The Adrenal Glands Part The Adrenal Cortex Ziying












 protein • St. AR deficiency: lipid")



 Serum")

 axis")






 (glucose + cortex + steroid)")



 Effects on carbohydrate metabolism: BS↑ a. increase glyconeogenesis b.")
 Effects on protein metabolism a. stimulates protein catabolism b.")
 Effects on lipid metabolism: a. stimulate lipolysis b. cause")
 Effects on salt and water metabolism • • a.")






 94, (557– 572) (Printed in Great Britain)")
 Inhibiting phagocytosis and management of macrophages")
membrane stabilization:")
 anti-inflammatory and anti-toxic effects 2)directly relaxing")

 Stimulating hemopoiesis: RBC, PLT , Hb↑ (2) Neutrophils")
 Central nervous system: excitation (2) Digestive system: excitation (3) Skin")

")



 • Deficiency of biosynthesis enzyme")


 Basic test: Serum levels of cortisol")





 CBG: Liver,")


Severe acute bacterial infections Eg: fulminant epidemic meningitis(暴发性流脑), toxic")
 Some virus infection Eg. severe infective hepatitis epidemic")
 Prevention for inflammatory sequela (1) tuberculous diseases: Eg.")
 Autoimmune diseases: used widely rheumatic fever, rheumatic or")
 Organ transplantation: Combined with immunosupressive agents 3)Allergic diseases:")
infectious-toxic shock : first choice 2)other")
Blood disorders acute lymphatic leukemia, aplastic anemia (AA), thrombocytopenia, granulocytopenia")



 Latrogenic adrenocortical insufficiency : adrenocortical atrophy adrenal crisis 2) Rebound")

 Substitution therapy with small dose 2) Impact therapy with large")
- Slides: 80
The Adrenal Glands PartⅡ: The Adrenal Cortex Ziying WANG Institute of Pharmacology School of Medicine, Shandong University wangziying@sdu. edu. cn
Part 1 Introduction More important than adrenal medulla
Adrenal and their hormones mineralocorticoid Adrenal cortex glucocorticoids sex hormones AD NE
a Tissue section of adrenal cortex
Capsule Cortex Parenchyma Medulla
Electron micrograph Zona glomerulosa Zona fasciculata
Part 2 Hormones produced by the adrenal cortex Belong to steroid hormones
Basic Structure of Adrenocortical Hormones 11 C O A 4 B 5 CH 2 OH 20 c 18 R 3 21 17 D o OH Basic structure: Steroid nucleus C 3 = 0 (酮基) C 4 -5 (双键) C 20 =0 (羰基) are necessary for adrenocortical hormones
Hormones of adrenal cortex
Case: 4 -year-old girl Report from her mother • • Height and weight lower than expected Ambiguous genitalia Public hair developed from 3 BP: 70/30 mm. Hg(↓) Blood test • • • Serum sodium: 127 mmol/L(↓) Serum potassium: 5. 4 mmol/L (→) Serum cortisol: 128 nmol/L(↓) Serum ACTH: 55 ng/L(↑) Plasma renin activity: 1242 Pmol/L/h (↑) Serum 17 -hydroxyprogesterone: 76 nmol/L (↑ ↑ ↑)
Steroid biosynthesis • From cholesterol • Hydroxylation reactions: CYP 450 family • Rate-limiting enzyme: CYP 11 A 1
Steroid biosynthesis CYP 11 A 1 CYP 21
Steroid biosynthesis • St. AR: (steroidogenic acute regulatory) protein • St. AR deficiency: lipid adrenal hyperplasia
Raw material: cholesterol • Release: from lipid droplets St. AR protein phosphorylation Cholesterol ester hydrolase • Source De novo synthesis From LDL • Stimulated by ACTH
Do novo synthesis of cholesterol 乙酰Co. A 乙酰乙酰Co. A HMG-Co. A还原酶 HMG-Co. A MVA 鲨烯 胆固醇
Defects of steroid biosynthesis • Congenital adrenal hyperplasia • 21 -hydroxylase encoded by CYP 21 deficiency
Case: Establishing the diagnosis Blood test • • • Serum sodium: 127 mmol/L(↓) Serum potassium: 5. 4 mmol/L (→) Serum cortisol: 128 nmol/L(↓) Serum ACTH: 55 ng/L(↑) Plasma renin activity: 1242 Pmol/L/h (↑) Serum 17 -hydroxyprogesterone: 76 nmol/L (↑ ↑ ↑)
Part 3 Regulation of steroid production
Cortisol: HPA (hypothalamicpituitary-adrenal cortex) axis
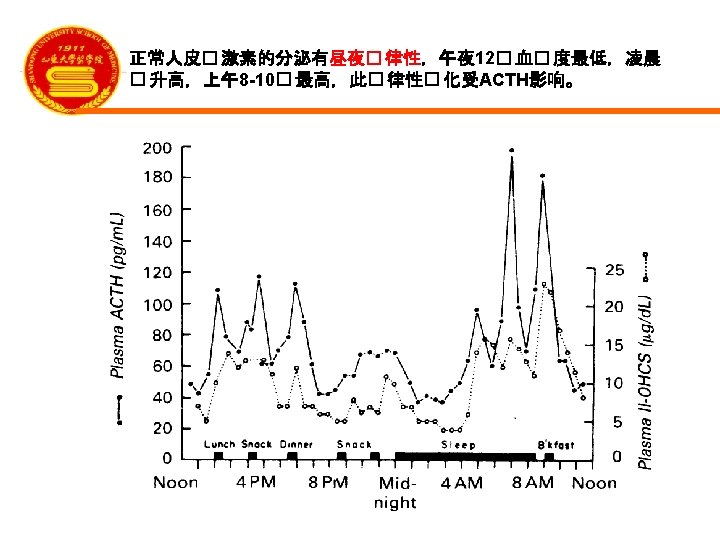
ACTH : diurnal variation
The actions of ACTH • • • 1. Increase adrenal blood flow 2. Increase steroidogenic enzyme expression 3. Activate St. AR protein 4. Activate cholesterol ester hydrolase 4. Increase the size of adrenal gland
Molecular mechanism of ACTH: G-protein coupled receptor
Case: Explanation of plasma ACTH result Blood test • • • Serum sodium: 127 mmol/L(↓) Serum potassium: 5. 4 mmol/L (→) Serum cortisol: 128 nmol/L(↓) Serum ACTH: 55 ng/L(↑) Plasma renin activity: 1242 Pmol/L/h (↑) • Serum 17 -hydroxyprogesterone: 76 nmol/L (↑ ↑ ↑)
Aldosterone: the renin-angiotensin system
Part 4 Actions of adrenal steroids Glucocorticoids Mineralocorticoids Adrenal androgens
Actions of glucocorticoids (GCS) (glucose + cortex + steroid)
Molecular mechanism of GCS Glucocorticoid receptor Functional structure of the glucocorticoid receptor. The glucocorticoid receptor protein has 3 domains: the amino terminus, the DNA binding domain (DBD), and the carboxyl terminus for hormone binding. Two zinc fingers are located in the central region. There also phosphorylation sites and regions of hormone-independent activation function (AF 1) and hormone-dependent activation function (AF 2) related to transcription.
Molecular mechanism of GCS Glucocorticoid receptor Signaling
Actions of GCS 1. Effects on metabolism 2. Permissive action 3. Anti-inflammatory effects 4. Immunosuppressive and anti-allergic effects 5. Anti-toxic effects 6. Anti-shock effects 7. Effects on blood and hematopoietic system 8. Other effects
1. Effects on metabolism (1) Effects on carbohydrate metabolism: BS↑ a. increase glyconeogenesis b. increase glycogenolysis c. decrease the oxidation and utilization of glucose • Net result: hyperglycemia
1. Effects on metabolism (2) Effects on protein metabolism a. stimulates protein catabolism b. inhibit protein synthesis Net result: negative nitrogen balance
1. Effects on metabolism (3) Effects on lipid metabolism: a. stimulate lipolysis b. cause dramatic redistribution of body fat. Result: concentric obesity
1. Effects on metabolism (4) Effects on salt and water metabolism • • a. mineralocorticoids-like activity: weak b. antagonizing Vitamin D
2. Permissive action Definition: GCS facilitates other hormonal effects other than direct effects. eg. Increase the vasoconstriction of CA, increase the hyperglycemic effect of glycagon
3. Anti-inflammatory effects Characteristics: rapid, strong , nonspecific , both the early phase and late phase
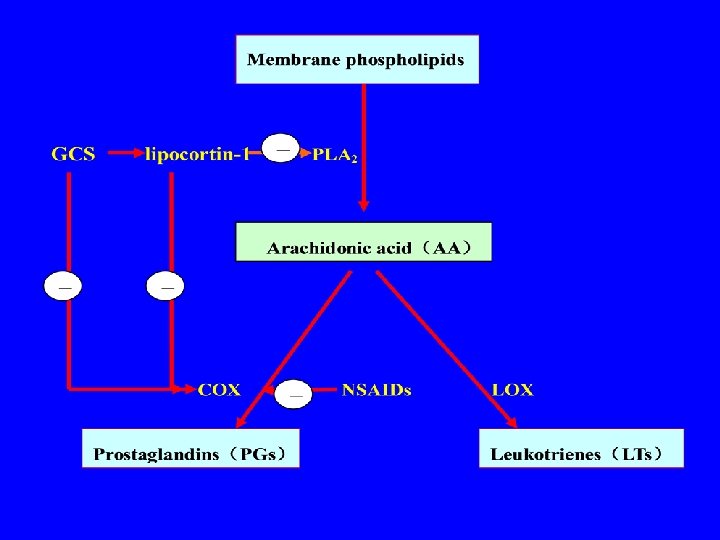
Mechanism of anti-inflammatory action ⅠReducing the vascular response of inflammation a. Affecting AA metabolism→ PGs , LTs↓ (inducing lipocortin-1, inhibiting COX) b. Inhibiting i. NOS expression→ NO ↓ c. Inducing ACE→ BK↓ d. Increasing the vasoconstriction of CA
Mechanism of anti-inflammatory action L-Arginine i. NOS NO GCS + BK ACE Degradation production
Mechanism of anti-inflammatory action Ⅱ. Reducing the cell response to inflammation a. Inhibiting some pro-inflammatory cytokines expression (eg. IL-1, 2, 5, 6, 8, TNF-α) b. Inducing some anti-inflammatorycytokines expression (eg. IL-10, IL-12, IκB 1). c. Inhibiting adhesion molecule expression (eg. ICAM-1, E-selectin). d. Inducing inflammatory cells apoptosis : inducing caspase and endonuclease
Mechanism of anti-inflammatory action Ⅲ. Postponing the inflammatory sequela Mechanism: inhibiting hyperplasy of blood capillary and fibroblast, preventing adhesion and scar formation
Molecular mechanism of anti-inflammatory Clinical Science (1998) 94, (557– 572) (Printed in Great Britain) Antiinflammatory actions of glucocorticoids: molecular mechanisms
2. Immunosuppressive effects and anti-allergic effects Mechanisms 1) Inhibiting phagocytosis and management of macrophages on antigen 2) Promoting the redistribution of lymphocyte in human blood, decreasing the number of lymphocytes in circulation 3) Inhibiting IL-1 mediated immunoreactions 4) Stabilizing mast cell membrane
3. Antitoxic effects Mechanism: enhancing body tolerance to bacterial endotoxin Antipyretic mechanism: 1)membrane stabilization: endogenous pyrogens release ↓ 2)decreasing the sensitivity of body temperature regulating center to endogenous pyrogens.
4. Anti-shock effects: especially infectious-toxic shock Mechanisms: 1) anti-inflammatory and anti-toxic effects 2)directly relaxing the spasmodic vessels and enhancing the contractility of myocardium 3) reducing the sensitivity of some vasoconstrictive substances on vessels 4) membrane stabilization, MDF production and release↓ (MDF: myocardial-depressant factor)
shock ischemia hypoxia acidosis vicious cycle lysosomal membrane disruption - Release of proteinase plasma protein Myocardial depression MDF vasospasm GCS
5. Effects on blood system (1) Stimulating hemopoiesis: RBC, PLT , Hb↑ (2) Neutrophils : number ↑, function↓ (3) Other blood cells: ↓ ( lymphocytes, basophilic , eosinophile granulocytes )
6. Other effects (1) Central nervous system: excitation (2) Digestive system: excitation (3) Skin and bone ① relieving itching ② anti-hyperplasy ③ osteoporosis
The effects of GCS in stress 1. Stress 2. Stress hormone is increased 3. Cortisol is an essential part of the body’s response to stress.
Actions of mineralocorticoids (mineral+ cortex + steroid)
Actions of mineralocorticoids 11 -HSD: 11βhydroxysteroid dehydrogenase AME: apparent mineralocorticoid excess
Actions of adrenal androgens In disease states Virilizing effects Can be converted to estrogens
Part 5 Disorders of adrenal steroids Congenital adrenal hyperplasia Glucocorticoid excess Mineralocorticoid excess Adenal insufficiency
Congenital adrenal hyperplasia (CAH) • Deficiency of biosynthesis enzyme
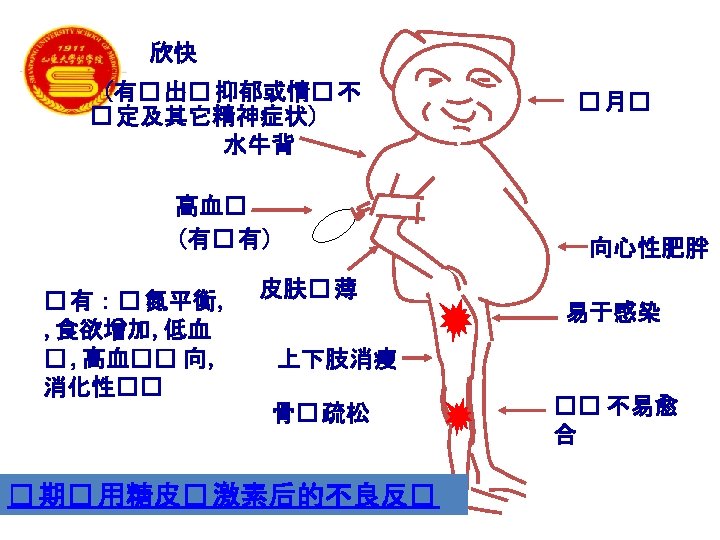
Glucocorticoid excess: Cushing’s syndrome Causes • • 1. Exogenous corticosteroid administration 2. Cushing’s disease 3. Adrenal adenoma 4. Ectopic ACTH production
Glucocorticoid excess: Cushing’s syndrome
Investigations of GCS excess 1. Blood test (1) Basic test: Serum levels of cortisol and ACTH (2) Dynamic test: Dex suppression test 2. Image examination: CT and MRI
Mineralocorticoid excess: Conn’s syndrome Causes • 1. Aldosterone-secreting adrenal adenoma • 2. Idiopathic hyperaldosteronism Sympotoms: • hepertension and hypokalaemia Treatment: ADS receptor blockers
Adrenal insufficiency Seconary Hypothalamus • • pituitary • Primary : adrenal cortex
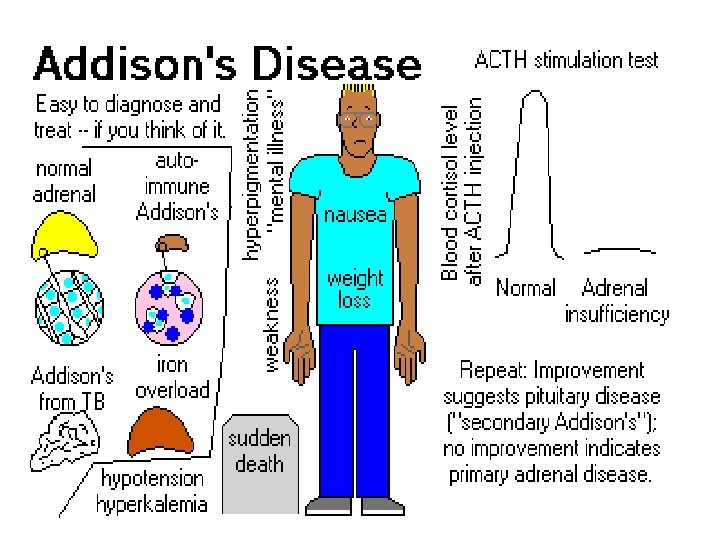
Adrenal insufficiency Acute: Water-house Friderichsen syndrome adrenal crisis ablation of bilateral adrenal glands Chronic: Addison’ s disease (primary) hypofunction of hypothalamus or pituitary (secondary)
Adrenal crisis
Pharmocological uses of GCS Drugs hydrocortisone prednisone prednisolone methylprednisolone dexamethasone betamethasone fludrocortisone fluocinolone Metabolism on electrolyte carbohydrate and water (rate) 1. 0 0. 8 0. 6 0. 5 0. 1 125 > 100 1. 0 0. 8 3. 5 4. 0 11 20 11 10 ~ Antiinflammation (rate) 1. 0 0. 8 3. 5 4. 0 5. 0 30 25~ 35 12 40
Pharmacokinetics of GCS Absorption Distribution: PPBR>90% 80% : corticosteroid binding globulin (CBG) CBG: Liver, estrogen 10%: albumin Metabolism: liver cortisone →hydrocortisone prednisone → prednisolone Excretion: kidney
Pharmocological uses of GCS • • 1. Replacement therapy 2. Severe infection and inflammation 3. Autoimmune and allergic diseases 4. Shock 5. Others (1) blood disorder (2) topical use (3) cancer
1. Replacement therapy: in small dose Primary/secondary, acute/chronic adrenal cortex hypofunction Acute: Water-house Friderichsen syndrome adrenal crisis ablation of bilateral adrenal glands Chronic: Addison’ s disease (primary) hypofunction of hypothalamus or pituitary (secondary)
2. Severe infection and inflammation 1)Severe acute bacterial infections Eg: fulminant epidemic meningitis(暴发性流脑), toxic bacillary dysentery(中毒性菌痢), toxic pneumonia, scarlet fever, acute miliary tuberculosis of lung, septicemia(败血症) large-dose , short-term treatment of GCS may help patients go through dangerous stage. Attention: must be used plus enough effective antibacterial agents. (why? )
2. Severe infection and inflammation 2) Some virus infection Eg. severe infective hepatitis epidemic parotitis (流行性腮腺炎) measles (麻疹) Japanese B encephalitis (乙脑) SARS
2. Severe infection and inflammation 3) Prevention for inflammatory sequela (1) tuberculous diseases: Eg. meningitis, pleuritis(胸膜炎), pericarditis(心包炎) (2) ocular diseases: iritis(虹膜炎), keratitis(角膜炎), retinitis(视网膜炎)
3. Autoimmune and allergic diseases 1) Autoimmune diseases: used widely rheumatic fever, rheumatic or rheumatoid arthritis rheumatic myocarditis systemic lupus erythematosus (SLE), autoimmune hemolytic anemia nephrotic syndrome
3. Autoimmune and allergic diseases 2) Organ transplantation: Combined with immunosupressive agents 3)Allergic diseases: bronchial asthma, urticaria(荨麻疹), hay fever, anaphylactic rhinitis(过敏性鼻炎) be given as supplements to the primary therapy
4. Shock effective to all kinds of shock 1)infectious-toxic shock : first choice 2)other shocks: supplements
5. Other clinical uses (1)Blood disorders acute lymphatic leukemia, aplastic anemia (AA), thrombocytopenia, granulocytopenia (2) Topical uses : local therapy some skin diseases some ocular diseases (3) Some cancers
Adverse reactions caused by continuous and longtime use of large doses of GCS Withdrawl reactions: adverse reactions caused by sudden withdrawl after a continuous and longtime use.
1. Adverse reactions caused by continuous and longtime use of large doses of GCS 1) Latrogenic(医源性) Cushing’s syndrome 2) Induction and aggravation of infection 3) Possible risk of peptic ulcers 4) Cardiovascular complications:HBP, AS 5) Other complications a. osteoporosis b. psychosis, euphoria c. growth retardation d. glaucoma:GIG e. abnormity
Abnormity
2. Withdrawal reactions 1) Latrogenic adrenocortical insufficiency : adrenocortical atrophy adrenal crisis 2) Rebound phenomenon
Contraindications Severe psychosis and epilepsy active peptic ulcer restore period of fracture and wound corneal ulcer severe hypertension diabetes pregnancy uncontrolled infection
Methods of application 1) Substitution therapy with small dose 2) Impact therapy with large dose 3) Long-term therapy with moderate dose (1) Therapy on every morning (2) Therapy on every other morning