in oral mucosa and halitosis u Make denture wearing uncomfortable due to reduced surface tension between the dry mucosa and the denture, leading to poor diet.
XEROSTOMIA n Complications continued u Contributing factor to high prevalence of geriatric malnutrition in the USA u Poses social problems by affecting the willingness or ability of patient to talk u Contributes to pain, caries and oral infection
XEROSTOMIA Production of Saliva Oral Glandular Tissue 3 (saliva secreting) Begins development at 6 weeks gestation and is completed by about the 12 th week The glandular tissue continues to enlarge until birth
NORMAL FUNCTION OF SALIVA n n n n Hydrating–moisturizing Cleansing Lubrication Digestion Remineralization of dentition (so fight tooth decay) (p. H maintenance, buffering) Maintenance of mucosal integrity Immunity mediator (Ig. A), lysozyme, lactoperoxidase, histatins) Antimicrobial (antifungal, antibacterial) Stimulation of minor salivary glands Cellular maintenance Enables swallowing Enables tasting Enables speech articulation Physically protects teeth by coating them with glycoproteins and mucoids.
Histatin ATP ATP G 1 arrest Nucleus ROS
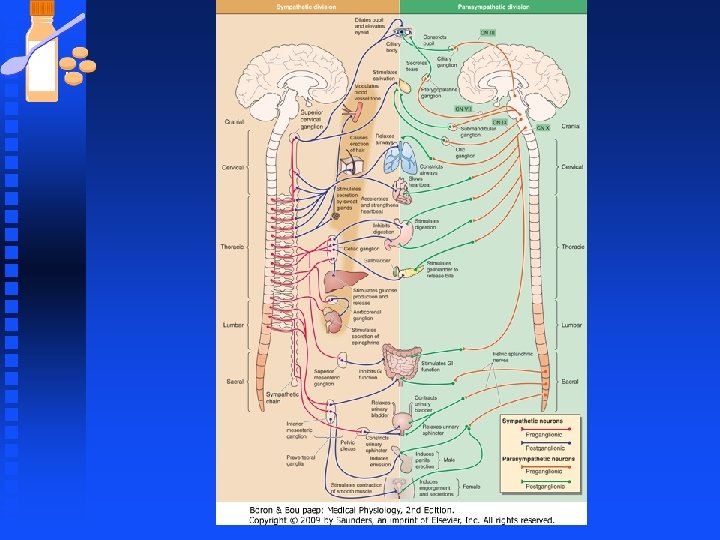
XEROSTOMIA Mechanisms of Salivary Production 3 Salivary glands Neural innervation Cause one of two divisions Sympathetic Causes very dry, thick, ropy saliva Parasympathetic Causes thin, watery, profuse salivation
XEROSTOMIA Salivary Gland Classifications by Secretion 3 n n n Serous: very thin and watery Mucous: very thick and viscous Mixed secretions: mixture of the two
XEROSTOMIA Salivary Gland Classifications by Secretion 3 n Serous: very thin and watery o o parotid gland lingual glands of von Ebner (serous glands of von Ebner) n n Mucous: very thick and viscous Mixed secretions: mix of the two Serous acini
XEROSTOMIA Salivary Gland Classifications by Secretion 3 n n Serous: very thin and watery Mucous: very thick and viscous o palatine glands posterior lingual glands o labial buccal glands o n Mixed secretions: mix of the two Mucous acini
XEROSTOMIA Salivary Gland Classifications by Secretion 3 n Serous: very thin and watery Mucous: very thick and viscous n Mixed secretions: mix of the two n o o o Sublingual glands • Mostly mucous with some serous Submandibular glands • Mostly serous with some mucous Anterior lingual glands • Mixed secretion Mixed: mostly serous acini (dark), partially mucous acini (light cells)
XEROSTOMIA Salivary Gland Classifications by Major or Minor Glands 3 n n Major glands o Secrete saliva intermittently Minor glands o Secrete saliva continuously
XEROSTOMIA The Major Glands n Parotid gland 3, 4 o Largest of the 3 major glands o Produces 30% of total saliva output § § o o o Parotid duct is also known as Stenson’s duct Parotid/Stenson’s duct exits opposing the maxillary second molar Located anterior but inferior to the external auditory meatus Innervated by sympathetic and parasympathetic divisions Secretes serous type saliva Parotid gland
XEROSTOMIA The Major Glands n Submandibular gland 3, 4 o Second largest salivary gland o Produces 65 -70% of total saliva output § § o o The duct is called Wharton’s duct exits on the floor of the mouth opposing the lingual surface of the tongue Located in a depression on the lingual side of the mandibular body Innervated by parasympathetic nerve endings and possesses NO sympathetic receptors The parasympathetic fibers arrive through the facial and glossopharyngeal nerves Mixed secretion – mostly serous Submandibular gland
XEROSTOMIA The Major Glands n Sublingual glands 3, 4 o Smallest of the major glands o Produce less than 5% of total saliva output § § o o o Saliva delivered via the ducts of Bartholin The Bartholin ducts exit on the base of the lingual surface of the tongue Innervated by parasympathetic fibers Little or no sympathetic influence Mixed secretion – mostly mucous Sublingual gland
XEROSTOMIA The Minor Salivary Glands 3 Minor salivary glands are found throughout the mouth: u u u Lips Buccal mucosa (cheeks) Alveolar mucosa (palate) Tongue dorsum and ventrum Floor of the mouth Together, they play a large role in salivary production.
XEROSTOMIA Salivary Flow 3 n Unstimulated Flow (resting salivary flow―no external stimulus) o Typically 0. 2 m. L – 0. 3 m. L per minute o Less than 0. 1 m. L per minute means the person has hyposalivation § Hyposalivation – not producing enough saliva n Stimulated Flow (response to a stimulus, usually taste, chewing, or medication [eg, at mealtime]) o Typically 1. 5 m. L – 2 m. L per minute o Less than 0. 7 m. L per minute is considered hyposalivation
XEROSTOMIA Salivary Flow 3 n n The average person produces approximately 0. 5 L – 1. 5 L per day Salivary flow peaks in the afternoon Salivary flow decreases at night when the parotid gland shuts down There is a difference in the quality between stimulated and unstimulated saliva
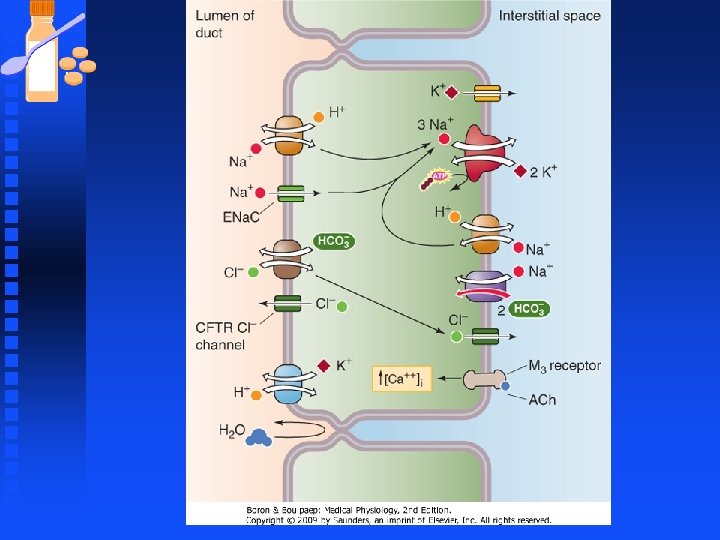
XEROSTOMIA Salivary Composition 1 n n n 90% of saliva is water 10% is composed of inorganic and organic ions, and cellular components o sodium, potassium, and calcium are positive ions (cations) o chloride, bicarbonate, and phosphates are negative ions (anions) The cationic and anionic components play an important role in the function of saliva
XEROSTOMIA Ions and Salivary Flow 3 As saliva passes through the salivary ducts, cations (sodium and chloride) are reabsorbed into the adjacent blood vessels. (comment)
XEROSTOMIA Ions and Salivary Flow 3 As saliva passes through the salivary ducts, cations (sodium and chloride) are reabsorbed into the adjacent blood vessels. In exchange, bicarbonates and potassium are transferred from the blood vessels into the salivary ducts.
XEROSTOMIA Ions and Salivary Flow 3 Stimulated Salivary Flow • Saliva passes through the salivary duct very rapidly (a negative result of fast flow) o It impedes the exchange of sodium and chloride for potassium and bicarbonate Unstimulated Salivary Flow • Has a high content of potassium and bicarbonate (a positive result of slow flow) o The quality of unstimulated saliva will change when flow increases because of a stimulus (chewing gum, thinking about lemons, looking at a food you crave)
XEROSTOMIA Fluoride and Saliva 3 Fluoride is also secreted in saliva. Unlike the ions in saliva, the fluoride content (level) is not altered whether the salivary flow is simulated or unstimulated.
XEROSTOMIA Organic Components of Saliva 3 Enzymes: o o o o Amylase – converting starch into glucose and fructose Lysozymes – prevents bacterial infections in the mouth Histatins – prevents fungal infections Secretory Ig. A – immunity mediator Lactoperoxidases – stimulation of minor salivary glands RNase and Dnase – cellular maintenance Lipase – initiates digestion of fat Kallikrein – vasoreactive substances
XEROSTOMIA Cellular Composition of Saliva 3 The cellular composition consists of: o o Epithelial cells Neutrophils Lymphocytes Bacterial flora
XEROSTOMIA: Epidemiology Factors that Affect Salivary Flow n n n Medication Autoimmune disease (Sjogren’s syndrome, lupus)3 Systemic diseases (diabetes, asthma, kidney, sarcoidosis, HIV)3 Stress/anxiety/depression 5 Radiation therapy to the head and neck 3 u u n n 30 Gy = glandular fibrosis (gland can still produce some saliva) 60 -70 Gy = glandular destruction (gland can no longer produce saliva) Gender (70 % female, usually postmenopausal 3) Sympathomimetic medications (stimulate the sympathetic nervous system) 6 Parasympatholytic medications (inhibit the parasympathetic nervous system) 6 Circadian rhythms (decreases in the fall and increases in the spring)
Category of Xerogenic medications and Examples Antianxiety (hydroxyzine, diazepam, lorazepam) n Anticholinergic (dicyclomine, mepenzolate) n Anticonvulsant (felbamate, gabapentin) n Antidepressant n u Tricyclic (amitriptyline, imipramine, doxepin, desipramine u SSRI (sertraline, paroxetine, fluoxetine) n n Antiemetic (meclizine, bucilzine) Antihistamine (fexofenadine, azelastine, loratadine)
Category of Xerogenic medications and Examples Antihypertensive (clonidine, methyldopa, prazosin) n Antiparkinsonian (biperiden, selegiline) n Antipsychotic (clozapine, chlorpromazine) • Bronchodilator (ipratopium, albuterol, metaproterenol) • Cholesterol reducing ( n
Category of Xerogenic medications and Examples • • Decongestant (pseudoephedrine) Diet pills Diuretic (spironolactone, chlorothiazide, furosemide) Hormonal replacement therapy Muscle relaxant (cyclobenzaprine, baclofen) Narcotic analgesic (meperidine, morphine) Sedative (flurazapam, triazolam, temazepam)
XEROSTOMIA: Epidemiology Factors that Affect Salivary Flow Age 2, 8 o o Studies show that among non-institutionalized people not taking medication, neither the quantity or quality of saliva change significantly with age Studies show a positive correlation between the number of drugs taken and the incidence and severity of xerostomia
XEROSTOMIA: Etiology “Dry Mouth” Xerostomia is the term used for the symptom of oral dryness. While oral dryness is most commonly associated with a reduction in salivary gland output (termed salivary gland hypofunction), the symptom may be reported by patients with apparently normal salivation who have changes in saliva composition. 1
XEROSTOMIA: Etiology Prevalence Xerostomia affects 25% of the population and is becoming one of the fastest-growing oral health problems in North America 3, 5 n n n Medications are the cause of more than 90% of xerostomia cases 32 million Americans today take three or more medications daily Xerostomia was not a great problem in the past because people did not take as many medications as they do today 5
XEROSTOMIA: Etiology Global Prevalence The reported prevalence of dry mouth varies widely due to the methodological and population differences in various studies. Prevalence has been estimated to range from 10% to 38%, 9 -12 with 20% the most commonly reported figure 2, 3 Xerostomia is becoming increasingly common in developed countries where adults are living longer and poly-pharmacy is very common. 13
XEROSTOMIA: Diagnosis “The approach to managing the patient has to follow a logical progression. It should be part of a comprehensive evaluation. Symptoms should be noted and signs should be recognized in order to properly diagnose the condition. Treatment should be based on all of that gathered information. ” 5 – Joseph L. Perno, DDS, FAGD
XEROSTOMIA: n Reduced saliva whether qualitatively or quantitatively , may negatively impact oral health u Saliva of patients with xerostomia becomes more viscous and foamy, losing its lubricating ability and adhereing to teeth amd mucous membranes. u This thick saliva causes food and bacteria to adhere to teeth, resulting in plaque buildup leading to periodontal disease. u It is the decline in mucin production that results in xerostomia.
XEROSTOMIA: Diagnosis Symptoms 3, 5 n n n n n Viscous saliva Sticky saliva Difficulty speaking Difficulty swallowing Halitosis Altered taste Complaint of dryness Complaint of burning mouth, lips, or tongue Altered sense of smell
XEROSTOMIA: Diagnosis Signs 3, 5 n n n Increased caries Food sticking to the oral structures Frothy saliva Gingivitis Absence of saliva Cracking and fissuring of the tongue Ulceration of oral mucosa No pooling of saliva in the floor of the mouth Recurrent candidal infections A toothbrush, mouth mirror, or instrument that sticks to the soft tissues Poorly fitting prostheses
XEROSTOMIA: Diagnosis Increase Salivary Flow • • Two Approaches Using drugs that mimic or stimulate the parasympathetic division of the autonomic nervous system 3 o These are typically only used for radiation therapy or Sjogrens’ syndrome -induced xerostomia o They have adverse side effects including: sweating, urination, stuffy nose, lacrimation, and abdominal pain. Using citric acid–containing lozenges and candy that are sugar-free 1, 5 o This approach may decrease the p. H into an acidic range. Salivary p. H is between 6. 0 and 7. 0. The critical p. H where enamel erosion begins to be seen is reported to be below 5. 5 Saliva Substitutes • Over-the-counter products are indicated for medication-induced salivary hypofunction or xerostomia 3, 5
XEROSTOMIA: Diagnosis Simple Management Strategies for Patients 3, 14 n Perform oral hygiene at least 4 times daily, after each meal and before bedtimes n Use fluoride toothpaste n Rinse with a salt and baking soda solution 4 to 6 times daily n Avoid citrus juices (oranges, grapefruit, tomatoes) n Rinse and wipe oral cavity immediately after meals n Keep water handy to moisten the mouth at all times n Avoid liquids and foods with high sugar content n Avoid rinses containing alcohol and salty foods n Brush and rinse dentures after meals n Apply prescription-strength fluoride get at bedtime as prescribed n Use moisturizers regularly on the lips n Try salivary substitutes or artificial saliva preparations
XEROSTOMIA: Management Treatment Challenges 14 Some patients are predisposed to candidiasis because of the lack of salivary histatins n Recommendation: o Antifungal medication can be recommended to control fungal growth Denture patients also face challenges n o Dentures do not adhere to the tissues and are not retained as well o Lack of lubrication increases the frictional forces between the dentures and the oral mucosa, causing sores o Alveolar bone continues to resorb throughout life―dentures no longer fit properly o Denture wearers are prone to inflamed tissues, called denture stomatitis (usually fungal) Recommendation: o Be sure the denture correctly adapts to the denture-bearing tissues o Optimize the patient’s tissue health o Apply oral lubricants or saliva substitutes just before eating
XEROSTOMIA: Management Treatment of Xerostomia-Associated Problems 14
XEROSTOMIA: Management Treatment of Xerostomia-Associated Problems 14
XEROSTOMIA GETTING INVOLVED IN DIAGNOSING XEROSTOMIA CAN BE A WINDOW TO YOUR PATIENTS’ OVERALL HEALTH Diagnosing xerostomia is an important diagnostic tool for other systemic diseases. The signs and symptoms of xerostomia are often associated with and/or result from other conditions.
XEROSTOMIA: References 1. Fox PC. Dry mouth: managing the symptoms and providing effective relief. J Clin Dent. 2006; 17(2): 27 -29. 2. Nederfor T. Xerostomia: Prevalence and pharmacotherapy. Wed Dent J Suppl 116: 1 -70, 1996 3. Crossley H. Unraveling the mysteries of saliva: its importance in maintaining oral health. Transcript of a lecture presented on August 6 at the 2006 AGD Annual Meeting & Exposition. Gen Dent. 2007; 55)4): 288 -296. 4. Netter FH, Jansen JT. Atlas of Human Anatomy. 3 rd ed. Teterboro, NJ: Icon Learning Systems; 2003. 5. Gater L. Understanding xerostomia. AGD Impact. 2008; June(Special Report): 26 -30. 6. Urquhart D, Fowler CE. Review of the use of polymers in saliva substitutes for symptomatic relief of xerostomia. J Clin Dent. 2006; 17(2): 2933. 7. Kroll B. Dry mouth. The pharmacist’s role in managing radiation-induced xerostomia. Pharma Pract. 1998; 14: 72 -82. 8. Shirodaria S, Kilbourn T, Richardson M. Subjective assessment of a new moisturizing mouthwash for symptomatic management of dry mouth. J Clin Dent. 2006; 17(2): 45 -51. 9. O’Grady NP: Incidence of dry mouth complaint in Cork Dental Hospital population. Stoma (Lisb). 1990; 2(17): 55 -56, 58. 10. Osterberg T, Birkhed D, Johnannson C, Svanborg A. Longintudinal study of stimulated whole saliva in an elderly population. Scand J Dent Res. 1992; 100(6): 340 -345. 11. Thomson WM, Brown RH, Williams SM. Medication and perception of dry mouth in a population of institutionalized elderly people. NZ Med J 106: 219 -221, 1993 12. Locker D: Xerostomia in older adults: A longitudinal study. Gerodontology. 12: 18 -25, 1985. 13. Edgar WM, O’Mullane DM. Saliva and Oral Health. 2 nd ed. London: British Dental Journal Brooks; 1996. 14. Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc. 2009; 138(September–Special Supplement): 15 S-20 S.
XEROSTOMIA This IFDEA Educational Teaching Resource was underwritten by an unrestricted grant from: