SCLERODERMA Virginia Steen MD Professor of Medicine Scleroderma































- Slides: 33
SCLERODERMA Virginia Steen, MD Professor of Medicine
Scleroderma • Localized Scleroderma – Morphea – Linear Scleroderma – En Coup de Sabre (Progressive Hemi-atrophy) – Pansclerotic, Deep subcutaneous
Linear Scleroderma Linear, single extremity Hyperpigmented, Muscle atrophy but normal strength
Linear Scleroderma Severe contractures, growth disturbances, atrophy
Systemic Sclerosis An uncommon disease 250/million population, 20 new cases/ million per year, about 80 - 150, 000 in US Age onset usually 30 -50 years, rare under 10. Female 3 -5: 1; Increased in African-Americans Multisystem disease - Raynauds, digital ulcers, arthritis, tendon inflammation, skin thickening, myopathy, gastrointestinal, lung, heart and kidney involvement Survival – decreased primarily from severe lung involvement, pulmonary fibrosis and pulmonary hypertension
Diagnosis • Clinical diagnosis by Rheumatologist – Raynaud’s – Swollen fingers and/or skin thickening of hands/face – Esophageal symptoms-GERD. – Other organs • • Small intestines Pulmonary Fibrosis Pulmonary Hypertension Cardiac or Kidney involvement
Laboratory Diagnosis • Laboratory - not required – Antibodies helpful for prognosis, but not necessary for diagnosis ( even ANA can be negative) – There can be false positives, particularly slightly positive tests – GI x-rays supportive but not required for diagnosis
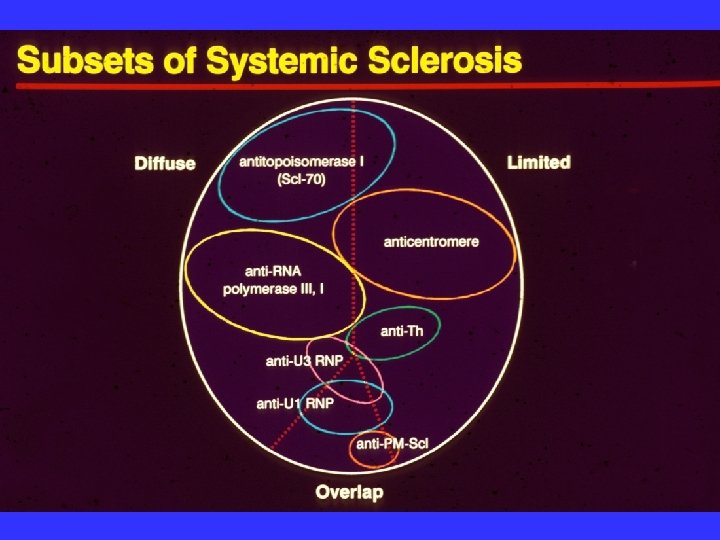
Clinical features associated with limited and diffuse scleroderma Limited cutaneous Diffuse cutaneous Raynaud’s -1 st symptom, Raynaud’s often delayed alone for many years Milder general symptoms Milder joint symptoms Acute onset, a lot of constitutional symptoms Arthralgias, carpal tunnel Tendon friction rubs Swollen, puffy HANDs Early diffuse skin Anti-Scl 70 antibody Anti-RNA polymerase III Puffy FINGERs Limited skin thickening Anti-centromere antibody
S KI N T HI C K N E S S 50 NATURAL HISTORY OF SCLERODERMA SUBSETS Contractures Renal crisis Myocardial failure Pulmonary fibrosis 40 Diffuse scleroderma 30 20 Limited scleroderma 10 Pulmonary hypertension Malabsorption 0 5 10 15 DISEASE DURATION (YEARS) 20
RAYNAUD’S
Digital Ulcers
. . . and can lead to autoamputation
Skin Thickening
Swollen Hands
Early Scleroderma Puffy Phase
Evaluation of Skin Thickening Rodnan Skin Score 17 different sites. Score 0 to 3 Total 51 Limited - <12 Diffuse >12 Measuring skin thickness. Rodnan Skin Score Questionnaire Health Assessment Other Measures. Medsger Severity Scale (only research)
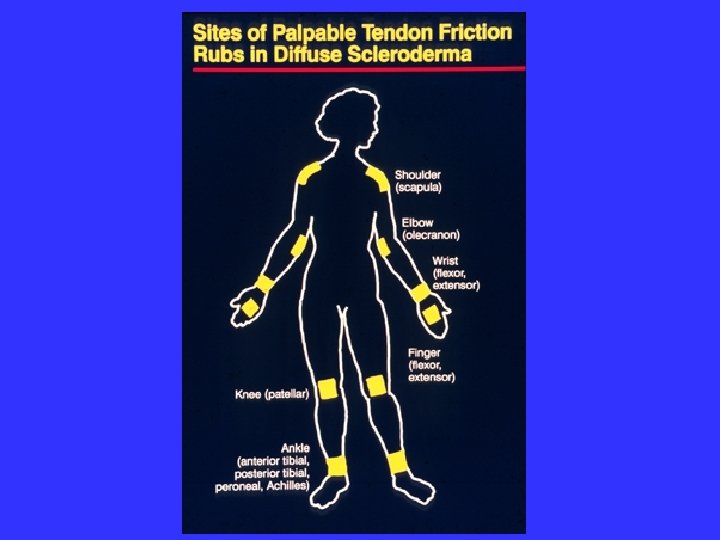
Joint and Tendon • Hand swelling, joint pain and stiffnessfingers, wrists, swelling/puffiness, other joints also • Contractures- hands, wrists, hips, shoulders, elbows. • Acroosteolysis- deformity causing loss of function • Tendon rubs- painful- hands, arms, ankles, knees
Sclerodactyly
Hand Contractures
CALCINOSIS
ACROOSTEOLYSIS
Systemic Sclerosis. Multisystem Disease
Gastrointestinal Involvement • Esophageal- trouble swallowing, heartburn, reflux, potential aspiration • Stomach –bloating, inability to eat full meals, need to eat small frequent meals • Small Intestine- malabsorption, diarrhea, pseudo obstruction, bacterial overgrowth, weight loss, need for hyperalimentation. • Large Intestine- constipation, rectal prolapse • Rectum- fecal incontinence
PULMONARY PROBLEMS IN SYSTEMIC SCLEROSIS • • Pleurisy, pleural effusions, pleural scarring Spontaneous pneumothorax (bronchiectasis) Aspiration pneumonia Malignancy-all cell types BOOP Interstitial fibrosis Pulmonary vascular disease (PHT)
Pulmonary Fibrosis • Shortness of breath with activity • Fatigue with activity • Pulmonary function tests- Decreased FVC, TLC and DLCO, restrictive disease • CT scan of lung- scarring, honeycombing • Begins early in disease and progresses slowly or rapidly, major cause of death
Pulmonary Hypertension • Shortness of breath and fatigue with exercise • Occurs later in illness • More common in limited scleroderma • Low DLCO on PFTs, and high PAP on echo • Most common cause of death
Heart and Kidney • Less common but more serious • Heart- Pericarditis, pericardial effusion, cardiomyopathy, rhythm problems, heart failure • Kidney- Malignant hypertension, kidney failure, dialysis.
Disability in Limited Scleroderma – Usually after a long history of Raynaud’s, (unless digital ulcers) – Pain, fatigue, GI symptoms – Loss of hand function – digital ulcers, loss of mobility/dexterity, fine motion – Fatigue/shortness of breath- anemia, weight loss, GI, pulmonary fibrosis/hypertension.
Special Situations • Raynaud’s – can be disabling without ulcers, if job is outdoors, requires cold exposure (meat cutter) • Limited skin- can be disabling even without contractures if very swollen, late acroosteolysis, need for fine motion • GI –can be very disabling - with severe reflux, vomiting, difficulty swallowing, fatigue, inability to eat, weight loss •
Disability in Diffuse Scleroderma – Early in Disease- mostly from progressive skin thickening, pain, fatigue, weight loss, contractures, digital ulcers. – Pulmonary fibrosis – Heart and Kidney
Special Consideration • Most diffuse scleroderma patients have enough problems that they are disabled. • While some diffuse scleroderma patients are able to continue working, it is usually because they are professionals and have a very flexible work situation.