Early Indicators of Schizophrenia Dr Jim Simm FRCPC










: Abnormalities in one or more of 5")





 due to a mental or psychological")













 • Drugs/alcohol • Adjustment disorder •")





 Antipsychotic Discontinuation and Relapse in Schizophrenia")
 90 80 70")



- Slides: 45
Early Indicators of Schizophrenia • Dr Jim Simm*, FRCPC; CCSAM • Dr Richard Tachere*, MD; MPH *Dept. of Psychiatry, University of Manitoba. CAPA Annual Conference October 30 th, 2016
Disclosure • Dr. Simm has received honorarium payments for speaking on behalf of Janssen pharmaceuticals on the treatment of schizophrenia. • Dr. Tachere has no conflict of interest to declare.
Stay Awake. . . WHY ? ? ?
Introduction: • Schizophrenia can be a terrible mental illness: Ø robs young people of their potentials; Ø tears families apart; Ø has an enormous burden on our society (financial, legal, social, etc. )
Facts: • Among the top 25 leading causes of disability globally • ~ 3% of the total burden of human disease • ~ 1% point prevalence • > 60% of patients with the first episode of the illness have persistence of symptoms & impairment in various domains of functioning.
Facts: • In Canada: - hospital bed occupancy: 1 in 12 (higher than any other single disease) - direct health & non-health care costs ~ $2 billion/yr. - indirect costs ~ $1. 4 billion/yr.
Facts: • Peak age of onset for first psychotic episode: - Males: early to mid-20 s; - Females: the late-20 s. • Early recognition and uninterrupted treatment can lead to optimal outcomes.
Outline: • Meaning of psychosis and schizophrenia; • Approaches to Assessment, Diagnosis & Treatment; • The importance of early continuous treatment; • Conclusion.
Overview • Schizophrenia is a major mental illness - the most well-known of the ‘psychotic’ disorders. • Most common age of onset is 15 -25 yrs • It affects ~ 1% of the population Ø But what exactly is “psychosis”?
Psychosis… • The term “psychosis” refers to an impairment in reality testing. • Symptoms: hallucinations, delusions, disorganized speech, behavior, etc.
The contemporary concept of psychosis (DSM 5): Abnormalities in one or more of 5 domains: • delusions, • hallucinations, • disorganized thinking (speech), • grossly disorganized or abnormal motor behavior (including catatonia), and • negative symptoms
Signs and Symptoms of Psychosis • Delusions • Hallucinations • Replaying or rehearsing conversations out loud- i. e. talking to yourself (very common sign) • Inappropriate responses - laughing or smiling when talking of a sad event, making irrational statements.
Signs and Symptoms of Psychosis • Catatonia - staying in the same rigid position for a long time, as if in a daze. • Intense & excessive preoccupation with religion or spirituality • Hypergraphia, bizarre writing with paranoid themes, conspiracy theories, etc • Frequent moves, trips, or walks that lead nowhere
Delusions • Usually paranoid: others are plotting to harm you, are monitoring you, can read your thoughts, etc. • Often accompanied by ideas of reference: events or occurrences have a special meaning to you. • Grandiose delusions, often religious in nature (more common in mania) • Somatic - infestation, bizarre somatic complaints (e. g. in psychotic depression) • Jealousy – Often delusional disorder.
Hallucinations • Auditory: most common; generally commenting on behavior, insulting comments or command hallucinations. • Often source is attributed to “talking through the wall”, radio waves; almost always human voices • These can be either inside the person's head or externally. • When external, they sound as real as an actual voice. Sometimes they come from no apparent source; at other times they come from real people who don't actually say anything.
Hallucinations… • Visual: 2 nd most common; usually misinterpretation of real objects (i. e. illusions) • Olfactory/gustatory: less common but usually of foul odour or food is spoiled or tainted. (Consider psychotic depression if this is a prominent feature). • Tactile hallucinations: rare; often of being sexually violated.
Differential Diagnosis: 3 broad groups • Psychoses: (a) due to a mental or psychological disorder (b) due to a general medical condition (c) due to a substance (medication or drug of abuse)
Examples… Mental or Psychological Other medical illnesses Substances Schizophrenia Infections Cocaine Bipolar Electrolyte imbalances LSD MDD, etc Brain tumors, etc Amphetamines, etc
DSM 5: Schizophrenia • Symptoms: 2 or more of the 5 psychotic symptoms • Duration: at least for 6 months • Functional impairment • Note: One of the obstacles to early recognition and treatment is lack of insight.
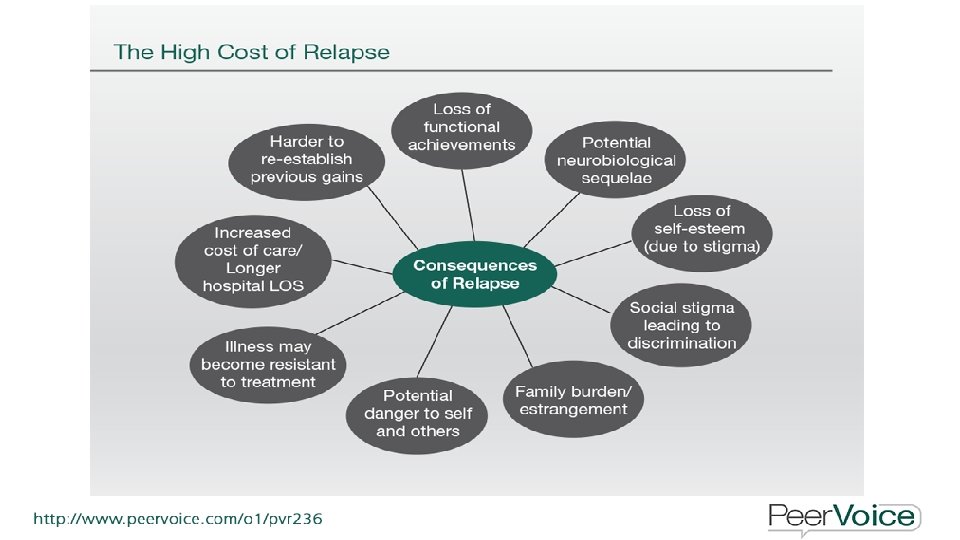
Complications of Schizophrenia • Suicidal thoughts; attempts & completed suicide; • Self-injury; • Anxiety disorders & obsessive-compulsive features; • Depression • Abuse of alcohol or other drugs, including tobacco • Inability to work or attend school
Complications of Schizophrenia • Legal and financial problems and homelessness • Social isolation • Health and medical problems • Being victimized • Aggressive behavior, although it's uncommon
So now that I’ve established that the most likely diagnosis is schizophrenia, What should I do?
Assessment • Goals of initial evaluation include: Ødevelopment of a therapeutic alliance; Øobtaining information required for diagnosis; Øidentifying factors that can assist or impede recovery
Assessment • Should include risk of: Ø suicide & deliberate self-harm Ø violence Ø neglect Ø victimization
Assessment • Should include supports available: Ø Engagement with families Ø Other relevant social networks Ø Community mental health resources available Ø Non-adherence to treatment & service disengagement.
Assessment • Goals of full medical work-up include: ØDetection of medical etiologies and/or comorbidities; ØIdentification of risk factors for possible medical disorders; ØProviding a baseline against which pharmacological complications & side-effects can be assessed.
Assessment • History is key especially family history; • Physical exam; • Investigations: ØComprehensive drug screen ØImaging: specific findings are quite rare without a neurological finding on exam; but family or patient will often insist and be unwilling to accept diagnosis until done. ØWeight, glucose, lipid profile as baseline.
Some non-specific physical findings on exam • A blank, vacant facial expression; e. g. staring while in deep thought, with infrequent blinking, etc. • Clumsy, inexact motor skills • Abnormal eye movements, e. g. difficulty focusing on slow moving objects • Unusual gestures or postures • Constant pacing • Movement could be slowed down - staying in bed (in extreme cases, catatonia)
Assessment: Investigations Type Blood Urine Imaging Others Examples CBC; extended lytes; LFT; BUN + Cr; TSH; Vit B 12. Urinalysis; street drug screen CT, MRI & EEG (where indicated) *Case-specific (e. g. syphilis, HIV, LP, etc. ) *If considering starting antipsychotics, then: lipid profile & FBS.
Non-specific early symptoms • Withdrawal from friends and family • A drop in performance at school • Trouble sleeping • Irritability or depressed mood • Lack of motivation
Non-specific early symptoms (other psychiatric disorders to consider) • Drugs/alcohol • Adjustment disorder • Mood disorder • Personality Disorder • ADHD (usually history of early difficulties in school) • Social anxiety disorder, etc.
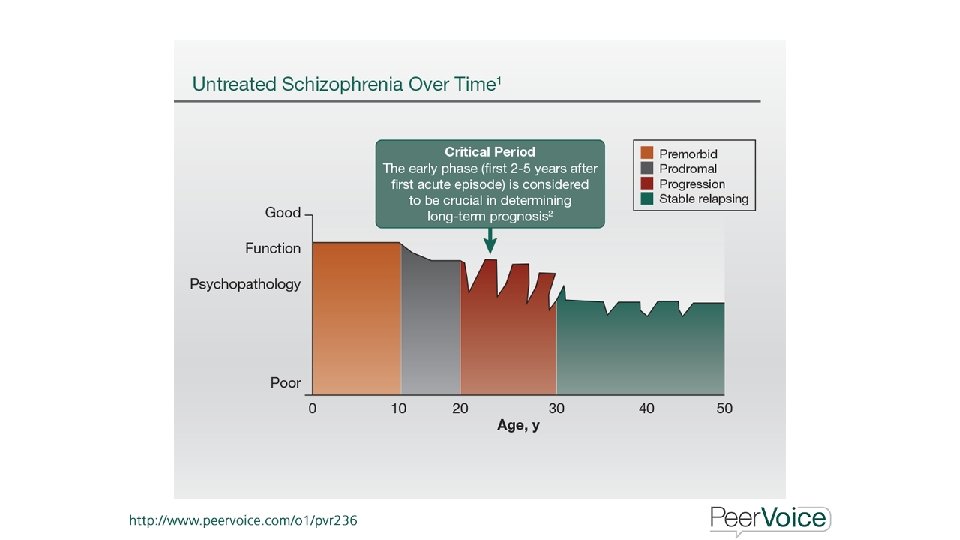
• Early recognition and uninterrupted treatment can lead to optimal outcomes.
Prodromal Stage: *Early detection & interventions* Stage Prodromal Transition rate: *22% within one year *36% within three years Symptoms *Significant decrease in functioning PLUS identified genetic risk or personality traits (schizoid or schizotypal) *Attenuated psychotic symptoms *Transient psychotic symptoms (brief in duration & remit spontaneously) *Others: substance use; ADHD; anxiety; social withdrawal, etc.
Progressive Stage: Stage Progressive Symptoms *Overt psychosis *Deterioration in symptoms (the 5 domains in DSM 5) *Deterioration in brain abnormalities (thinning of frontal cortex; lateral ventricular enlargement; reduction of white matter integrity, etc. ) *Relapses & remissions clinical deterioration.
Chronic/Residual Stage Symptoms Chronic/Residual *Generally: poor functioning; social & occupational disability. *Progression of brain abnormalities *Outcomes are heterogeneous.
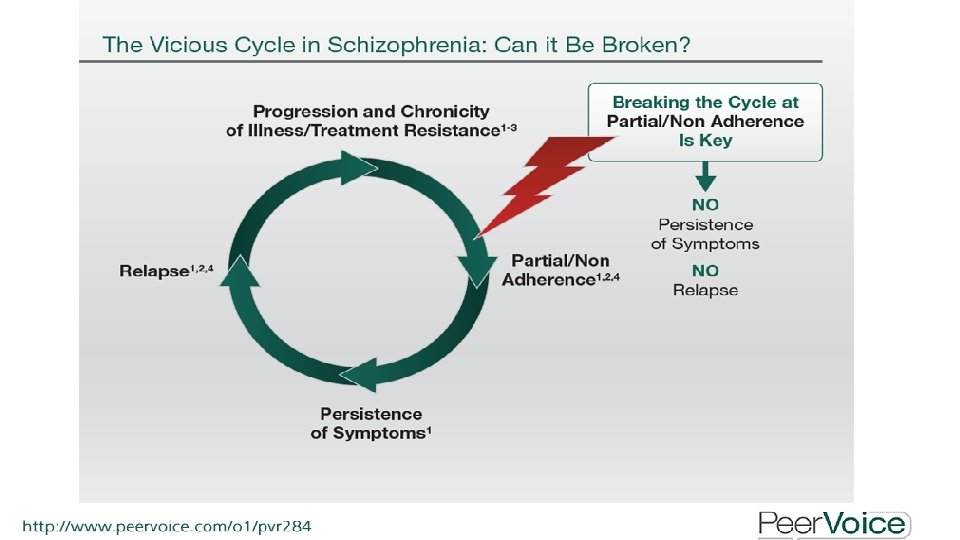
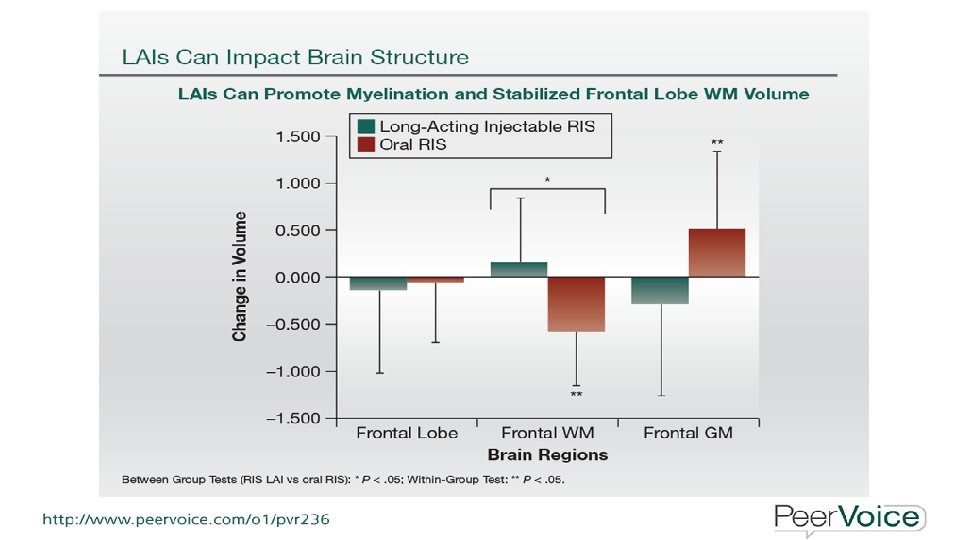
Clear evidence that early uninterrupted intervention decreases the burden of illness v. Reduces # of relapses & hospitalizations v. Higher functioning v. Preservation of grey matter
Patients without psychotic symptom exacerbation or relapse (%) Antipsychotic Discontinuation and Relapse in Schizophrenia 1. 0 0. 8 Relapsed 0. 6 0. 4 Remaining well 0. 2 0 0 12 24 36 48 Week 60 72 Gitlin M, et al. Am J Psychiatry 2001; 158: 1835– 42
Adherence to Treatment Among Outpatients With Schizophrenia 100 Adherence Rate (%) 90 80 70 60 50 40 30 Self-Report Clinician rating Pill Count Adherence Measure *Medication Event Monitoring System (MEMS®) Remington G. et al. Scz Res 2007. MEMS*
Enhancing Adherence • Patient engagement and active involvement; • Clear, simple instructions; (people recall at best 50% of what was said during appointments, and the 50% recalled is often not the same 50% as the clinician wanted to emphasize); • No blame environment; • Enquire about financial barriers.
Enhancing Adherence • If you give out reading material, make sure that the patient and family can understand it; • The best results are seen with Long Acting Injectables.
Conclusions • Schizophrenia can be a devastating illness for the patient, family & society; • Early recognition AND early uninterrupted treatment are crucial to long term positive outcomes.