Rosacea and GI disorders Inflammation and Dysbiosis Leonard

Rosacea and GI disorders Inflammation and Dysbiosis Leonard Weinstock, MD Associate Professor of Clinical Medicine Washington University in St. Louis Specialists in Gastroenterology
, Ironwood (Linzess) Research grants: Salix (Xifaxan - rifaximin) Consultant:")
Disclosures Speaker’s Bureau: Salix (Relistor), Ironwood (Linzess) Research grants: Salix (Xifaxan - rifaximin) Consultant: Salix (Relistor) Off label use of medicine: In context of published research and FDA IND applications for new research

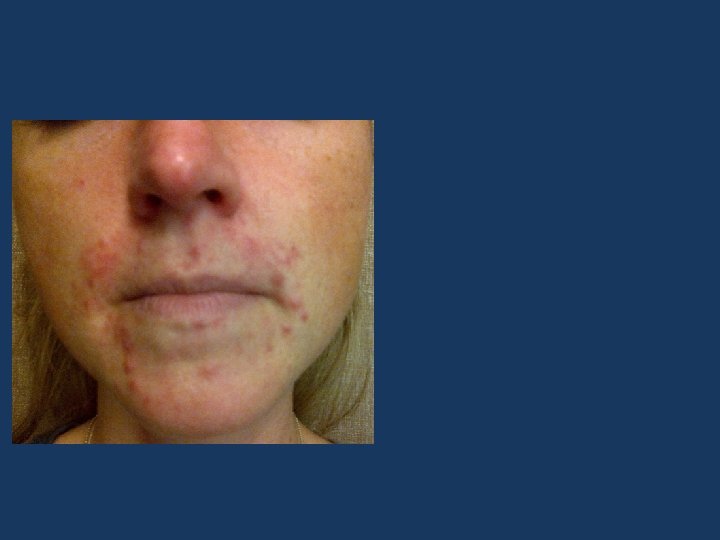
“Post-infectious Rosacea” “Rosacea-SIBO” 49 y. o. man • 3 yr Hx rosacea: • E/F/Pap • Failed 2 topical Abx • Started 4 months after food poisoning • Mild bloating • Dx: bacterial overgrowth

42 F s/p Mont. revenge 13 yrs ago followed by: – E/F/Phyma and ocular rosacea – Nail disorder – – IBS-c Cognitive dysfx Fatigue RLS 45 – Steatohepatitis – Type 2 DM 40 35 30 25 H 2 20 CH 4 15 Dx: Bacterial overgrowth 10 5 0 0 30 45 60 75 90

Review • Gut microbiome • History of rosacea & gut • Small intestinal bacterial overgrowth • Enteric infections lead to diseases • Antibiotic Rx for Rosacea-SIBO • Additional SIBO diseases and rosacea • Theories for shared pathophysiology

Gut vs. skin • 100 SF • 10 SF • Barrier with vascular & nerve interface • Barrier with vascular & nerve interface • Bacteria (100 trillion) • Bacteria (and mites) • > 500 types • Commensal when in balance and with normal innate and systemic immunity • > 200 types • Non-invasive when in balance and with normal innate and systemic immunity

Gut + microbiome > skin + spleen Largest immune system

Normal host prevents dysbiosis Stomach Colon bacterial balance, integrity & immunity 0 - 1000 Mucosal absorption Pancreas Colon 100, 000, 000 coliforms (bacteroides, firmicutes, bifidobacter, clostridium) Acid Motility ICV Distal ileum 100, 000 -1, 000, 000 coliforms oral bacteria Immunity (streptococcus, lactobacillus) Duodenum & Jejunum 1, 000 oral bacteria Proximal ileum 10, 000 oral bacteria Mondot. Dig Dis 2013; 31: 278 -85.

Effects of dysbiosis • Abnormal anatomy – Leaky tight-junctions --- incr. intestinal permeability – Thinner lamina propria, shallow crypts – Abnormal Peyer’s patches, fewer plasma cells • Immune disorders: – Altered cytokine profile – Altered innate immune response (Th 2 to Th 1, IL-17) – Diseases: atopy, diabetes, obesity, autoimmune

Bateman. Color Atlas of Dermatology. 1817. Text: “Rosacea and acne. Constipation. ”

History of rosacea and the gut • Alcohol & obesity – 13 th century (Chaucer) (? Steatohepatitis) • • Dyspepsia – 1895 Food intolerance/allergies – 1926 -1966 Achlorhydria – 1935, 1941 Gastritis – 1941 Celiac/jejunal diseases – 1965, 1970 Chronic pancreatitis – 1982 H. pylori – 1990’s IBD: UC 1989; CD 2000 (drug-induced, PPR, R. fulminans, granulomatous R. ) • Small intestinal bacterial overgrowth: 2008

Early text and rosaceaassociated disorders Kaposi. Pathology and Treatment of Disease of the Skin. 1895.
 • H. pylori: 1")
Textbooks and rosaceaassociated disorders • GI disorders (dyspepsia, diarrhea, constip) • H. pylori: 1 Coincidental , plausible , undecided 2, 3 4 • Parkinson’s disease • Hormonal changes 3 • Menopause • Migraine • Orthostatic hypotension • Vasoactive tumors • HIV 4, 5 5 1, 2 2 1 -3 1 2 • CNS tumors 1 1. 2. 3. 4. 5. Pelle. In Fitzpatrick 2012. Webster. In Bolognia 2008. In Mc. Kae 2005. Berth-Jones. In Rooks 2004. Plewig, Klingman. In Acne and Rosacea 2000.

Small intestinal bacterial overgrowth and rosacea First report in 2008

SIBO syndrome • Definition – – >105 colony forming units/m. L in jejunum Sx and/or signs of malabsorption • Treat 1 o small bowel abnormality – “Often impractical” • Antibiotics – Absorption and resistance concerns • Motility drugs – Limited medications • Intestinal permeability – Not addressed Gregg CR, Toakes PP. In Sleisenger and Fortran. Gastrointestinal and Liver Disease.
 in SIBO gas")
Lactulose breath test Early rise in H 2 (or CH 4) in SIBO gas chromatography • No gold standard to Dx SIBO - culture problems • Bacteria may be in various locations in the small bowel • Difficult to culture anaerobes

Textbook SIBO Scleroderma * Achlorhydria * Small intestinal Diabetes * pseudo-obstruction Pancreatic insufficiency * Radiation enteritis Immunodeficiency: Jejunal diverticulosis CLL, Ig. A def. , T-cell def. Post-surgical Billroth, Blind-loop anatomy: ICV resect. , J-pouch

SIBO – full blown • Symptoms • Pain • Bloating • Diarrhea • Foul flatus • Weakness • Weight loss • Signs and Labs • Edema • Anemia • Cachexia • Iron def. • Vitamin def. • Nutrient def.

“New” SIBO • • Crohn’s dis. * Celiac dis. * Irritable bowel synd. * Chronic liver dis. * • • • Restless legs synd. Rosacea Parkinson’s dis. * • • Renal failure Hypothyroidism Acromegaly Post-chemotherapy Fibromyalgia Rheumatoid arthritis * Interstitial cystitis Chronic prostatitis * Associated with rosacea Weinstock. Dig Dis Sci 2010; 55: 1667 -73. ; Weinstock. Inflam Bowel Dis 2010; 16: 275 -9. ; Pimentel. N Engl J Med 2011; 364: 22 -32. Walters, Weinstock. Sleep Med 2011; 12: 610 -3. ; Bellot. Liver Int 2013; 33: 31 -9. ; Parodi. Clin Gastroenterol Hepatol 2008; 6: 759 -764. ; Fasano. Mov Disord 2013; 28: 1241 -9. ; Weinstock. Dig Dis Sci 2008; 53: 1246 -51. ; Geng. Can J Urology 2011; 18: 5826 -30.

Diseases after GI infections w Guillain-Barré syndrome w Celiac disease w Reactive arthritis w Pancreatitis w IBS – 20% recall infection first Molecular mimicry & autoimmune pathways with genetic predisposition Koga. J Infect Dis 2006; 193: 547 -55. Yu. Rheum Dis Clin Noth Am 2003; 29: 21 -36 Stene. Am J Gastroenterol 2006; 101: 2333 -40.

Post-infectious IBS & associated syndromes Infection in gut Motility leads to SIBO Genetic phenotype (low IL-10) for IBS Pi-IBS, FMS, RLS, CPPS

Pi-IBS • 7 studies/2056 people: incidence 7 -30% • Duration: 50 -100% life-long (2 studies) • Pathophysiology: – Weak MMC leads to SIBO – Rat model: Camphylobacter caused SIBO in 27% – Anti-vinculin antibody studies • Rats AVA led to loss of myenteric nerves • Patients with Pi-IBS have AVA Pimentel 2004, 2011, 2013
 • Vinculin - involved in adhesion between cells – Skeletal muscle")
Anti-vinculin Ab (AVA) • Vinculin - involved in adhesion between cells – Skeletal muscle and nerves – Epineurial blood vessel smooth muscle – Endoneurium endothelial cells (EC) • Theoretical role in vascular changes of rosacea and neurologic balance in neurogenic rosacea: AVA might damage EC & nerves rosacea: especially in Pi-Rosacea Pimentel. Abstract. ACG; Am J Gastroenterol; October 2013. Massa et al. Muscle Nerve 1995; 18: 1277– 84.

Inflammation in SIBO & IBS • Interleukins – IL 1ß, 6, 8**, 12 • TNF-α (inflm. & incr. intestinal perm. ) • LPS (inflm. & incr. endothelial cell perm. ) • T- and B-lymphocytes – imbalance/activity • Mast cells infiltration in gut • Increased histamine, tryptase and seratonin • Substance P (neuropeptide) • Integrin Beta-7 T-lymphocytes (incr. vascular perm. ) Riordin. Scand J Gastroenterol 1996; 31: 977 -84. • A-V Ab Lin. JAMA 2004; 292: 852 -8. Hughes et al. Am J Gastroenterol 2013; 108: 1066 -74. Martinez et al. Gut 2013; 62: 1160 -8.

Systemic cytokines in rosacea • 60 rosacea pts vs. 25 controls • IL-18: 163 vs. 16 pg/ml (P<0. 01) • • • IL-6 lower in rosacea TNF-alpha numerically higher IL-8 not measured Salamon. Przegi Lek 2008; 65: 371 -4.

Changing roles of antibiotic Rx • 1950’s: Tetracycline • 2000: low dose doxycycline • Inhibition of matrix metalloproteinases • Inflammatory cytokine regulation • Inhibition of leukocyte chemotaxis & activation and anti-oxidation • Antibiotic effect on stratum corneum tryptic enzymes (SCTEs) • 2008: rifaximin for rosacea-SIBO Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Rifaximin – semi-sythetic CH 3 COO CH 3 22 CH 3 O OH CH 3 OH CH 3 22 OH OH OH CH 3 COO OH H N CH 3 O OH CH 3 H N O O O CH 3 O Rifamycin CH 3 N CH 3 O Rifaximin N CH 3 Rifamycin (Rifampin): FDA-approved uses of Rifaximin: Tb, Leprosy, streptococci, Traveler’s diarrhea and hepatic encephalopathy enterococci, staphylococci, Target 1&2 study for IBS published in NEJM Neisseria spp. and Target 3 study fully enrolled 11/15/13 Enterobacteriaceae EMEA – includes SIBO Pimentel et al. NEJM 2011; 364: 22 -32. Scarpignato. Digestion 2006; 73(S 1): 13 -27.

Antibiotic Rx for SIBO • 1356 articles reviewed, 10 met incl. criteria • Rifaximin most commonly studied (8 studies) • LBT normalization rate of 49. 5% (Efficacy varied by antibiotic dose) • Clinical response in 6 studies correlated with LBT normalization (SIBO eradication) Shah. Aliment Pharmacol Ther 2013; 38: 925 -34.

1 week course for H 2+ LBT Di Stefano. Aliment Pharmacol Ther 2000; 15: 1001 -8.
 (97% fecal excretion) w Gram-pos & neg;")
Rifaximin properties: benefits w Non-systemic (<0. 4%) (97% fecal excretion) w Gram-pos & neg; aerobes & anaerobes w Bile > water soluble – kills more bacteria in the small intestine than colon w Kills C. difficile Huang DB, Du. Pont HJ. J Infection 2005; 50: 97 -106.

Rifaximin resistance profile w Resistance w Not plasmid-mediated w Mutant resistant gut bacteria exhibit reduced viability w No clinically relevant resistance w 3 IBS-SIBO retreatment studies w Re-Rx in 2 – 7 courses: successful (83100%; 1 - 5 year follow up) Pimentel et al. Dig Dis Sci 2011; 56: 2067 -72. Weinstock. Dig Dis Sci 2011; 56: 3389 -90. Yang. Dig Dis Sci 2008.

SIBO in rosacea: LBT+ prevalence • Genoa, Italy: 46% of 113 consecutive rosacea clinic pts • St. Louis, MO: 51% of 63 consecutive GI clinic pts with rosacea • St. Louis, MO: 66% of 176 consecutive GI clinic pts with rosacea (incl. CH 4+ pts) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764. Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6. Weinstock. EMR review of records 2008 -2013.

False positive LBT: Controls • Genoa, Italy: 3/60 age matched controls • St. Louis, MO: 3/30 healthy controls (Lactulose gets to colon faster causes FP) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764. Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6.

Rifaximin for rosacea: 1 st study • N=113 pts seen in Rosacea Clinic • 83 F, 31 M, age 52 • 52/113 (46%) LBT+ • 24/113 H. p. + (7 had SIBO) • 7 pts treated for H. p. 1 mo after SIBO Rx (clinical response occurred with SIBO Rx) • GI sx response analyzed Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 • Rifaximin 1200")
Rifaximin for rosacea • N = 52 LBT+ (H 2 excretion) • Rifaximin 1200 mg/d/10 d vs. Placebo • Randomized, blinded only to pts • IGA scoring • 2 dermatologists (Kappa = 0. 97) • Additional studies • Cross-over for placebo group • Open label used for SIBO-negative pts • Subtype rosacea evaluated Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Randomized study results • Rifaximin normalized LBT in 28/32 • 71% cleared rosacea (GA score 0) • 21% marked impr. (GA score 1) • Placebo 2/20 worsened, rest unchg. • GI sx sig. decreased with rifaximin Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Before & 1 mo after 1200 mg/d/10 d rifaximin Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol 2008; 6; 759 -6.

Before & 1 mo after 1200 mg/d/10 d rifaximin Note periocular and cheek improvement Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol 2008; 6; 759 -64.

Additional study results • X-over: placebo group treated open-label • 17/20 LBT normalized • 15 of the 17 had rosacea cleared • 45/52 total eradication with rifaximin • 35/45 cleared • Improvement maintained in 96% at 9 mo • 2 w pap/pust returned & Re-Rx worked • LBT- group treated (see next) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 Rifaximin 1200 mg/d/10 d (N=20) Parodi et al. Am J Gastroenterol 2008; 6:")
(N=32) Rifaximin 1200 mg/d/10 d (N=20) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 SIBO positive Eradicated (LBT better) Rosacea cleared Flush")
Rifaximin for subtypes Patient type (N) SIBO positive Eradicated (LBT better) Rosacea cleared Flush (2) 2 2 2 Fl/Erythosis (27) 0 - - Papules (8) 6 5 4 Fl/Pap (34) 11 9 9 Fl/Ery/Pap (8) 7 6 3 Pap/Pustules (7) 4 4 4 Fl/Pap/Pust (16) 13 11 8 All four types (11) 9 8 5 Pap/Pust groups had SIBO > non P/P (p<0. 001) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Parodi study: critisms • Baseline mean IGA not stated – delta not shown • All sub-types included – Pust. +/- pap. was most impt to include (84/113 had one or both) • Study not blinded to physicians – 2 independent scores performed with high Kappa • LBT used for SIBO Dx – Potential for more false+ – Less invasive than jejunal aspiration

Second rifaximin study: methane • 15 H 2+ & 15 CH 4+ rosacea pts • Rx #1: rifaximin • H 2 pts - most responded • CH 4 pts - little or no improvement • Rx #2: metronidazole • CH 4 pts - majority with complete or significant clearance (Note: need for dual therapy in IBS-methane pts) Parodi. UEGS. Abstract 2008
 • Dx")
Rifaximin for rosacea: St. Louis • N=63 pts (59 from screening colonoscopy) • Dx by dermatolgist in 57; ETR in 50, PP in 9, refractory ocular in 4 (3 had E) • Most did not have GI sx • 32/63 pts (51%) had LBT+ vs. 3/30 controls (RR, 5. 0; 95% CI, 1. 7 -15. 1; P<0. 001) • 28 LBT+ pts given rifaximin 1200 mg/d/10 d • Limitations: open-label, self-assessment by questionnaire and photos by pts Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6

Improvement: self-assessed % Responders 50 45 40 46% 35 30 25 25% 20 15 18% 10 11% 5 0 Cleared/marked Moderate Mild Unchanged Cleared Moderate Mild Unchanged or Marked Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6.

Before & 1 mo after rifaximin 1200 mg/d/10 d Significant change in nose & pruritic rash over right eyebrow – patient seen 1 year later & both areas were clear

Before & 1 mo after rifaximin 1200 mg/d/10 d

Ocular rosacea Post-infectious ocular rosacea: 1 mo after rifaximin 1200/mg/day/10 d

Subsequent patient experience Higher dose to match IBS studies and additional Rx for complex pts: • Rifaximin 550 mg TID for 14 days • Comprehensive post-SIBO Rx for complex patients

Before & 5 wk after rifaximin 1650/mg/d/14 d Case 2 Eyes, RLS fatigue, memory, and nail strength Improved.

Before & 1 mo after rifaximin 1200 mg/d/10 d** **Pi-IBS and rosacea (worsened after colon cancer resection)

Before & 1 mo after rifaximin 1650 mg/d/14 d 1. 25 yrs after first treatment
")
Before & 1 mo after rifaximin 1650 mg/d/14 d (Failing Oracea, Metrogel, Protopic)

2 mo after end of rifaximin Less redness on cheek, nose, temple and beard area

Forehead papules: rifaximin 1650 mg/d/14 d 1 mo later: reduction of papules

Before & 3 mo after rifaximin 1650/mg/d/30 d

Facial rosacea study: 2014 • Prospective, R, DB, X-O study • PPR pts at UCSF • Rifaximin 1650 mg/d/14 d vs. placebo (regardless of LBT test result – blinded) • Rosacea-SIBO diet for all subjects • IGA scoring and masked photographs of face over 8 wks Steinhoff, Weinstock
 • Dry eye • Aqueous deficiency • Meibomian gland dysfunction")
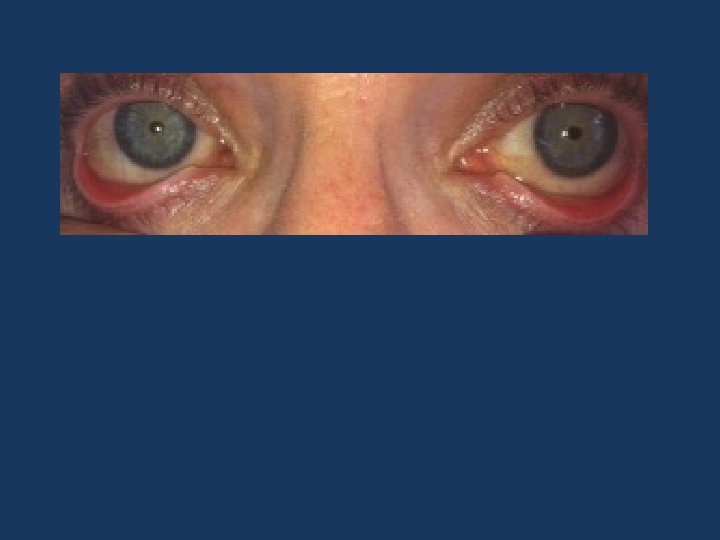
Ocular surface disease (OSD) • Dry eye • Aqueous deficiency • Meibomian gland dysfunction • Lipid deficiency: ocular rosacea • Eye lash loss • Tearing disorders • Corneal abrasions • Facial rosacea & ocular rosacea • 4% – 58% concordance

Rifaximin 1650/mg/day/14 d: Day 0 & Day 14 Less edema, redness and foreign body symptoms after Rx

Rifaximin 1650/mg/day/14 d: Day 0 & Day 14 Less injection of conjunctiva, decreased lid margin inflm, no symptoms

2 wks after 2 wks rifaximin 1650/d/14 d

Ocular rosacea study: 2014 • Prospective study over 8 wks • Rifaximin 1650 mg/d/14 d for all subjects Blinded to LBT test result • Rosacea-SIBO diet for all subjects • Standardized IGA ocular grading and photographs of eyes and face Berdy, Weinstock, Steinhoff

Rosacea and other SIBO diseases/disorders

Scleroderma: case study • Sclerodactyly, Raynaud’s, GERD, oral changes • GI SIBO sx – Bloating – Fatigue – Fe & B 12 def • New SIBO sx – RLS – Rosacea of face (not reported) 1 (Oc. Ros. - 45 SSc pts: 49% dry eyes, 40% blepharitis ) 2 1). Sleep Med 2002; 3: 341 -5. 2). Arch Clin Exp Ophthalmol 2012; 250: 1051 -6. 1). Sleep Med 2002; 3: 341 -5. 2).
 Rosacea:")
Scleroderma pt 4 wks after 2 wks Xifaxan and metronidazole (failed doxycyline) Rosacea: nose and cheeks much better RLS: completely better

Diabetes • Meibomian gland dysfunction study in a general population • N=619 people with and without eye sx • Asx MGD in 22% • Diabetes OR = 2. 2 2013 study: Viso et al. Invest Opthalmol Vis Sci 2012; 53: 2601 -6. Spoendlin et al. J Invest Dermatol 2013; 133: 2790 -3.
 • Sx MGD in 8. 6% of")
Rheumatoid arthritis • MGD study (cont. ) • Sx MGD in 8. 6% of population • Facial rosacea pts: OR = 3. 5 • Rheumatoid arthritis pts: OR = 16. 5 Keratoconjunctivitis common eye disease in RA RA seen in some neurogenic rosacea pts Viso et al. Invest Opthalmol Vis Sci 2012; 53: 2601 -6. Hamideh. Semin Arthritis Rheum 2001; 30: 217 -41. Scharshmidt et al. Arch Dermatol 2011; 147: 123 -6.

Crohn’s disease – Incidence of 5/60 consecutive CD clinic pts – 3 active rosacea: treated with rifaximin: 1 partial and 2 complete response – 2 not active (for both conditions) – Cases included: • 60 y. o. F w 40 yr ileitis on no Rx CD flares assoc w nasal rosacea – Rx - cleared • 46 y. o. M 26 yr CD s/p IC resection on 6 -MP CD flares assoc w facial rosacea – Rx - cleared • 32 y. o. F – see next Weinstock. J Clin Gastroenterol 2011; 45: 295 -297. Gastroenterol 2011;

Case 3: 32 y. o. WF with CD and rosacea 32 y. o. WF with Effect after 2 wks CD failing Rx. rifaximin Off all meds. 1200/mg/d/10 d
")
Subsequent effect of 8 wks biologic therapy (adalimulab)

Celiac disease • Celiac disease/SB disease – 20 of 60 rosacea pts had abnormal jejunal Bx – 4/20 were typical for celiac disease Possibities: • IL-8 and celiac • Primary effects of SIBO in jejunum Watson et al. Lancet 1965; 7402: 48 -50.

Parkinson’s disease • 70 PD pts, 22 controls – Sebumetry, corneometry, p. H • • 51% hyperhidrosis (low p. H) 32% cold/hot flush* 19% rosacea* 19% seborrhoea on forehead • MOA: “possible loss of vasostability d/t autonomic dysregulation in skin” Fischer et al. J Neural Transm 2001; 108: 205 -13.

Parkinson’s disease • Alpha-synuclein damages enteric neurons and reduces GI motility (prior to CNS Sx) • Prevalence of SIBO (LBT+) – PD (33) vs. controls (30): 55% vs. 20%; P=0. 01 – PD (48) vs. controls (36): 54% vs. 8%; P<0. 0001 – - SIBO Rx helped neuro sx Paillusson et al. J Neurochem 2013; 125: 512 -7. Gabrielli et al. Mov Disord 2011; 265: 889 -92. Davies et al. Parkinson's disease. Mov Disord 2013; 28: 1241 -9.

Steatohepatitis and rosacea?

Steatohepatitis • Liver expert poll: rosacea seen in NASH & ETOH, not viral or autoimmune hepatitis (Poordad, Bacon, Tetri) • Steatohepatitis (w/ & w/o ETOH) – SIBO (78% LBT+ in NASH) – LPS and IL-8 – IL-17 ---- increases VEGF (leads to angiogenesis) Bastard et al. Eur Cytokine Netw 2006; 17: 4 -12. Shanab. Dig Dis Sci 2011; 56: 1524 -34. Chander Roland B, J Clin Gastroenterol 2013; 47: 888 -93. Baudouin. J Fr Ophtalmol. 2007; 30: 239 -46.

Obesity and inflammation • Cytokines – Incr. T-cells, TNF-alpha, IL-6 • Dysbiosis – IBS & steatohepatitis link – Methane-obesity link • Fat absorption linked to histamine release (in rats) Bastard et al. Eur Cytokine Netw 2006; 17: 4 -12. Scalera. World J Gastroenterol 2013; 19: 5402 -5420. Basseri et al. Gastroenterol Hepatol 2012; 8: 22 -8. Ji et al. Am J Phys G L Phys 2013; 304: G 732 -40.
 Bernstein")
Alcohol abuse • Alcohol – flush • 1 ref for rosacea (not controlled) Bernstein JE, Soltani K. Br J Dermatol 1982; 107: 59 -61. Kostović K, Lipozencić J. Acta Dermatovenerol Croat 2004; 12: 181 -90.
 Rosacea ?")
Theoretical links in pathophysiogy SIBO Systemic IL-8 (or IL-6/TNF, IL-18 in NASH) Rosacea ? Upregulates local immune & inflm. LPS, IL-8 and integrin B-7 ? Increases dermal vascular permeability Systemic substance P ? Neurogenic inflam. or incr. in collagenase and bacterial virulence* FODMAPs/bacterial activity Histamine foods and mast cells ? Food triggers *Miljouin. PLo. S One 2013

Summary • Diseases and SIBO occurs after enteric infections • SIBO causes systemic inflammation • Rifaximin helps “Rosacea-SIBO”

Rosacea Multiple disorders & triggers Interacting disorders Altered local immunity Vascular and neural disorders Cutaneous disorders Inflammation SIBO TLR 2 & calthelicin Mites & bacteria Inflammation & immunity SIBO Triggers Environmental Food
 Activated OGFr Endothelial cell barrier maintained")
Opioid growth factor & receptor = Met-enkephalin (endorphin) Activated OGFr Endothelial cell barrier maintained Lymphocytes production controlled Singleton. Am J Respir Cell Mol Biol 2007; 37: 222 -31. Zagon. Immunobiology. 2011; 216: 579 -90.

LPS & OGFr – role in rosacea? Activated OGFr SRC and p. Y production leads to endothelial cell barrier disruption (Integrin could worsen net effect)

Potential Rx for LPS-induced inflam: Naltrexone binds to OGFr Decreased OGFr Activity Short-term Cells perceive OGFr reduction

Naltrexone & OGFr Animal studies: Activated OGFr Decreased T- and B-cell activity and less permeability (Decreased neovascularity in cornea – rats) Zagon. Arch Ophthalmol 2008; 126: 501 -6.

Role of Mast Cells in IBS Normal IBS Abdominal pain and severity correlated with the number of mast cells <5µm Proximity to nerves Elevated tryptase and histamine Barbara. Gastroenterology. 2004; 126: 3.

Rosacea food triggers • Direct • Hot temperature • Histamine foods • Indirect • FODMAPs • Spicy food • History • 1926 – Carbohydrate intolerance (Kendall) • 1966 – GI sx but Nl mucosal enzyme activity • 2008 -13 – SIBO link and risks of FODMAPs

Food triggers: GI perspective • Spicy food • Increase capsaicin • Hot drinks • Release vasoactive proteins • Histamine foods • Activation of mast cells • FODMAP foods • • • Increase fermentation & inflammation Substance P Hydrogen sulfide
 • Fruit (13%) – – – Citrus fruits Red plums")
• Alcohol (52%) • Fruit (13%) – – – Citrus fruits Red plums Raisins & figs Tomatoes Bananas • Dairy (8%) – Aged cheese – Yogurt • Vegetables – – Broad-leaf beans & pods Avocado Eggplant Spinach Wilkin J, National Rosacea Society Survey. • • • Spicy food (45%) Hot drinks (36%) Histamine foods – – – Red wine Aged cheese Yogurt Beer Bacon • Other triggers – – – Chocolate Vanilla Soy sauce Yeast extract Vinegar Liver

e breath test vs. History Rifaximin Comprehensive Rx Lactulos Non-absorbed ABx Diagnosis General principles of SIBO Rx Improve motility Restore permeability Reduce inflammation Weinstock, Fern, Thyssen, Todorczuk. Am J Gastroenterol 2006; 110: A 1124

Repeat rifaximin Rx for IBS N in study N repeat Rx 1 st response Re-treatment responses 1) 54/65; 2) 38/40; 3) 17/18 169 99 84 1– 6 1– 7 1– 2 75% had 100% response 74% 49 pts re-Rx avg 2. 2 x over 3. 8 yrs had 100% response; 9% needed intermittent rifaximin since prokinetic Rx failed 69% 1) 16/16; 2) 4/4 had 100% response Pimentel. Dig Dis Sci 2011. Weinstock. Dig Dis Sci 2011. Yang, Dig Dis Sci 2008.

H. pylori controversy • Local gastric infection with systemic immune changes • Cag-A more virulent – prevalent in Poland & China • A possible “coincidence” - H. pylori Rx also treats SIBO and also rosacea – which one explains the phenomenon observed in H. p. pts?

H. pylori: “plausible study” • N=60, 31 -72 y. o. Polish pts with P/P/E/F • 60 age- & gender-matched NUD pts w/o rosacea • Hp prevalence in rosacea 88% vs. 65% in NUD • Rosacea pts: 67% were cytotoxin-associated gene A (CAG-A) positive vs. 32% of controls pts • OCM Rx: 51/53 rosacea pts became Hp • Within 2 -4 wks rosacea disappeared in 51, markedly declined in 1 and remained unchanged in 1 subject • Rx decreased IL-8 (65%) and TNF-alpha (72%) Szlachcic et al J Physiol Pharmacol. 1999; 50: 777 -86. Szlachcic et al

Complex Regional Pain Syndrome • Reflex Sympathetic Dystrophy or Reflex Neurovascular Dystrophy • Severe pain, swelling & changes in skin often in arm or leg • Spreads throughout the body in 92% • Neurogenic inflammation, nociceptive sensitisation vasomotor dysfunction & aberrant response to tissue injury Report: 2 cases with improvement with LDN Chopra. Neuroimmune Pharmacol 2013; 8: 470 -6.


Clinical Summary of the MGD Staging Used to Guide Treatment Stage MGD Grade Symptoms Corneal Staining 1 + (minimally altered expressibility and secretion quality) None 2 ++ (mildly altered expressibility and secretion quality) Minimal to Mild None to limited 3 +++ (moderately altered expressibility and Moderate secretion quality) Mild to moderate; mainly peripheral 4 ++++ (severely altered expressibility and Marked secretion quality) Marked; central in addition “Plus” disease Co-existing or accompanying disorders of the ocular surface and/or eyelids Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Investigative ophthalmology & visual science. Mar 2011; 52(4): 2050 -2064.

Rosacea & CV risk factors • N = 60 rosacea pts & 50 controls (66% F) • Waist, BMI, glucose, CRP, lipids • Median duration of rosacea 36 mo • High total cholesterol (>200 mg/d. L), LDL (>130 mg/d. L) & high CRP levels, FHx of premature CVD and Hx smoking & ETOH > in rosacea vs. controls • Rosacea pts may have a high risk of CVD Duman N. J Eur Acad Dermatol Venereol. 2013 Aug 2. doi: [Epub ahead of print]

Healthy GI microbiota • • • Immune system development Epithelial integrity Inhibition of NF-k. B activation Anti-inflammatory metabolite production Colonization resistance Mucus homeostasis Bile acid deconjugation Lipid metabolism Insulin resistance

Mediators Activating factors • Intestinal permeability Mast Cell • Bacteria and biproducts • Food allergies (Ig. E- & non-Ig. E-mediated) • Neuropeptides • Bile acids • Tryptase • Lipid mediators • Cytokines ENS Altered gut secretion & motility Sensory neurons Corticotrophin Releasing Factor • Histamine CNS Pain GI Pain CPPS Cross talk Stress Pezzone. Gastroenterology 2005; 128: 1953 -64 Barbara. Neurogastroenterol Motil. 2006; 18: 6 -17.
- Slides: 102