Inflammatory Bowel Diseases Ulcerative Colitis Crohns disease Are

Inflammatory Bowel Diseases

Ulcerative Colitis & Crohns disease Í Are chronic inflammatory bowel diseases with protracted relapsing & remitting coarse. Í The incidence of ( IBD ) vary between population. Í The incidence of UC is 10/ 100000, while CD is 5 -7/100000. Í CD & UC had 2 peaks 1 st in young & 2 nd in 7 th decade.
 o o o Genetic: More common in")
Factors associated with the development of (IBD) o o o Genetic: More common in Jews. 10% have + ve FH of IBD. High concordance between identical twins. Associated with autoimmune thyroiditis & SLE. Four regions of linkage on chromosomes 16, 12, 6 & 14 (IBD 1 -4 ). HLA-DR 103 associated with sever UC. UC & CD with HLA-B 27 commonly develop Ankylosing Spondylitis. Environmental: UC is more common in non-smokers & ex- smokers. CD most patients are smokers. Associated with low residue , high refined sugar diet. Appendicectomy protects against UC.

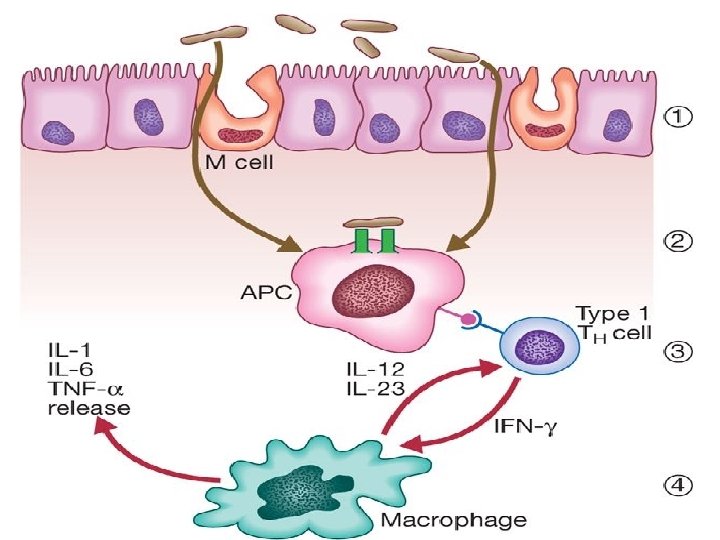
Pathogenesis Of IBD TRIGGER e. NTEROCYTES MACROPHAGES IL. 1 tnf SYS. SYM. ADHESION MOLECULE NEUTROPHIL AGREGGATION Fibroblast activation Fibrosis INFLAMMATION Stim. cd 4 IL 8 Mast & plasma cell activation ACTIVATION OF NEUTROPHILS

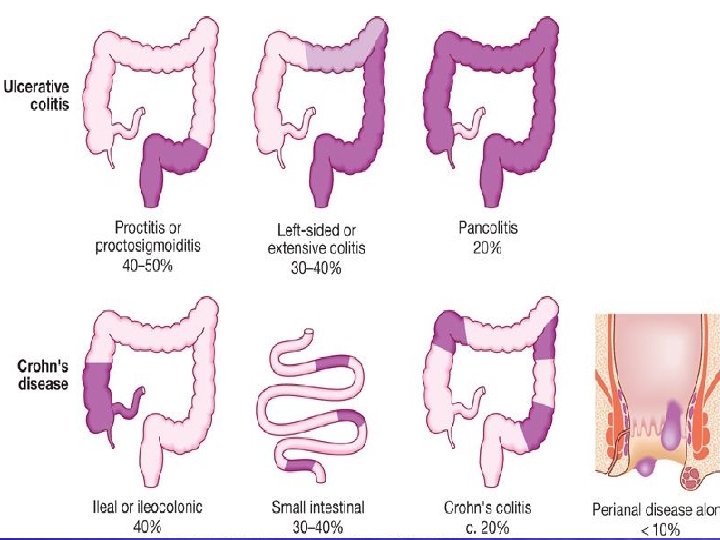
Common patterns of IBD distribution: Ulcerative colitis: - 40 -50% proctitis or proctosigmoiditis. - 30 -40% left sided colitis or extensive colitis. - 20% pan colitis. Crohns, disease: - 40% Ileal or ileocolonic. - 30 -40% small intestinal. - 20% Crohns colitis. - <10% perianal disease (alone).

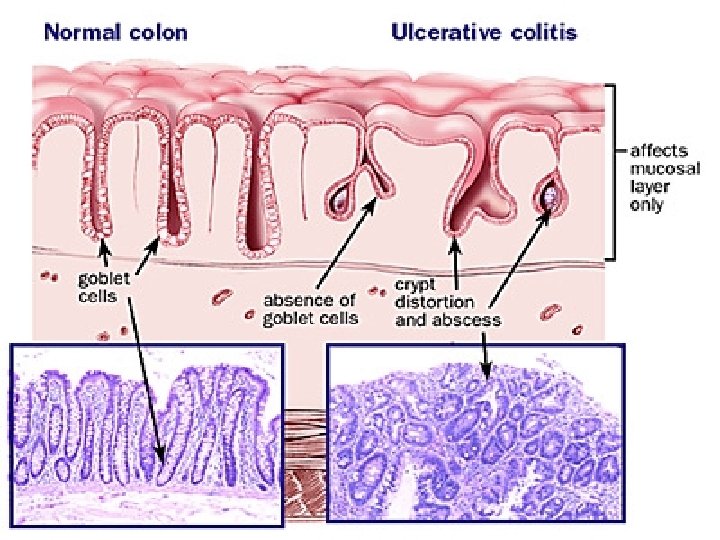
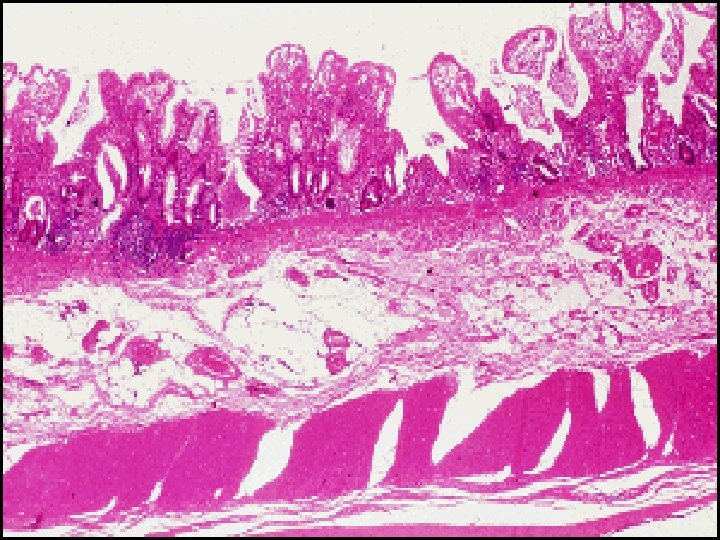
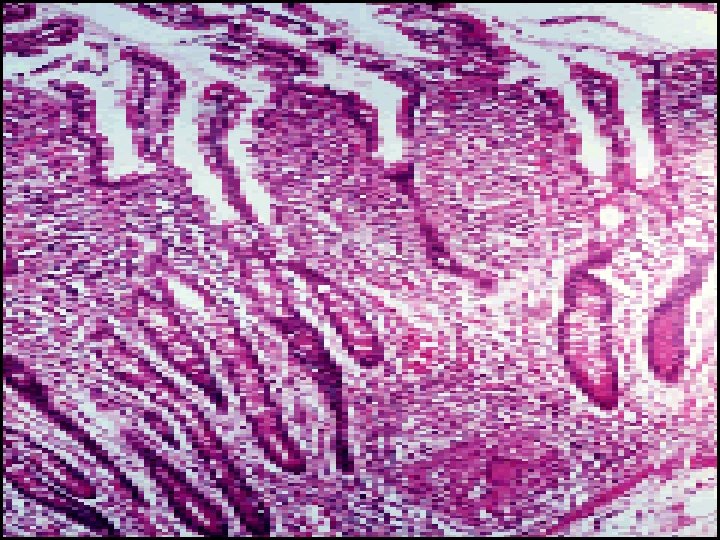
Histopathology of IBDS v. Ulcerative Colitis: -- The inflammatory process is limited to the mucosa . Acute & chronic inflammatory cells infiltrate the lamina propria & crypts ( Cryptitis ). Crypt abscesses are typical. -- Distorted Goblet cell which loss its mucus. -- Dysplasia : increased mitotic rate + nuclear atypia which herald the development of Ca colon.

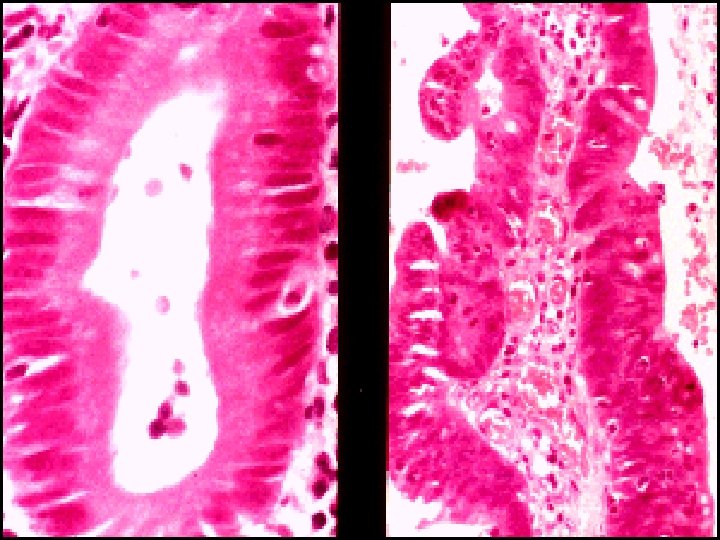

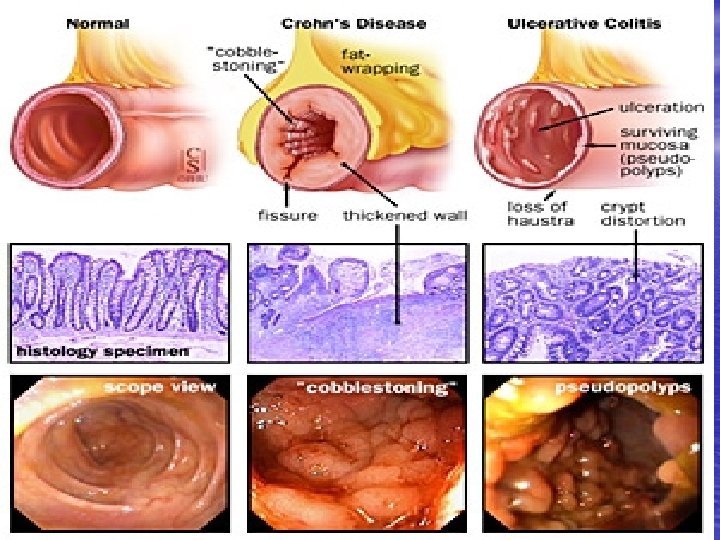
v. Crohn , s disease: --The whole wall of the intestine is oedematous & thickened , There are deep ulcers which appear as linear fissures with normal mucosa between them ( cobblestone). -- Fistulae & ulcers. -- The lesion is patchy ( skip lesion ). -- Chronic inflammatory cell infiltrate the whole layers -- Microgranuloma (aggregate of histeocytes which surrounded by lymphocytes & contain giant cells). -- Aphthus ulcer.

Clinical features of IBDS Ulcerative Colitis: -- The 1 st attack is most severe. -- Characterized by relapse & remission. -- Rarely chronic unremitting coarse.

Precipitating factors for acute relapse: ØGastroenteritis. ØAntibiotic. ØNSAIDS. ØEmotional stress. ØIntercurrent infection.

Í Proctitis: Rectal bleeding & mucous discharge some times with tenesmus , no constitutional symptoms. Í Proctosigmoiditis: bloody diarrhea with mucous Small no. of patients with v. active limited disease develop fever, lethargy & abdominal discomfort. Í Extensive colitis: bloody diarrhea with passage of mucous, in sever cases anorexia , nausea , weight loss & abdominal pain , patient is toxic with fever & tachycardia & signs of peritoneal inflammation.

Disease severity assessment in UC Mild severe 8 Daily Bowel frequency <4 >6 8 Blood in stool +/- +++ 8 Stool volume <200 >400 8 PR <90 >90 8 Temperature Normal >37. 8 8 Sigmoidoscopy Normal or granular Blood in lumen 8 Abdominal XR Normal Dilated bowel & /or mucosal islands 8 Hb g/dl Normal <100 8 ESR <30 >30 8 S. Albumin g/l >35 <30

Crohn , s disease: Ileal involvement: Abdominal pain which is associated with watery diarrhea (with out blood & mucous) + weight loss + features of protein & vitamins deficiencies. Crohn , s colitis: Like ulcerative colitis. *** Rectal sparing + Perianal disease*** Small bowel & colonic disease. Isolated Perianal disease. Severe oral ulceration.

Differences between UC & CD Ø Ø Ø Ø Ø 1 -UC involve only the colon while CD involve any part of GIT. 2 -UC is continuous while CD is patchy. 3 -Rectum is always involved in UC while rectal sparing in CD. 4 -Histology: UC is superficial while CD affect all intestinal layers. 5 -Pathology: UC there is Cryptitis & Crypt abscess While CD there is granuloma. 6 -Presence of fistulae in CD > UC. 7 -Presence of Perianal lesions in CD > UC. 8 -Clinical presentation: bloody diarrhea in UC while in CD abdominal pain , wt. loss. 9 -UC is more in non/ex-smoker appendicectomy protect , while CD more in smokers. 10 -Surgery is curative in UC & not in CD.





Complications of IBD v. Intestinal : § Severe colitis. § Perforation. § Hemorrhage. § Toxic megacolon. § Fistula. § Cancer of the colon.

v. Extra intestinal: § Unrelated to IBD activity: -Autoimmune hepatitis. - Primary Sclerosing Cholangitis & Cholangiocarcinoma. - Gallstones. - Amyloidosis & oxalate calculi. - Sacroiliitis/ankylosing spondylitis. - Metabolic bone disease.

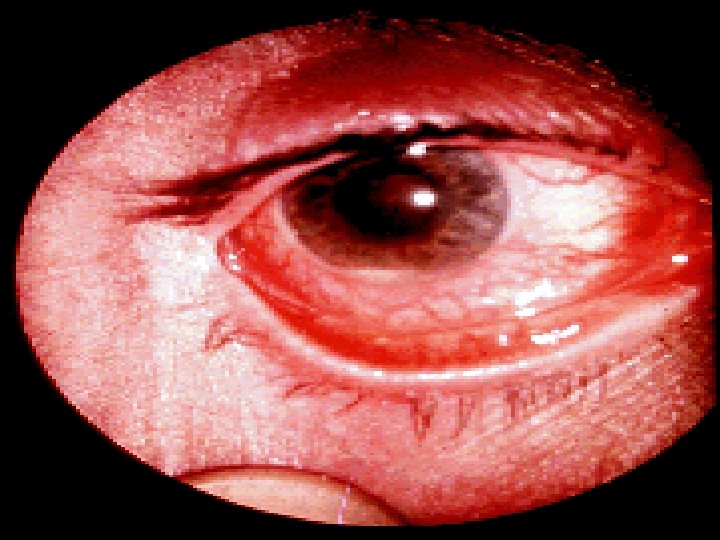
• Occur during the active phase of IBD: - Conjunctivitis. - Episcleritis. - Mouth ulcers. - Fatty liver. - Liver abscess / Portal pyaemia. - Mesenteric or portal vein thrombosis. - Venous thrombosis. - Arthralgia or large joints. - Erythema nodosum. - Pyoderma gangrenosum




Differential diagnosis of IBD FD. D of UC & Crohn , s colitis: v. Infective: § § § Bacterial: Salmonella, Shegella , Campylobacter pylori Viral: Herpes simplex proctitis, Cytomegalovirus. Protozoal: Amoebaiasis. v. Non-Infective: § § § Vascular: Ischemic colitis, Radiation proctitis. Idiopathic: Collagenous colitis. Drugs: NSAIDs. Neoplastic: Colonic carcinoma. Other: Diverticulitis.

FD. D of small bowel CD: v. Other causes of right iliac fossa mass. ØCaecal carcinoma ØAppendicular mass ØInfection ( TB , Yesinia , Actinomycosis ) v. Mesenteric adenitis. v. Pelvic inflammatory disease. v. Lymphoma.

Investigations of IBDs. z. Blood tests: z. Bacteriology: z. Endoscopy: Indications for endoscopy: o o o Diagnosis of IBD. Disease extent. Stricture ( biopsy ). Filling defect. Differentiation between UC & CD. For follow up: Random biopsies for dysplasia or cancer for UC > 8 ys. z. Barium studies. z. Radionuclide scan.

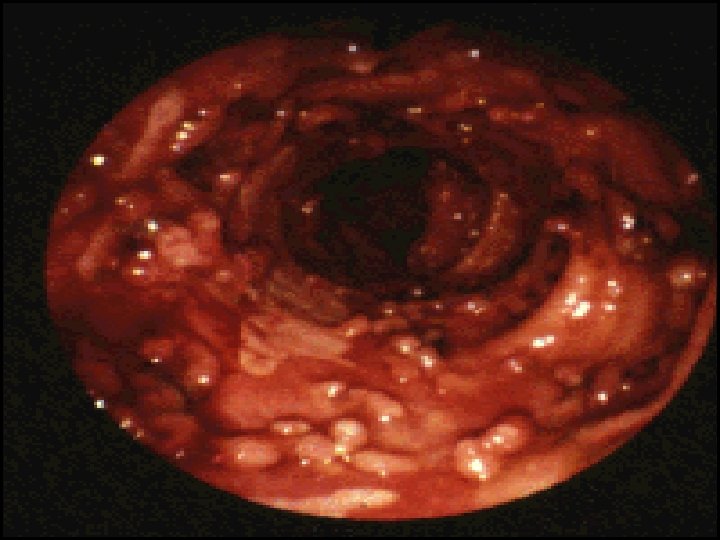
• Endoscopic image of ulcerative colitis affecting the left side of the colon. The image shows confluent superficial ulceration and loss of mucosal architecture Crohn's disease (regional ileitis)


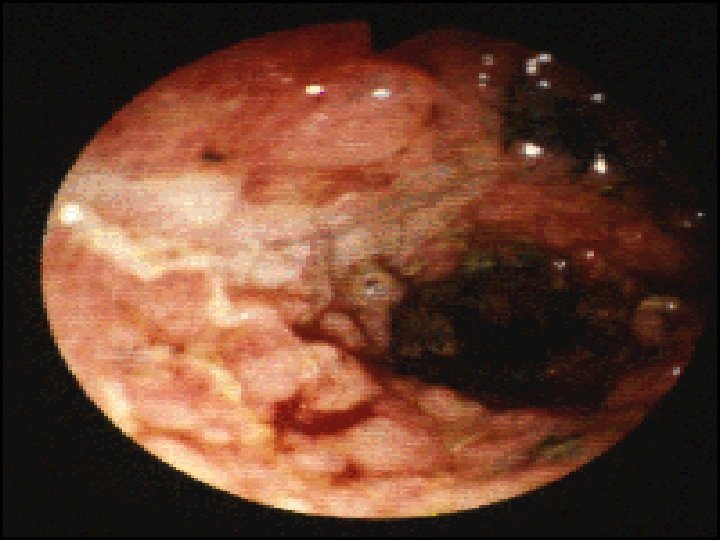
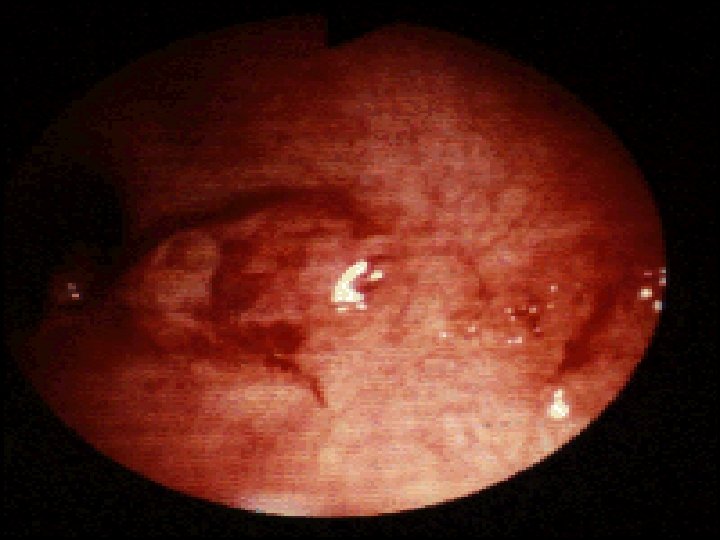
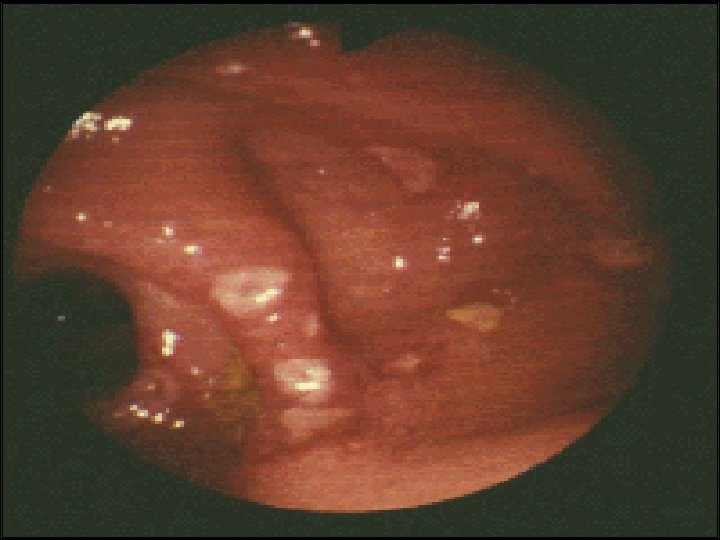

Endoscopic views of Crohn’s disease showing mucosal oedema, ulceration and exudates.

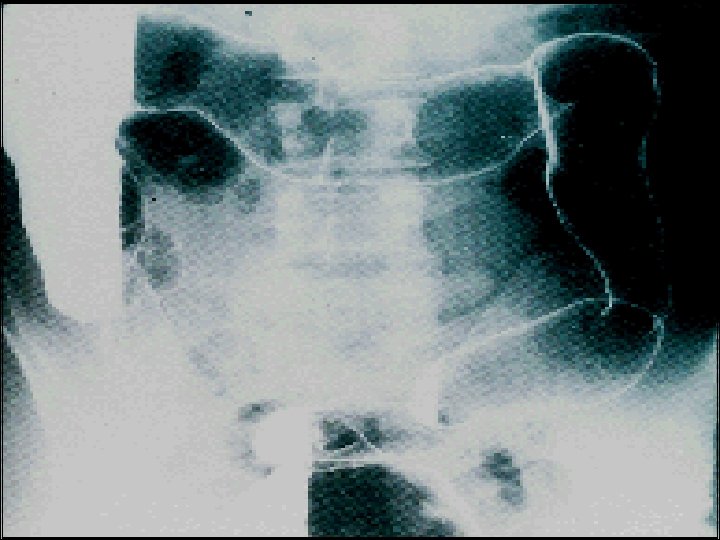
Ulcerative colitis. Double-contrast barium enema study shows pseudopolyposis of the descending colon Crohn’s disease (regional ileitis)


Imaging Crohn’s Disease • Small bowel contrast study vs CT – SBFT useful for characterizing length of involvement and areas of stricture • Characteristic Findings – – – Mucosal nodularity Narrowed lumen Ulceration String sign Abscesses or fistula • String Sign – Term often applied to the appearance of any marked narrowing of the lumen, but originated as descriptor of reversible narrowing in Crohn disease. – Narrowing caused by incomplete filling as result of irritability/spasms associated with ulceration. String Sign Masselli G. The gastrointestinal string sign. Radiology. 2007 Feb; 242(2): 632 -3.

Imaging Ulcerative Colitis • Barium Enema vs. CT – Barium Enema is no longer the test of choice • Findings – Continuous lesions from rectum proximally with circumferential involvement n Lead Pipe Sign n n Repeated episodes of mucosal ulceration and marked muscularis hypertrophy results in shortening, narrowing and smoothing out of the normal haustral markings. “Lead pipe” appearance of colon due to chronic scarring and retraction/loss of haustra Weinstein A et al. A super ‘lead pipe’ colon: radio-pathological correlation of long-standing ulcerative colitis. SA Journal of Radiology; 2008 Oct: 70 -72

Radiographic Features in Crohn's • The transmural inflammation of CD leads to • • • decreased luminal diameter and limited distensibility. As ulcers progress deeper, they can lead to fistula formation. The radiographic "string sign" represents long areas of circumferential inflammation and fibrosis, resulting in long segments of luminal narrowing. The segmental nature of CD results in wide gaps of normal or dilated bowel between involved segments.

CT enterography in Crohns disease • large volumes of ingested neutral enteric contrast material permit visualization of the entire small bowel and lumen. • Unlike routine CT, which is used to detect the extraenteric complications of CD such as fistula and abscess, CT enterography clearly depicts the small bowel inflammation associated with CD by displaying mural hyperenhancement, stratification, and thickening; engorged vasa recta; and perienteric inflammatory changes. • CT enterography is the first-line test for the evaluation of suspected CD and its complications.

MRI in Crohn's disease • As an initial test in children or in adults with multiple radiation exposures, MR enterography is comparable to CT in diagnostic accuracy. • Pelvic MRI is superior to CT for demonstrating pelvic lesions such as ischiorectal abscesses and perianal fistulae
) Modulate cytokine")
Drugs used in treatment of IBDs Aminosalysilates: (( Mesalasine, Olsalazine , Balsalazide)) Modulate cytokine release from mucosa Delivered to the colon by: 1 -PH-dependent ( Asacol ) 2 -Time-dependent ( Pentasa ) 3 -Bacterial breakdown by colonic bacteria from carrier molecule ( Sulfasalazine, Olsalazine, Balsalized ).
 Thiopurines:")
Corticosteroid Prednisolone , Hydrocortisone , Budesonide. Anti-inflammatory ( topical, oral or I. V) Thiopurines: Azathioprine , 6 -mercaptopurine Immunomodulation by inducing T-cell apoptosis. Is effective in 6 -8 ws after starting therapy.

Methotrexate • Anti-inflammatory • Side Effect: Intolerance in 10 -18%. nausea stomatitis hepatotoxicity pneumonitis.
 • Given as I. V infusion 4 -8 weekly.")
Anti-TNF antibodies (Infliximab & adalimumab) • Given as I. V infusion 4 -8 weekly. • Induce apoptosis of inflammatory cells • Uses: Moderately-severely active CD especially fistulating & in sever active UC. Ø Anaphylactic reaction after multiple infusions. ØContraindicated in presence of infection , reactivation of TB. ØIncreased risk of infection & alignancy.

Ciclosporine v. Suppression of T cell expansion. v. As rescue therapy to prevent surgery in UC responding poorly to corticosteroid. v. No value in CD. Side Effects: Nephrotoxicity. Neurotoxicity. Hirsutism.

Antibiotics Antibacterial. Useful in perianal CD. Side Effects: Peripheral neuropathy in long term metronidazole. Antidiarrheal agents: ( Codeine phosphate , Loperamide , lomotil) Avoided in moderately or severe active UC may precipitate colonic dilatation.

Treatment of IBDs Treatment of Ulcerative Colitis: q. Treatment of acute attacks( Induction of remission ). q. Prevent relapses (Maintenance ). Sulfasalazine, Aminosalysilates. q. Detect carcinoma at early stage. q. Select patients for surgery.

Active left-sided or extensive ulcerative colitis: o High dose Aminosalysilates + Topical W aminosalicylat & Corticosteroid o Oral prednisolone 40 mg for more active disease & if no response to topical therapy. Sever UC: Admission& managed by physician, surgeon. 1 -Clinically: for presence of abdominal Pain, Temp. , PR , stool bl. & frequency. 2 -Lab. : Hb% , WBC count , Alb. , Electrolytes , ESR & CRP. 3 -Radiologically: For colonic dilatation on plain abdominal XR

Medical management of fulminant UC 1 -I. V fluid. 2 -Transfusion if Hb< 10 gm/L. 3 -I. V methylprednisolone ( 60 mg daily ) or Hydrocortisone. 4 -Antiboitic for proven infection. 5 -Nutritional support. 6 -Subcutanous heparin for prophylaxis of venous thromboembolism. 7 -Avoidance of Opiates & Antidiarrheal agents. 8 -I. V Cyclosporine ( 2 mg/kg) or Infliximab ( 5 mg/kg ) in stable patient not responding to steroid 3 -5 days

Indication for Urgent Colectomy Colonic dilatation >6 cm on plain abdominal X-Ray. Lab. & Clinical deterioration. No response after 7 -10 days.

Indications for Elective Colectomy Impaired quality of life. -Loss of occupation or education. -Disruption of family life. Failure of medical therapy. -Dependence on corticosteroids. -Complications of drug therapy.

Indications for Colectomy Fulminant colitis. Disease complications unresponsive to medical therapy. -Arthritis. -Pyoderma Gangrenosum. Colon cancer or severe dysplasia.

Maintenance of remission in UC: -Life-long treatment for all patients with extensive disease & distal disease with more than once per year relapse. -Oral Aminosalysilate ( Mesalasine or Balsalazide ) or Salazopyrine ( for patients with arthropathy ). v If no response to aminosalicylate drugs treated with Thiopurines.

Medical treatment of CD Active Colitis or Iliocolitis: Like UC ( AS + Steroid ). Isolated Ileal: Corticosteroid( Budesonide) if no response surgery. Anti-TNF AB (Infliximab , adalimumab) : v. I. V infusion 4 -8 weekly on 3 occasions induce remission in patients with CD at any site of GIT v. For refractory cases to steroid. v. Heals enterocutanous fistulae & maintains longer remissions.

v. Effective in the management of Pyoderma gangrenosum & arthritis. v. It is contraindicated in presence of infection like TB. v. Relapse occur after 12 weeks so combine with Disease modifying drugs like methotrexate or Thiopurine. v. It cause remarkable mucosal healing---- scaring & stricturing so used with caution in stenosing disease.

• Side effects of biological drugs: • Suppression of cell-mediated immunity. • Infection; TB are contraindication for their use. • Malignancy: They should be avoided in patients with history of cancer or lymphoma. Increased incidence of malignant disease in patients on maintenance therapy particularly if combined with thioprines.
+Surgical Intervention +Endoscopic Balloon")
Extensive & diffuse iliocolonic: Drug therapy +Nutritional (Prolonged Parenteral Nutrition )+Surgical Intervention +Endoscopic Balloon dilatation. Fistulating & Perianal disease: Ø-Metronidazole or Ciprofloxacin. Ø-Localize fistula by Ba. radiography , CT , MRI. Ø-Surgical treatment. Ø-Corticosteroid & nutritional therapy ( TPN ). Ø-Thiopurine for chronic disease. Ø-Infliximab infusion 4 -8 weekly.

Maintenance of remission in CD: 1 -Smoking cessation. 2 -Aminosalysilate have minimal efficacy. 3 -Patients with relapse more than once per year: Thiopurine. 4 -If patient intolerant to Thiopurine or 6 mercaptopurine then use once weekly methotrexate + Folic acid. 5 -More severe & aggressive disease: Combined immunomodulating agents + Infliximab.
- Slides: 69