Scleroderma and Inflammatory Myositis Kathryn Dao MD Arthritis




![DDX of Tight Skin n n Pseudosclerodactyly ] IDDM, Hypothyroidism Drugs: Tryptophan, bleomycin, pentazocine,](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-6.jpg "DDX of Tight Skin n n Pseudosclerodactyly ] IDDM, Hypothyroidism Drugs: Tryptophan, bleomycin, pentazocine,")
 Scleroderma-like conditions Eosinophil myalgia syndrome")
![ACR Systemic Sclerosis Preliminary Classification Criteria* n Major Criterion ] Proximal n Scleroderma Minor](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-8.jpg "ACR Systemic Sclerosis Preliminary Classification Criteria* n Major Criterion ] Proximal n Scleroderma Minor")


![Scleroderma A disorder of Collagen, Vessels ] ] n Small to medium-sized blood vessels,](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-11.jpg "Scleroderma A disorder of Collagen, Vessels ] ] n Small to medium-sized blood vessels,")






![Scleroderma Renal Crisis n Risk Factors ] diffuse skin involvement ] rapid progression of](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-23.jpg "Scleroderma Renal Crisis n Risk Factors ] diffuse skin involvement ] rapid progression of")










![DDX MYOPATHIIES n Toxic/Drugs ] n Infectious ] n n n Etoh, Cocaine, Steroids,](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-39.jpg "DDX MYOPATHIIES n Toxic/Drugs ] n Infectious ] n n n Etoh, Cocaine, Steroids,")
![NONMYOPATHIC CONSIDERATIONS n Fibromyalgia/Fibrositis/Myofascial n n Pain disorder Polymyalgia Rheumatica ] Caucasians, > 55](https://slidetodoc.com/presentation_image/0aff954a635d8b9be45431ecb1571192/image-40.jpg "NONMYOPATHIC CONSIDERATIONS n Fibromyalgia/Fibrositis/Myofascial n n Pain disorder Polymyalgia Rheumatica ] Caucasians, > 55")
 & monocytes")








, Neurologic Exam Acute")
 Call the neuropathologist! 85%")







 n")




- Slides: 64
Scleroderma and Inflammatory Myositis Kathryn Dao, MD Arthritis Center February 16, 2006
Scleroderma “Skleros-” = hard “-derma” = skin n Incidence 1 -2/100, 000 in USA n Peak age of onset 30 -50 y. o. n Female: male 7 -12: 1 n Disease manifestation is a result of host factors + environment (concordance is similar in monozygotic and dizygotic twins) n
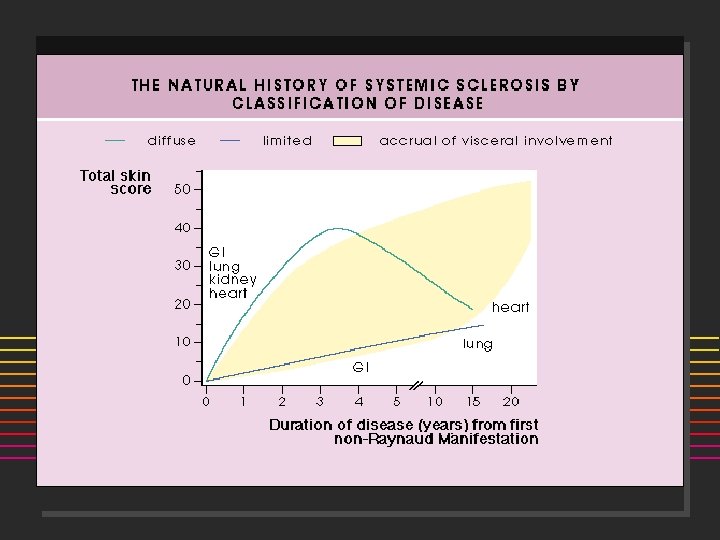
Scleroderma Three major disease subsets: based on extent of skin dz n Localized Scleroderma Morphea: manifests as focal patches ] Linear scleroderma: band-like (linear) areas of thickening. (Coup de Sabre) ] n Limited disease AKA "CREST" syndrome ] n n Calcinosis, Raynauds, Esophageal dysmotility Sclerodactyly, Telangiectasias Diffuse disease - skin abnormalities extending to the proximal extremities (AKA - PSS) (Scleroderma sine scleroderma)
DDX of Tight Skin n n Pseudosclerodactyly ] IDDM, Hypothyroidism Drugs: Tryptophan, bleomycin, pentazocine, vinyl chloride, solvents Eosinophilic fasciitis Overlap syndromes Scleredema
DDX of Tight Skin n n Scleromyxedema (popular mucinosis) Scleroderma-like conditions Eosinophil myalgia syndrome (tryptophan) ] Porphyria cutanea tarda ] Toxic oil syndrome ] Nephrogenic fibrosing dermopathy ]
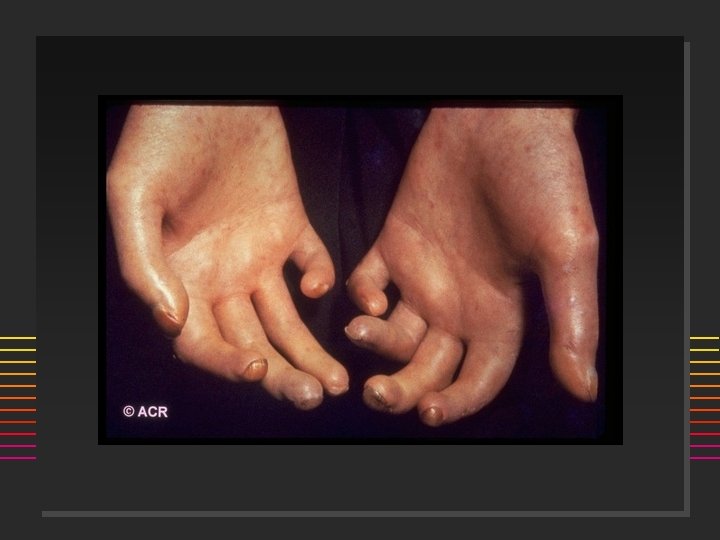
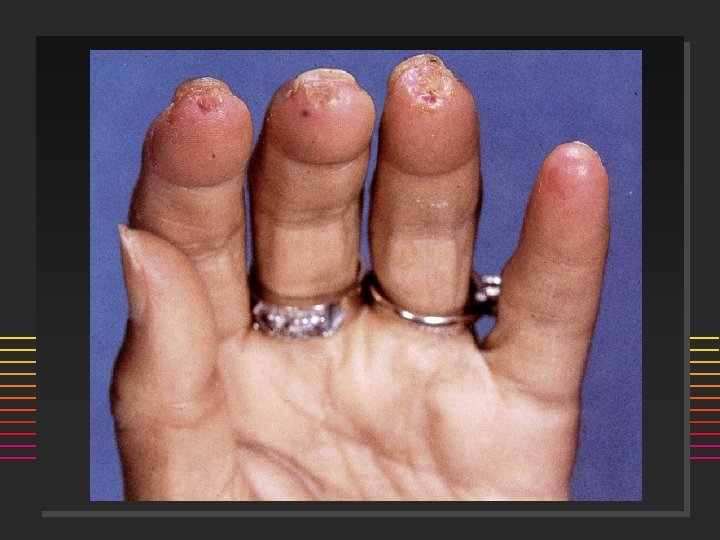
ACR Systemic Sclerosis Preliminary Classification Criteria* n Major Criterion ] Proximal n Scleroderma Minor Criteria ] Sclerodactyly ] Digital pitting or scars or loss of finger pad ] Bibasilar pulmonary fibrosis * One major and two minor required for diagnosis
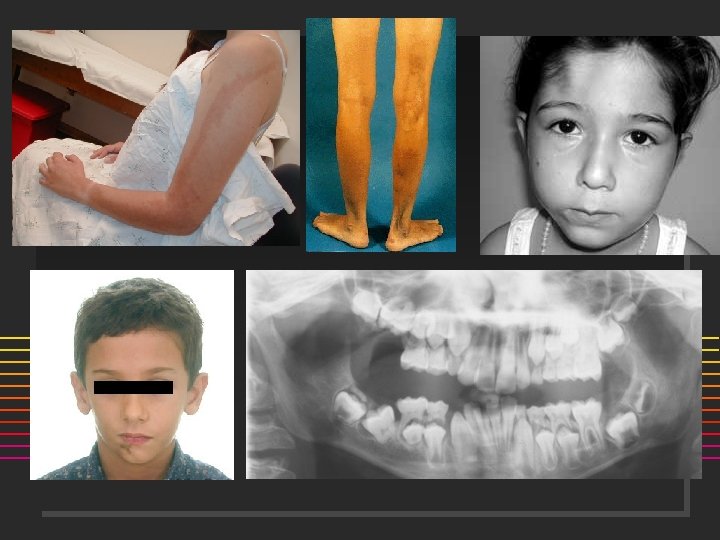
Scleroderma: Onset n n n Raynauds Swollen or puffy digits Loss of skin folds, no hair growth Digital pulp sores/scars Arthralgias >> Arthritis
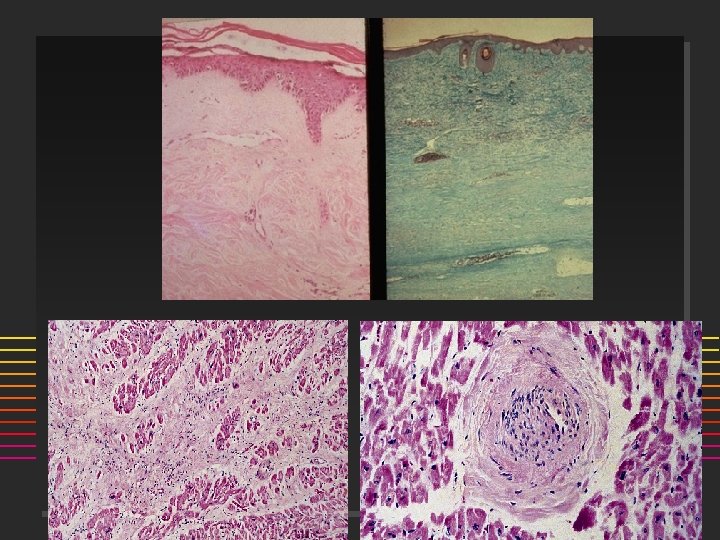
Scleroderma A disorder of Collagen, Vessels n n n Etiology: unknown? Autoimmune disorder suggested by the presence of characteristic autoantibodies such as ANA, anti-centromere and anti-SCL-70 antibodies. Pathology: ] Early dermal changes lymphocytic infiltrates primarily of T cells ] Major abnormality is collagen accumulation with fibrosis.
Scleroderma A disorder of Collagen, Vessels ] ] n Small to medium-sized blood vessels, which show bland fibrotic change Vasculopathy, NOT vasculitis! Small thrombi may form on the altered intimal surfaces. Microvascular disease Cold Normal PSS
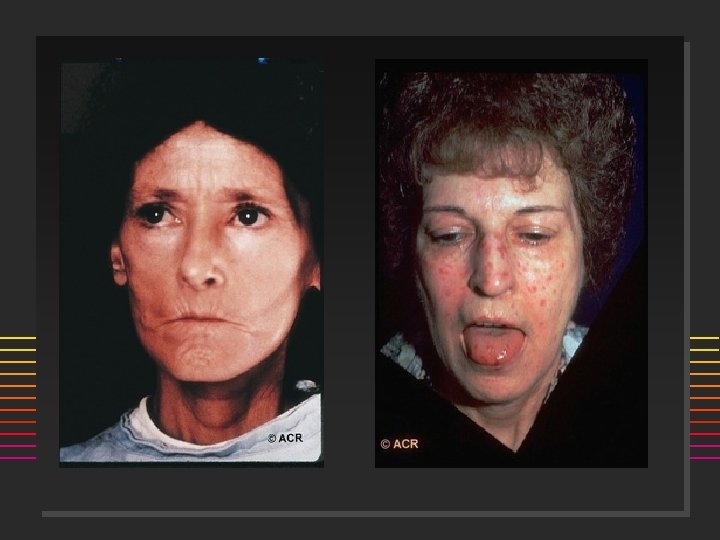
PSS - Clinical n Skin: Skin thickening is most noticeable in the hands, looking swollen, puffy, waxy. ] Thickening extends to proximal extremity, truncal and facial skin thickening is seen. ] Raynaud's phenomenon is present. ] Digital pits or scarring of the distal digital pulp ] n Musculoskeletal: Arthralgias and joint stiffness are common. Palpable tendon friction rubs associated with an increased incidence of organ involvement. ] Muscle weakness or frank myositis can be seen. ]
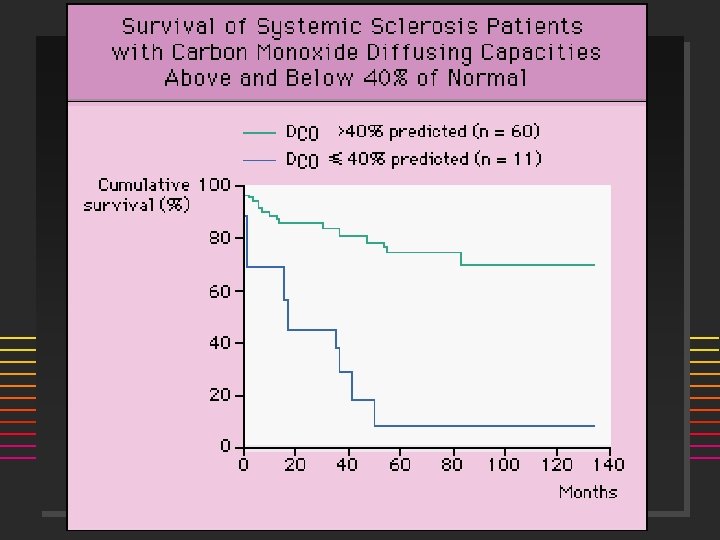
Skin Scores Extent of skin involvment predictive of survival: J Rheumatol 1988; 15: 276 -83. % Survival at 5 yr 10 yr Sclerodactyly 79 -84 47 -75 Truncal 48 -50 22 -26
PSS - Clinical n Gastrointestinal: Esophageal dysmotility, dysphagia, malabsorptive or blind loop syndrome, constipation.
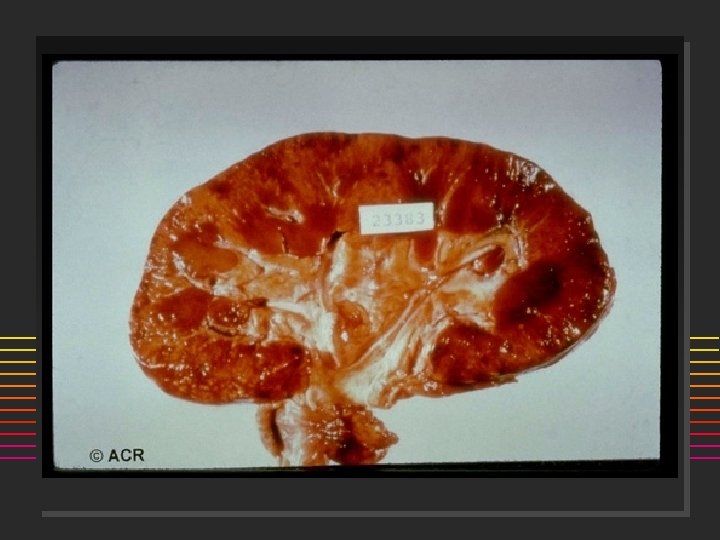
Renal: Kidney involvement is an ominous finding and important cause of death in diffuse scleroderma. A hypertensive crisis (AKA renal crisis) may herald the onset of rapidly progressive renal failure.
Scleroderma Renal Crisis n Risk Factors ] diffuse skin involvement ] rapid progression of skin thickening ] disease course < 4 years ] anti-RNA-polymerase III-antibodies ] newly manifested anemia ] newly manifested cardiac involvement äpericardial effusion äheart insufficiency preceded high-dose corticoid therapy ] pregnancy ] Am J Med 1984; 76: 779 -786.
Scleroderma Renal Crisis n n n Microangiopathic hemolytic anemia +Microscopic hematuria Fatal before the introduction of ACE-I, CCB ] Survival without ACE-I 16% @ 1 year, with ACE-I 45% at 5 years Continue use of ACE-I even if dialysis appears imminent Ann Int Med 1990; 113: 352 -357.
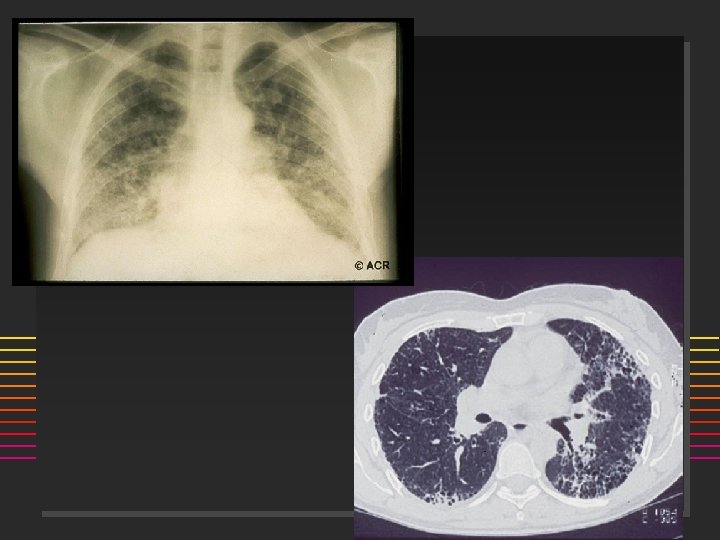
Pulmonary Manifestations of PSS n n n Dyspnea Pulmonary HTN primarily in CREST Ground glass (alveolitis) Interstitial fibrosis (bibasilar) High resolution CT vs Gallium Scan ] n Major cause of death RARE: Pulmonary embolism ] Pulmonary vasculitis ]
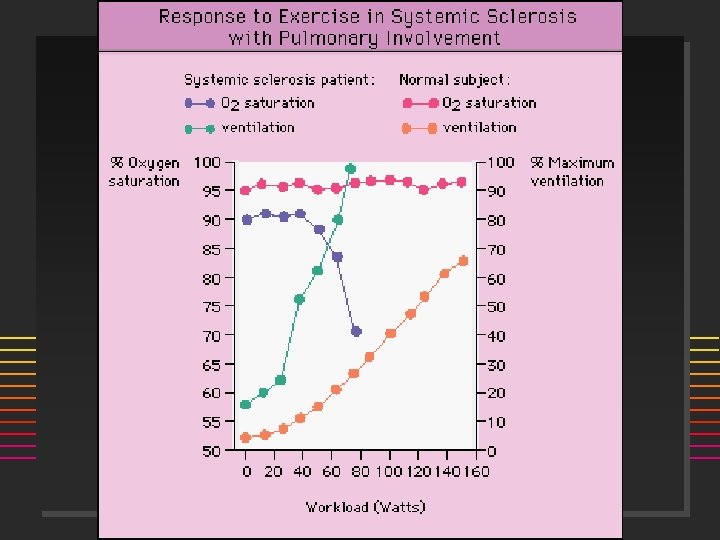
PFT’s in Systemic Sclerosis Decreased DLCO is the Earliest Marker n Increased A-a Gradient with Exercise n Restrictive Pattern n ] n VC, FEV 1/FVC Pulmonary Vascular Disease ] DLCO with Normal Volumes
Cardiac Findings in PSS Myocardial fibrosis n Dilated cardiomyopathy n Cor pulmonale n Arrhythmias n Pericarditis n Myocarditis n Congestive heart failure n Myocardial infarction (Raynaud’s) n
Comparison CREST v. PSS Feature Calcinosis Limited CREST ++ Diffuse PSS + Arthralgia/Arthritis Pulmonary fibrosis Pulmonary HTN ++ ++ ++ ++++ + Tend friction rubs Renal crisis Centromere Ab Anti-Scl 70 Ab Raynaud’s 0 0 +++ + +++++ + +/0 ++ +++++ Telangiectasia +++++ Esophageal dysmotility +++++ 5 yr Survival +++++ + Relative percentages: +++++ 81 -100%; ++++ 61 -80%; +++ 41 -60%; ++ 21 -40%; + 1 -20%
Treatment of Scleroderma Localized: none n Raynauds: warmth, skin protection, vasodilator therapy n CREST: same as Raynauds n PSS: none proven n ] No Value: Steroids, Penicillamine, MTX ] Cytoxan: for lung disease? ] Experimental: stem cell transplant, TNF-I – Epoprostenol (Flolan): Prostacyclin – Bosentan (Tracleer): Endothelin receptor antagonist ] Finger ulcers: difficult; vasodilators, Abx
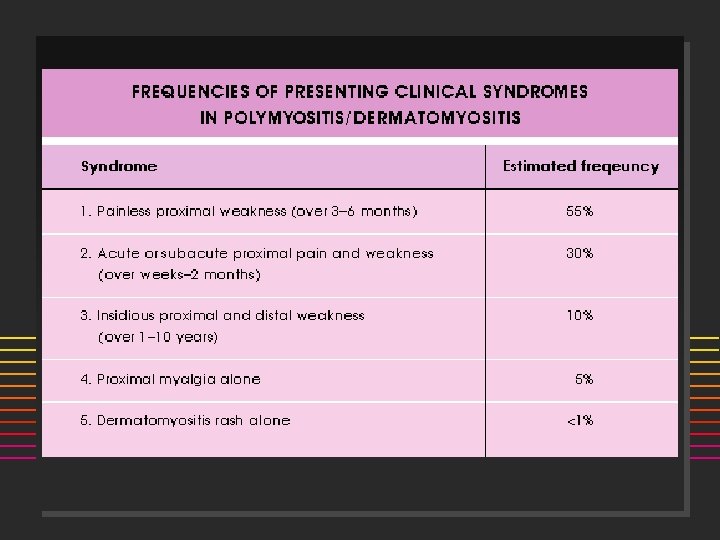
Inflammatory Myositis: Polymyositis/Dermatomyositis n n n n n F: M = 2: 1 Acute onset Weakness (+ myalgia): Proximal > Distal Skeletal muscle: dysphagia, dysphonia Sx: Rash, Raynauds, dyspnea 65% elevated CPK, aldolase 50% ANA (+) 90% +EMG 85% + muscle biopsy
Proposed Criteria for Myositis 1. 2. 3. 4. 5. n n Symmetric proximal muscle weakness Elevated Muscle Enzymes (CPK, aldolase, AST, ALT, LDH) Myopathic EMG abnormalities Typical changes on muscle biopsy Typical rash of dermatomyositis PM Dx is Definite with 4/5 criteria and Probable with 3/5 criteria DM Dx Definite with rash and 3/4 criteria and Probable w/ rash and 2/4 criteria
Polymyositis Classification Bohan & Peter 1. 2. 3. 4. Primary idiopathic dermatomyositis Primary idiopathic polymyositis Adult PM/DM associated with neoplasia Childhood Dermatomyositis (or PM) ä often associated with vasculitis and calcinosis 5. Myositis associated with collagen vascular disease
MYOPATHY: HISTORICAL CONSIDERATIONS n n n n Age/Sex/Race Acute vs. Insidious Onset Distribution: Proximal vs. Distal Pain? Drugs/Pre-existing Conditions Neuropathy Systemic Features
DDX MYOPATHIIES n Toxic/Drugs ] n Infectious ] n n n Etoh, Cocaine, Steroids, Plaquenil, Penicillamine, Colchicine, AZT, Statins, Clofibrate, Tryptophan, Taxol, Emetine Coxsackie, HBV, HIV, Stept, Staph, Clostridium, Toxoplasma, Trichinella Inflammatory Myopathies Congenital/metabolic myopathies Neuropathic/Motor Neuron Disorders-MG, MD Endocrine/Metabolic-hypothyroidism Inclusion body myositis
NONMYOPATHIC CONSIDERATIONS n Fibromyalgia/Fibrositis/Myofascial n n Pain disorder Polymyalgia Rheumatica ] Caucasians, > 55 yrs, M=F ] ESR > 100, normal strength, no synovitis CTD (SLE, RA, SSc) Vasculitis Adult Still's Disease
INFLAMMATORY MYOSITIS Immunopathogenesis n n n n Infiltrates - T cells (HLA-DR+) & monocytes Muscle fibers express class I & II MHC Ags T cells are cytotoxic to muscle fibers t-RNA antibodies: role? FOUND IN <50% OF PTS Infectious etiology? Viral implicated HLA-B 8/DR 3 in childhood DM DR 3 and DRW 52 with t-RNA synthetase Ab
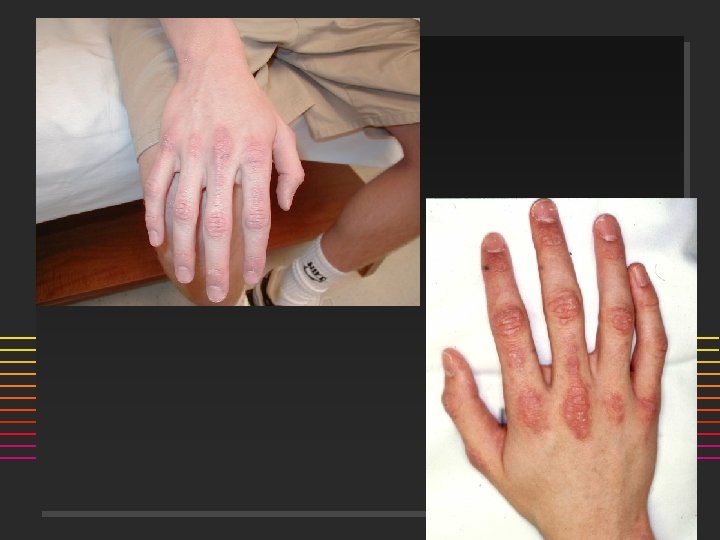
DERMATOMYOSITIS 5 Skin Features 1. Heliotrope Rash: over eyelids n 2. 3. 4. 5. Seldom seen in adults Gottrons Sign/Papules (pathognomonic): MCPs, PIPs, MTPs, knees, elbows V-Neck Rash: violaceous/erythema anterior chest w/ telangiectasias Periungual erythema, digital ulcerations Calcinosis
Why is it called a heliotropic rash?
Calcinosis
DIAGNOSTIC TESTING n n n Physical Examiniation: Motor Strength (Gowers sign), Neurologic Exam Acute phase reactants unreliable Muscle Enzymes ] ] n CPK: elevated >65%; >10% MB fraction is possible Muscle specific- Aldolase, Troponin, Carb. anhydrase. III AST > LDH > ALT Beware of incr. creatinine (ATN) and myoglobinuria EMG: increased insertional activity, amplitude, polyphasics, neuropathic changes, incremental/decremental MU changes
DIAGNOSTIC TESTING n Muscle Biopsy (an URGENT not elective procedure) Call the neuropathologist! 85% Sensitive. ] Biopsy involved muscle (MRI guided) ] Avoid EMG/injection sites or sites of trauma ] n n n Magnetic Resonance Imaging - detects incr. water signal, fibrous tissue, infiltration, calcification Investigational: Tc-99 m Scans, PET Scans Serologic Tests: ANA (+) 60%, Abs against t-RNA synthetases
INFLAMMATORY MYOSITIS Biopsy Findings n n n Inflammatory cells Edema and/or fibrosis Atrophy/ necrosis/ degeneration Centralization of nuclei Variation in muscle fiber size Rarely, calcification
Polymyositis: CD 8+Tcells, endomysial infiltration Dermatomyositis: Humoral response B cells, CD 4+ T cells; perifascicular/perivascular infiltration
Autoantibodies in PM/DM Ab ANA U 1 -RNP Ku Mi 2 PM 1 Jo-1 SS-B (La) PL-12, 7 Freq (%) 50 15 <5 30 15 25 <5 <5 Clinical Syndrome Myositis SLE + myositis PSS + myositis Dermatomyositis PSS – PM overlap Arthritis+ ILD+ Raynaud SLE, Sjogrens, ILD, PM ILD + PM
Anti-synthetase syndrome: ILD, fever, arthritis, Raynauds, Mechanics hands– association with Jo-1
MALIGNANCY & MYOSITIS n n Higher association with DM, less common with polymyositis Common tumors: Breast, lung, ovary, stomach, uterus, colon, NHL 60% the myositis appears 1 st, 30% neoplasm 1 st, and 10% contemporaneously Studies found 20 -32% with DM developed CA Lancet 2001 Ann Int Med 2001.
Dermatomyositis and Malignancy n All adults with DM should have ageappropriate screening annually during first several years after presentation: ] CXR ] Colonoscopy or sigmoidoscopy ] PSA/prostate exam in men ] Mammogram, CA-125, pelvic exam, transvaginal ultrasonography in women
PM/DM Complications PULMONARY n Aspiration pneumonitis n Infectious pneumonitis n Drug induced pneumonitis n Intercostal, diaphragm involvement n Fibrosing alveolitis n RARE: ] ] Pulmonary vasculitis Pulmonary neoplasia CARDIAC n Elev. CPK-MB n Mitral Valve prolapse n AV conduction disturbances n Cardiomyopathy n Myocarditis
Recap: PM/DM Diagnosis Symmetric progressive proximal weakness n Elevated muscle enzymes (CPK, LFTs) n Muscle biopsy evidence of myositis n EMG: inflammatory myositis n Characteristic dermatologic findings n
INFLAMMATORY MYOSITIS Treatment n n Early Dx, physical therapy, respiratory Rx Corticosteroids : 60 -80 mg/day ] n 80% respond within 12 weeks Steroid resistant Methotrexate ] Azathioprine ] n n IVIG, Cyclosporin, Chlorambucil: unproven No response to apheresis
PROGNOSIS n n n n Poor in pts. with delayed Dx, low CPK, early lung or cardiac findings, malignancy PT for muscle atrophy, contractures, disability Kids: 50% remission, 35% chronic active disease Adult < 20 yrs. do better than >55 yrs. Adults: Mortality rates between 28 -47% @ 7 yrs. Relapses & functional disability are common Death: due to malignancy, sepsis, pulm. or cardiac failure, and complications of therapy
RHABDOMYOLYSIS n n n Injury to the sarcolemma of skeletal muscle with systemic release of muscle macromolecules such as CPK, aldolase, actin, myoglobin, etc Maybe LIFE-THREATENING: from hyperkalemia, met. acidosis, ATN from myoglobinuria Common causes: Et. OH, Cocaine, K+ deficiency, infection, PM/DM, infection (clostridial, staph, strept), medications, exertion/exercise, cytokines
INCLUSION BODY MYOSITIS n n n n Bimodal age distribution, maybe hereditary Males > females Slow onset, progressive weakness Painless, distal and proximal weakness Normal or mildly elevated CPK Poor response to corticosteroids Dx: light microscopy may be normal or show CD 8+ lymphs and vacuoles with amyloid. Tubulofilamentous inclusion bodies on electron microscopy