Postoperative LASIK complications Maayan Keshet M D LASIK











 Also known as diffuse intersitial keratitis, “sands of the Sahara”")




























 –")

 PK")


 Ablation plume blocks central")



- Slides: 63
Postoperative LASIK complications Maayan Keshet, M. D.
LASIK complications Flap displacement Infection Microstriae Macrostriae DES Glare/halos Epithelial ingrowth Corneal ectasia Central islands
Flap displacement Can occur from first day to years later Presentation: – Folding at flap edge – Complete dislocation – Complete avulsion Symptoms: acute pain, decreased VA
Flap displacement: Management Within few hours: reposition with weckcell/spatula at the slit lamp Within few days: reposition under microscope. – Underside should be scarped to removed epithelial ingrowth – Irrigate – Stretch out folds – Can suture in place – If melting -- may need to amputate flap
Infection Symptoms: pain, redness, decreased vision May begin days or weeks post-operatively Can occur on the surface or at flap interface
Infection: causes Bacteria: usually within 3 to 5 days Atypical mycobacteria: within 2 to 4 weeks – Multiple discrete infiltrates at the interface Fungus: at least 2 to 4 weeks post-op – May be secondary to steroid use Recurrent HSV: may present as dendrite or stromal keratitis
Infection: prevention Blepharitis: treat pre-op Pre- and post-op antibiotic drops Betadyne prep pre-op Limit topical steroid use Treat dry eye after surgery
Infection: Management Small peripheral superficial infiltrates: frequent fluoroquinolone or fortified antibiotic drops Infiltrates in the interface: lift flap, culture, irrigate with antibiotics, replace flap Remove flap if infection not improving with antibiotics or flap is melting
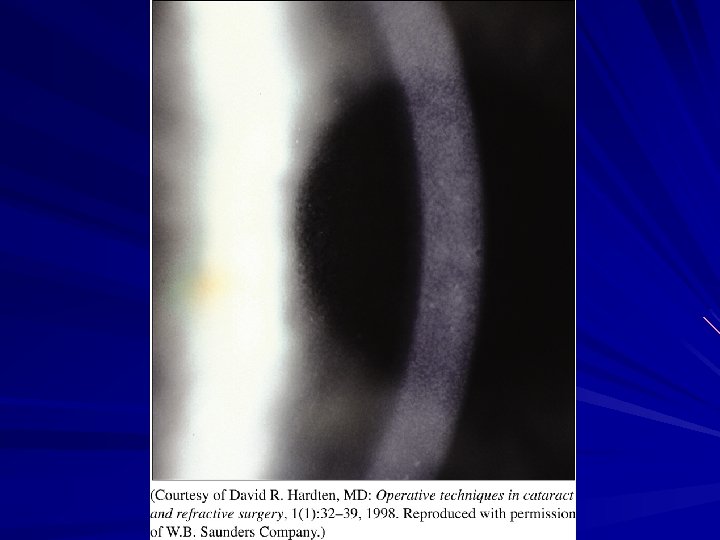
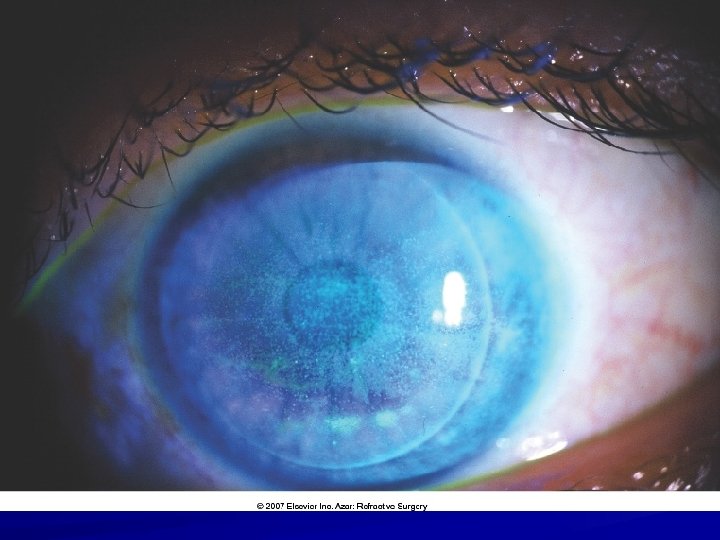
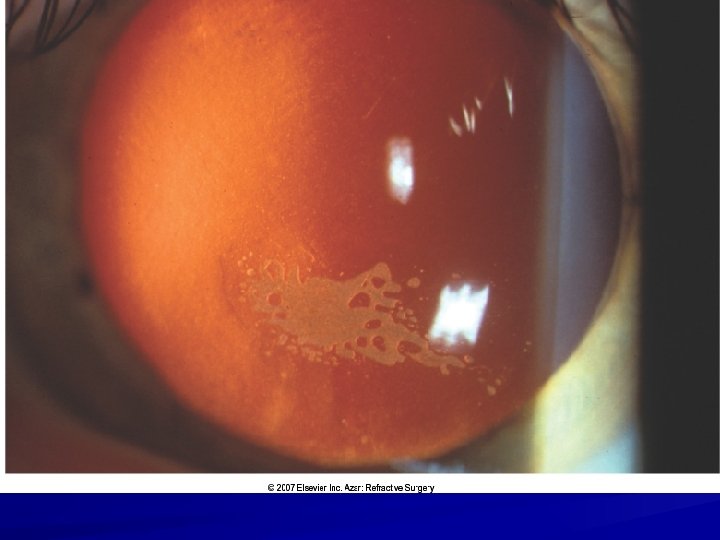
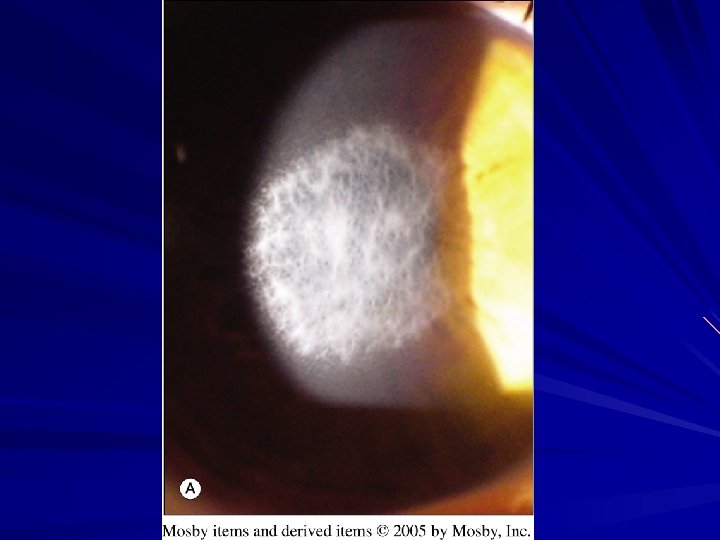
DLK (diffuse lamellar keratitis) Also known as diffuse intersitial keratitis, “sands of the Sahara” or S. O. S syndrome Sterile inflammatory response to trauma: – – – Normal case Bacterial toxins Meibomian secretions Epithelial defect Excessive intralaser energy Infectious keratitis (bacterial or viral) Onset: within days to months, even years
Haze: signs Haze usually begins peripherally and moves centrally “Wave like” migration pattern Minimal or no AC reaction Eventually, clumping of inflammatory cells obscures AC details Melting can occur
DLK: Grading Grade 1: Peripheral mild to no symptoms – Treat: PF Q 1 hour while awake Grade 2: Moderate infiltration extending to central cornea. Decreased vision and photophobia. – Treat: PF Q 1 hour, possibly Prednisone
DLK: Grading Grade 3: Significant infiltration, central involvement, clumping. – Treat PF Q 1 hour, Prednisone 60 mg PO, lift flap, brush stromal bed, and irrigate
DLK: Grading Grade 4: Dense white infiltrate centrally with possible melt – Treat: Lift flap, scrape, culture, and irrigate. – Steroid to stromal bed. PF Q 1 hour. Prednisone PO.
Pressure-induced Stromal Keratitis IOP is not measured Pt placed on PF for “DLK” Keratitis worsens on PF
Pressue induced stromal keratitis Fluid cleft develops in flap interface Cleft creates falsely low IOP Elevated IOP is a steroid response
Pressure-induced stromal keratitis: prevention/treatment Check IOP 1 week post-op Consider checking IOP with tonopen peripherally and centraly or off-center with Goldmann tonometer Treat with IOP lowering drops and stop the PF
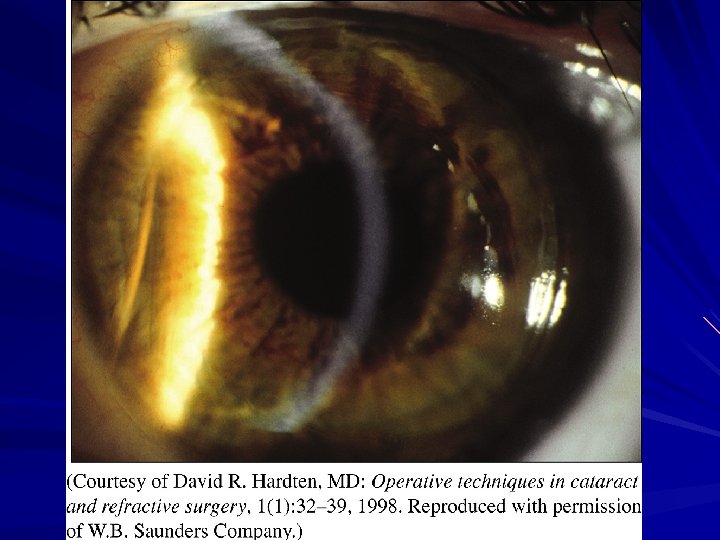
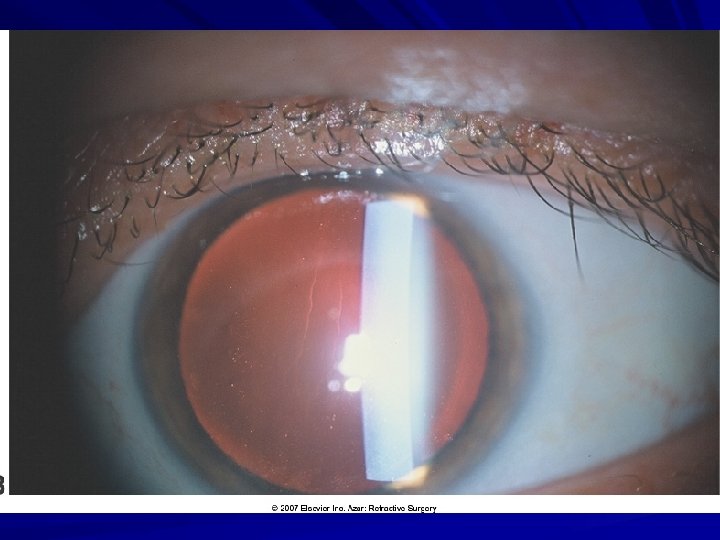
Microstriae Flap and bed have different curvatures after ablation Tiny striae can result when flap is reposited “cracked mud” appearance on retroillumination Fine parallel lines Usually do not affect visual acuity
Microstriae: causes Flap-stromal bed mismatch Epithelial defects can cause flap swelling which aggrevates the mismatch
Microstriae: prevention and treatment Check ink mark alignment and trough width around the flap Prevent epithelial defects Observe for most striae Refloat flap for central striae that are visually significant
Macrostriae Can significantly alter vision Result from: – Poor flap alignment intra-op – Minor trauma after surgery such as eye rubbing, eye drops, or eye trauma – Idiopathic
Macrostriae: prevention Make sure flap is well positioned, marks are aligned, and guters are symmetrical Remove speculum very carefully Educate pt on post-op care
Macrostriae: treatment Within days: lift and refloat On day one: lift and strech flap under microscope, or use weck-cell to iron it Consider removing central epithelium that may be “molding” striae in place PTK gray zone between micro and macrostriae Heat flap to “iron” it on Lift, stretch, and suture in position with seven 100 nylon sutures -- leave for 4 -6 weeks
DES/neurotrophic epitheliopathy Corneal nerves are transected --> neurotrophic epitheliopathy Decreased feedback loop to lacrimal glands Reshaped cornea may not provide as good a reservoir for tear film Suction ring may damage goblet cells
DES: predisposing factors and prevention Baseline dry eye: – – – optimize the ocular surface: AT Restasis Nasal hinge flap transects fewer nerves PRK transects fewer nerves Consider alternatives to laser vision correction Low ambient humidity Blepharitis/meibominitis: HC 2 x 2 x
DES: post-op management Tears, gels, ointments Restasis Plugs Humidifier Hydration, especially in physically active pts Imporves with time
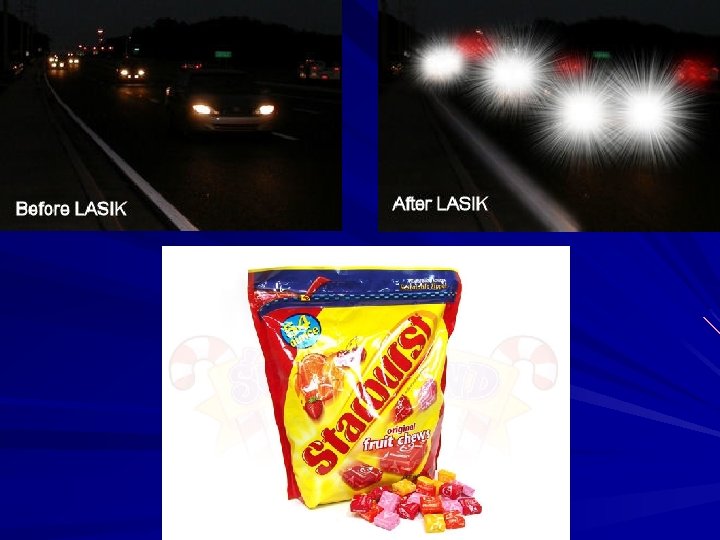
Glare/Halos Common 2 -6 weeks post-op Usually noted at night Predisposing factors: – High myopia (smaller optical zone) – High astigmatism (smaller OZ) – Large pupils (>6. 5) – Older age – Undercorrection
Glare/Halos: prevention Assess for glare/halos with night driving in pre -op exam Start by treating non-dominant eye in pts with pre-existing glare/halos Mark 3 and 9 o’clock axes if treating high astigmatism, to correct for intra-op cyclotorsion Use larger optical zone (6. 5 mm) and blend zone (8 mm) Custom LASIK may induced fewer higher order aberrations
Glare/Halos: Management Treat refractive error Topical Alphagan or dilute Pilocarpine Wavefront or Topo-guided ablation Try Pre. Vue lens from VISX Observe for improvement
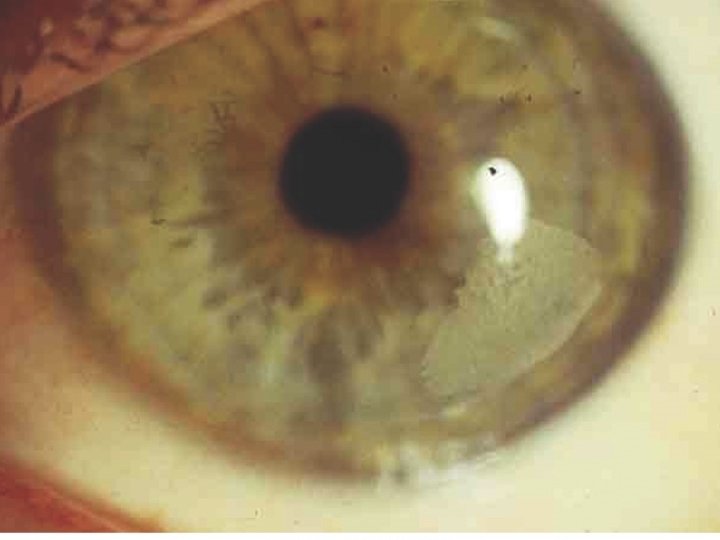
Epithelial ingrowth Commonly noted at flap edge Grows centrally and/or circumferentially from epithelial-interface tract Can present as island “planted” during surgery Dangers: – – Blocking visual axis Blocking nutrition from reaching the flap --> flap necrosis Can occur with enhancement procedures
Epithelial Ingrowth: predisposing factors Inverted flap edge Epithelial defect at flap edge ABMD Flap buttonhole (microkeratome) Free cap (microkeratome) Flap dehiscence Enhancements Hyperopic ablations (larger OZ -- ablates outside stromal bed Older pts
Epithelial ingrowth: Prevention Bandage CL Replace epithelial tags during enhancements Enlarge flaps for hyperopic treatment
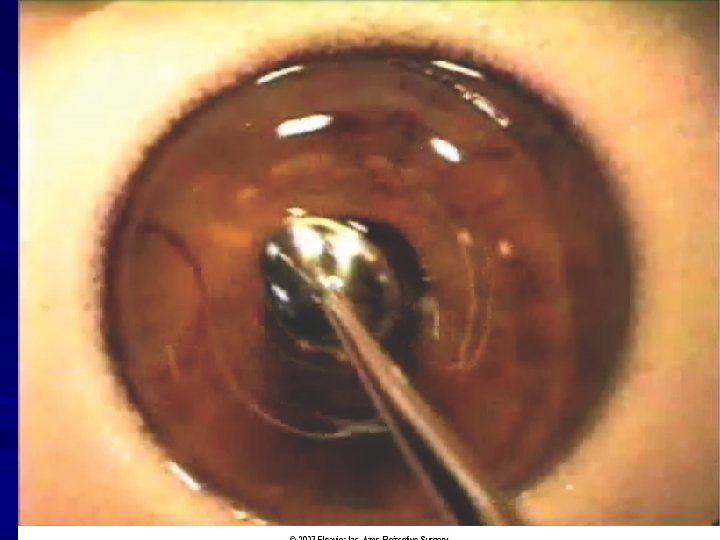
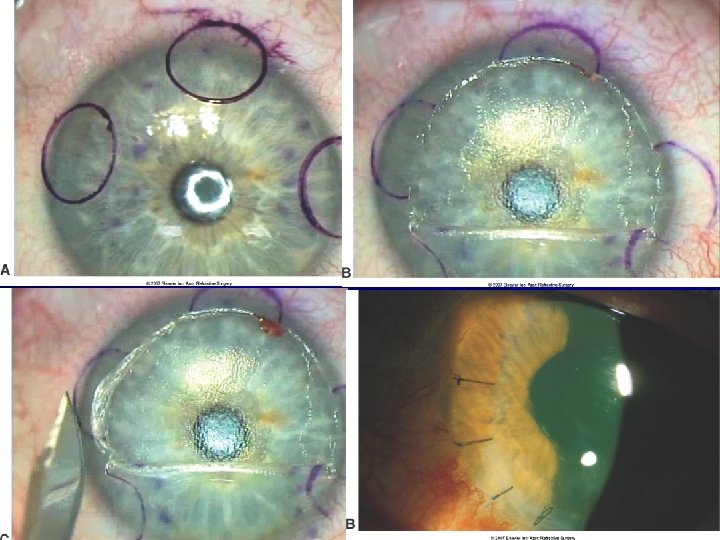
Epithelial ingrowth: management Mark ingrowth area and score side-cut with sinskey hook Lift flap under the microscope Use a Tooke knife or blade to scrape epithelial cells off stromal bed Flip flap over and irrigate interface Consider BCL
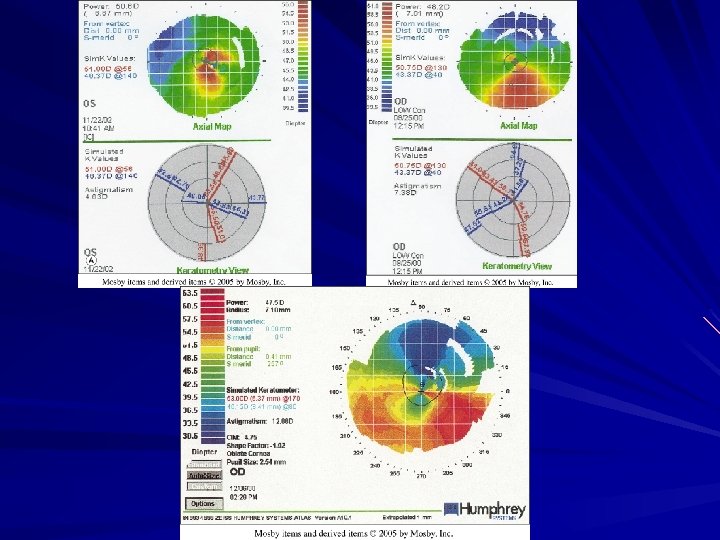
Corneal Ectasia Predisposing factors: Forme fruste keratoconus stromal bed less than 250 microns (some say <300) Thick flaps Younger pts with higher hysteresis
Corneal Ectasia: prevention Review topography for: – Asymmetric astigmatism (>1. 2 D difference) – ATR astigmatism – Inferior steepening or “crab-claw” pattern – Posterior float steepening – Overall steepening (>47)
Corneal Ectasia: prevention Check pre-op pachy Calculate ablation depth and residual stromal bed thickness Check stromal bed thickness intraoperatively Take pt age into account Consider PRK
Corneal Ectasia: management RGP or Boston sceral lens Intacs Collagen cross-linking (in trials) PK
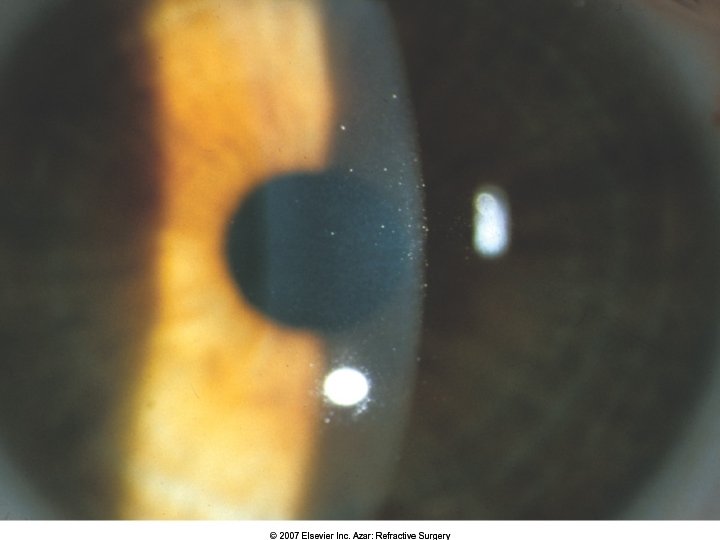
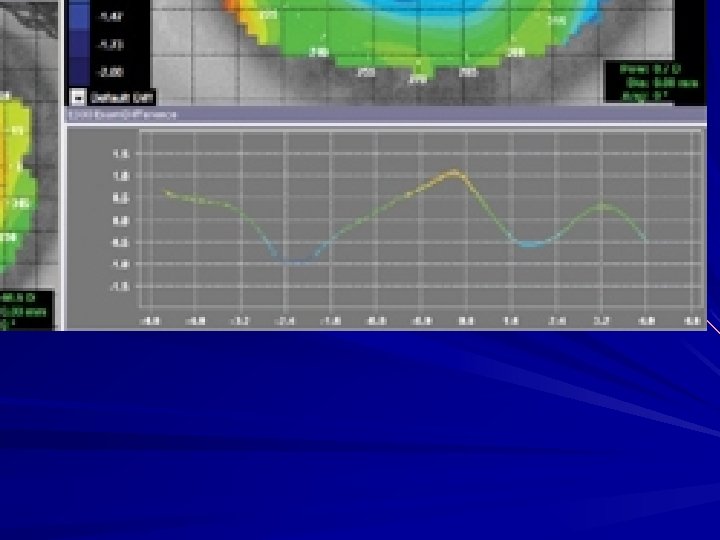
Central Islands Small, central, focal area of steep cornea – 1. 5 to 3. 0 D steepness – 1. 5 to 2. 5 mm in diameter More common after PRK Symptoms: ghosting, decreased BCVA Noted few days to weeks post-op
Central Islands: causes Beam profile abnormalities (broad beam excimer lasers) Ablation plume blocks central pulses Uneven stromal hydration Material in the treatment zone: epithelium, blood or fluorescein High myopic treatment with larger OZ Persistent epithelial defect post-op
Central Islands: treatment Most resolve in 6 -12 months If they do not resolve spontaneously, treat with – small diameter PRK treament – topo-guided ablation – Custom preview lens
PRK Post-op pain – Tx: Cold AT pre-, post- and intra-operatively – BCL Delay of visual recovery Haze (especially in more myopic ablations) Scarring and keloids – MMC to stromal bed for 1 -2 mins after ablation – PF for at least 1 month – Vit C 1000 QD
Conclusions Complications should be discussed with pts prior to surgery Most LASIK complications can be managed, if they present promptly LASIK candidates can be referred to Dr. Keshet for a discount