Juvenile Idiopathic arthritis and infectious arthritis Division of


 5 joints or more o Oligoarticular type (50 -60%)")









 o Evanescent skin rash (salmon-pink) o High fever o Polyarthragia/arthritis")



")







 o Children (<5 years)")









- Slides: 50
Juvenile Idiopathic arthritis and infectious arthritis 郭三元 Division of R-I-A TSGH
Juvenile rheumatoid arthritis Juvenile Idiopathic arthritis Juvenile chronic arthritis
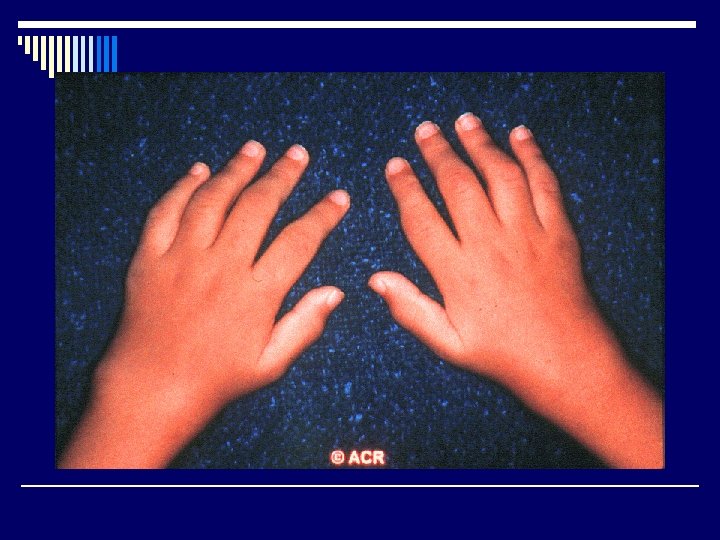
o Polyarticular type (20 -30%) 5 joints or more o Oligoarticular type (50 -60%) 4 joints or less o Systematic types (10%) o Enthesitis-related arthritis o Psoriatic arthritis
Juvenile idiopathic arthritis o Prevalence: 12 -113/100000, incidence 9 - 25/100000 o Age of onset < 16 years o Disease duration > 6 weeks o In oilgo- and poly- type: female > male, in systemic type: male=female o ESR usually elevated in poly- and systemic type, normal in oligo- type
Lab test o CBC, ESR, CRP o RF o ANA o HLA-B 27 o Ferritin o Anti-ccp
Genetic susceptibility o Spondyloarthropathy---HLA-B 27 o RF+ polyarticular – HLA-DR 1 and HLA- DR 4 o Early onset of oligoarticular with chronic uveitis ---HLA-DR 5 and HLA-DR 8 o Early onset oligoarticular --- HLA DQW 1 and DPW 2 o Systemic type--- HLA-DR 4
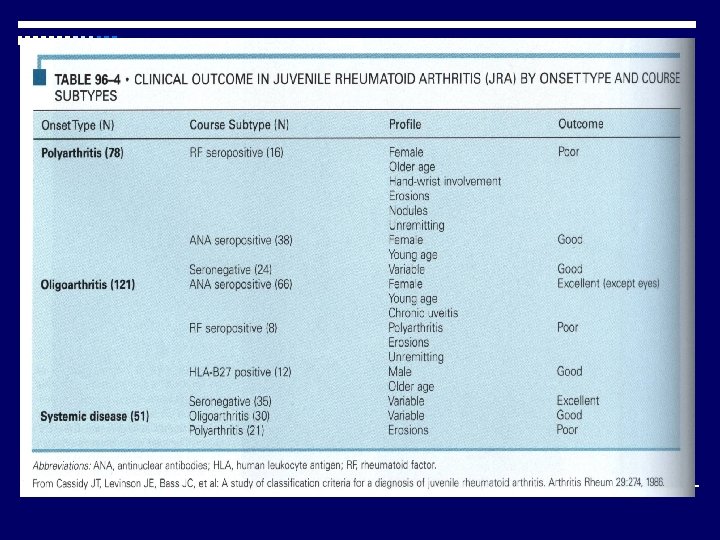
Polyarticular type o Symmetrical, large and small joints o Peak age of onset: 1 -3 years o F: M: 3 : 1 o Chronic uveitis: 5% o ANA: 40 -50% o Positive RF – 10%, increased risk of joint damage, more aggressive arthritis
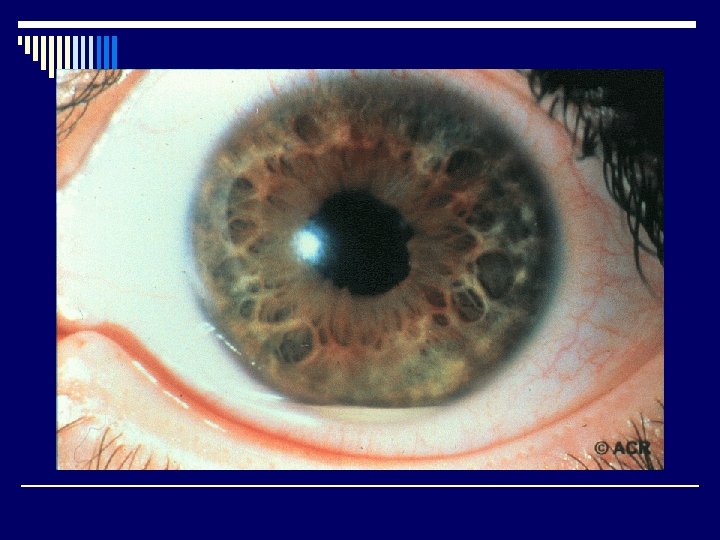
Oligoarticular type o Peak age of onset: 2 -5 years o F: M 5 : 1 o High frequency of positive ANA (70 -80%) o Chronic uveitis- related to positive ANA o RF: rare o Old age of onset (> 6 year), more often in males, with often HLA-B 27 positive
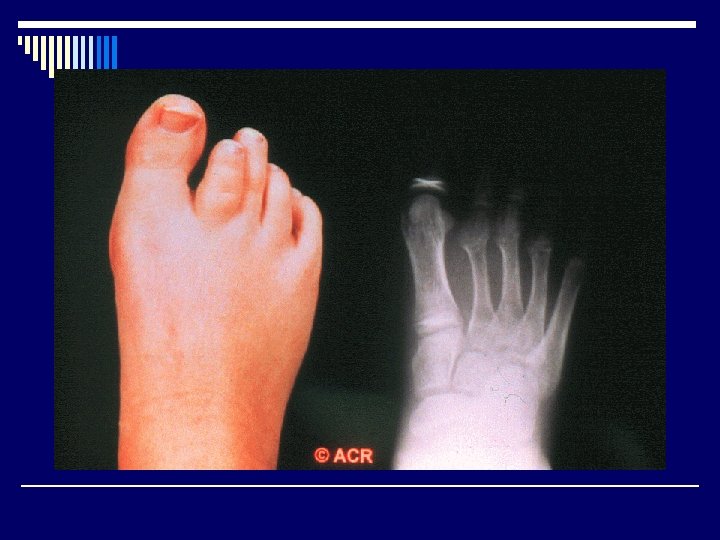
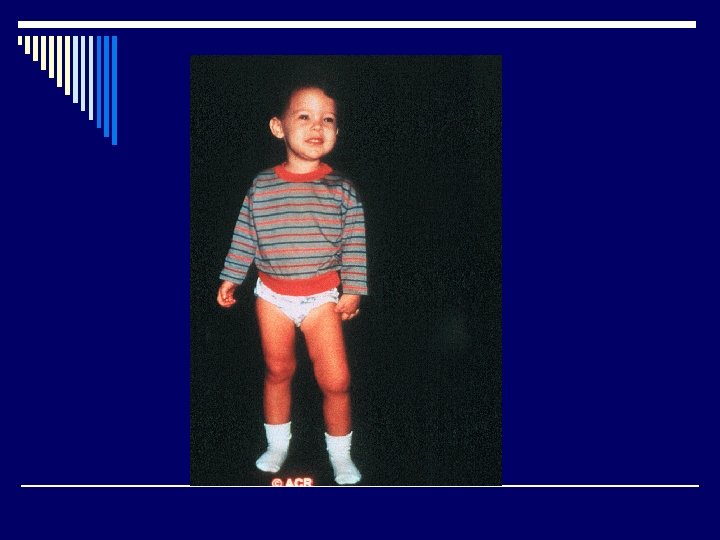
o Localized inflammation and cytokine release o Increase blood flow -macroepiphysis o Longer affected leg
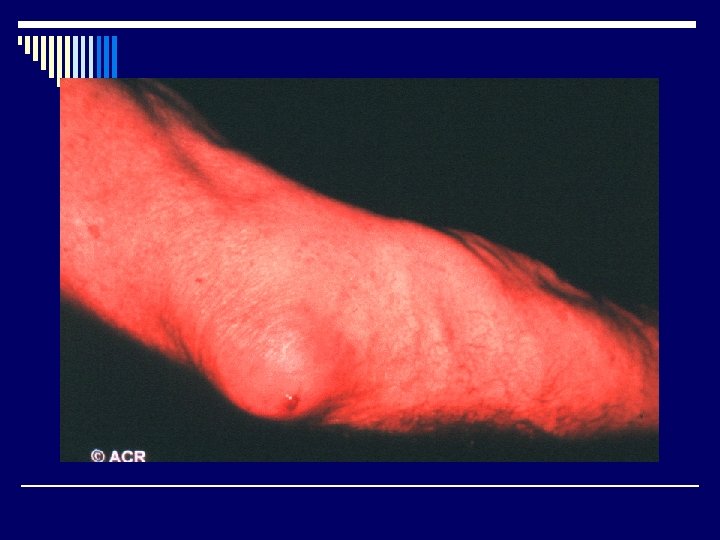
Systemic type (Still’s disease) o Evanescent skin rash (salmon-pink) o High fever o Polyarthragia/arthritis o F: M: 1: 1 o RF: rare o ANA: <10% o Uveitis: rare o hepatosplenomegaly, lymphadenopathy, pericarditis o high ferritin
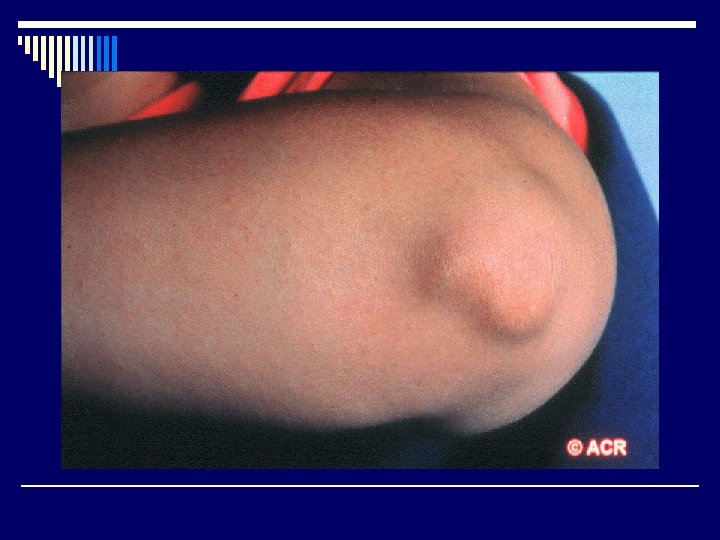
Koebner phenomenon
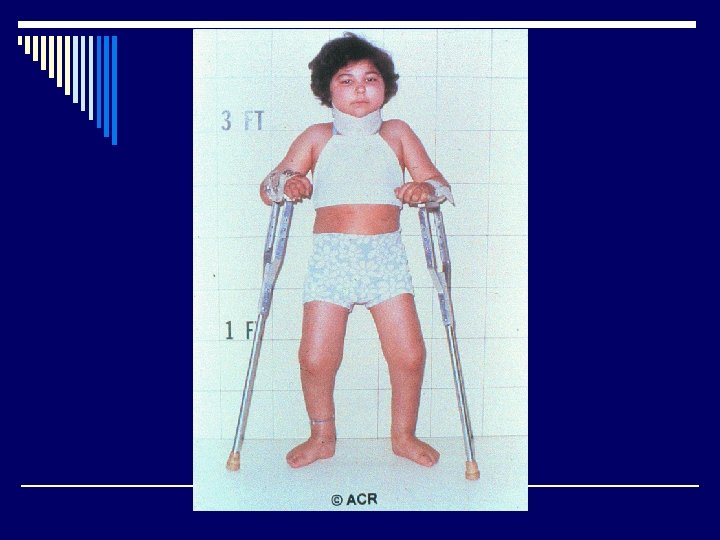
Management o Minimize the joint damage, early diagnosis and early treatment o Keep muscle strong and limb in good position, keep joint moving o Physical therapy and exercise o Routine eye examination from 3 -4 months interval to one year
Management o NSAIDs o Steroid o DMARDs o Biological agents ( anti-TNFα, anti-IL 6)
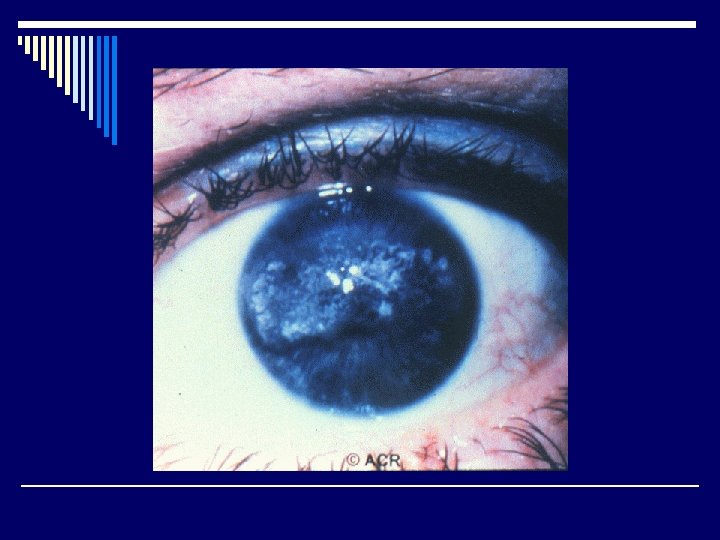
Prognosis o Oligoarticular type: 80% resolved after 15 years, 15% develop polyarticular type with severe joints problems, 50% decreased visual acuity after 10 years ( uveitis ) and 25% developed cataract or glaucoma o Polyarticular type: RF(+) showed more severe course and only 33% became independent after 15 years o Systemic type : 50% remission, others developed severe arthritis and especially in cases of disease onset < 5 years-old
Growing pain o Age attacked: 4 -12 years o F: M: 1: 1 o Deep aching, cramping pain in thigh or calf o Usually in evening or during the night, never in the morning o Normal physical examination and laboratory
Infection related arthritis
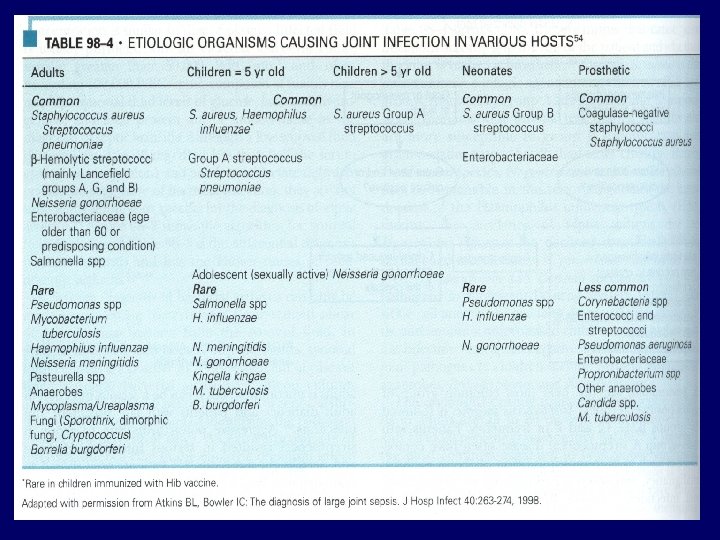
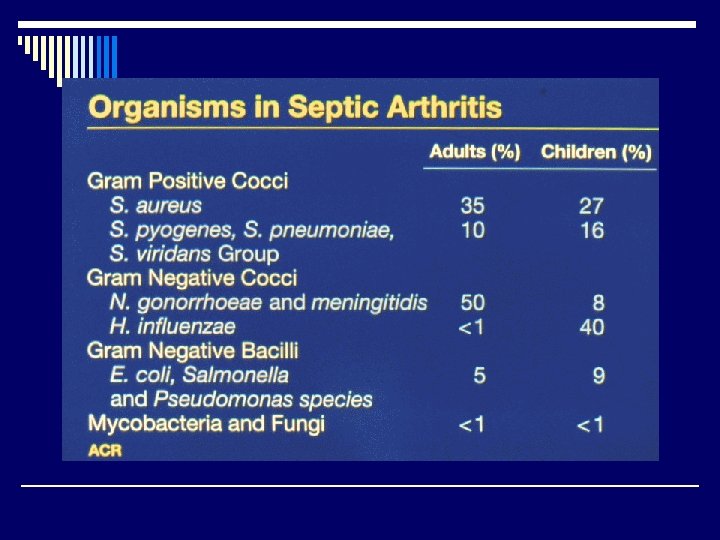
Septic arthritis o Acute onset of monoarthritis o Fever o Elevated ESR or CRP o Synovial fluid: WBC> 50000
Incidence of septic arthritis o 2 -5 /100, 000/year in general population o 5. 5 -12/100, 000/year in children o 28 -38/100, 000/year in RA patients o 40 -68/100, 000/year in prosthetic joint
Pathogenesis o Hematogenous route from a kind of remote o o infectious disease (70% ) – abundant vascular supply of synovium and lack of limiting basement membrane dissemination from near osteomyelitis Lymphatic spread from infection near the joint Iatrogenic infections from arthrocentesis or arthroscope (20% ) Penetrating trauma from plant thorns or other contaminated objects
Predisposing factors o Impaired host defense o Direct penetration o Joint damage o Host phagocytic defect
Impaired host defense o Neoplastic disease o Elderly (>65 years) o Children (<5 years) o Chronic illness ( DM, cirrhosis, chronic renal disease, HIV) o Immunosuppressive agents
Direct penetration o Intravenous drug abuse o Puncture wounds o Invasive procedures
Joint damage o Prosthetic joints o RA o Hemarthrosis o OA
Host phagocytic defects o Complement deficiency o Impaired chemotaxis
Relate to joint o Knee o Hip o Ankle o Shoulder o Wrist o Elbow o Bursa
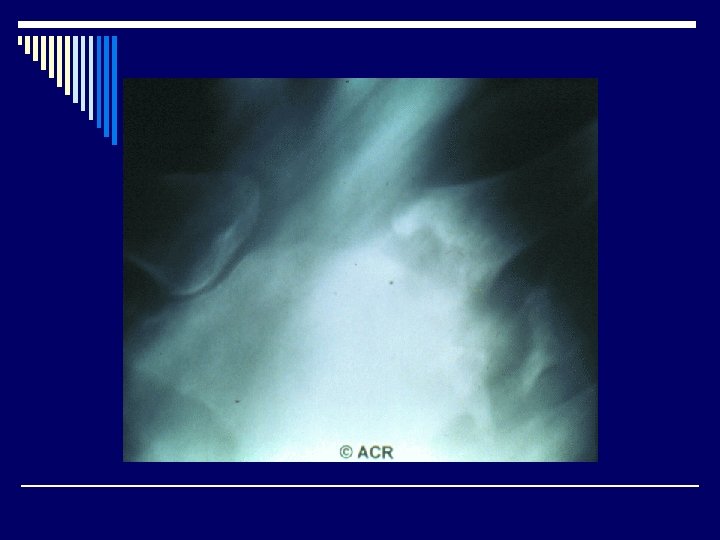
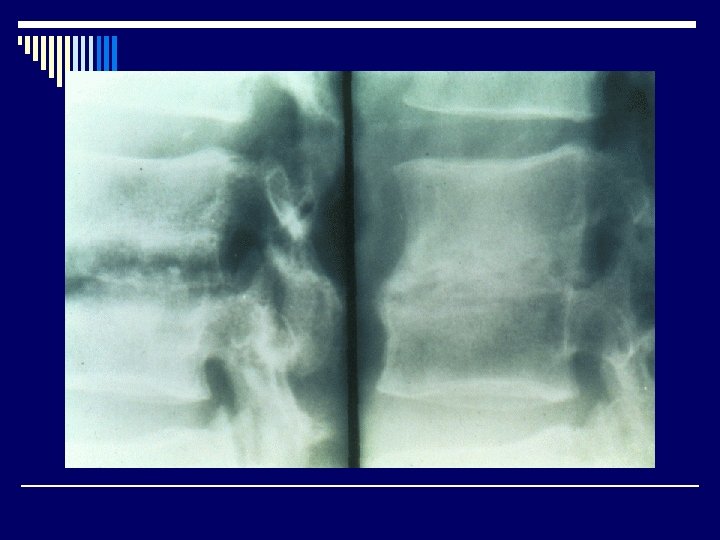
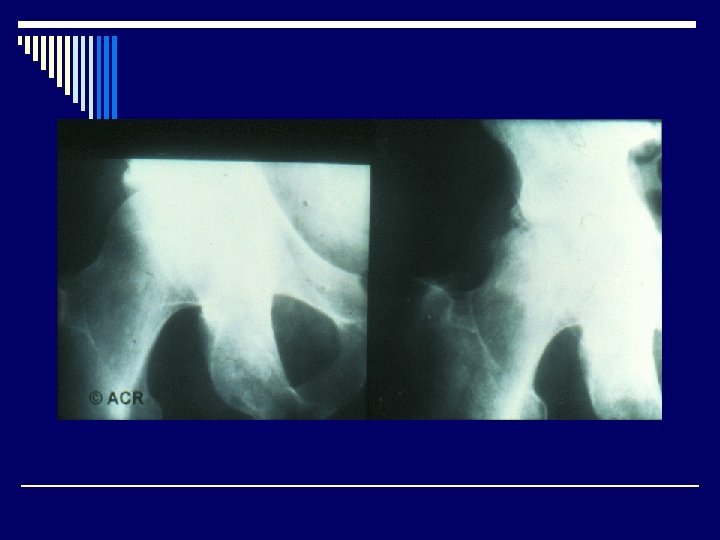
Radiological features o Joint effusion o Erosion o Joint space narrowing o Joint deformity o Osteoporosis o Bony ankylosis
Indication for surgical drainage o Hip and shoulder joint, S-C joint o Vertebral osteomyelitis with cord compression o Thick synovial purulent fluid or loculated o Persistent positive synovial fluid culture o Prosthetic joints o Associated with osteomyelitis o Delayed onset of therapy (>1 week)