Mechanical Ventilation 101 Dr Paul Healey ICU Fellow







 modes: – Continuous Positive Airways")






 • Pressure")






































 Opening Pressure Collapse Superimposed Pressure Inflated Small")
 given continuously via an ultrasonic")





 • Involves gas exchange via an extracorporeal")






- Slides: 95
Mechanical Ventilation 101 Dr Paul Healey ICU Fellow John Hunter Hospital Newcastle
Outline • • What is mechanical ventilation ? History of mechanical ventilation. Why do we mechanically ventilate patients ? Modes of mechanical ventilation ? Setting the ventilator Trouble shooting ventilation Refractory Hypoxaemia When to extubate the patient ?
Mechanical ventilation • Is a method to mechanically assist or replace spontaneous ventilation. • Is a supportive therapy. • Two main divisions of mechanical ventilation 1. Negative pressure ventilation 2. Positive pressure ventilation
Polio epidemic – Copenhagen 1952
Positive pressure ventilation
Mechanical ventilation Positive pressure ventilation • Non-invasive ventilation (NIV) modes: – Continuous Positive Airways Pressure (CPAP) – Bi-level Positive Airways Pressure (Bi. PAP) • Invasive positive pressure ventilation (IPPV) modes: – Volume Control Ventilation (VCV) – Pressure Control Ventilation (PCV) – Pressure Support Ventilation (PSV)
Case study • Mr CS – 75 year old male, weighs 80 kg. • Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. • Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. • Currently ventilated in OT on Fi. O 2 50% PCV-VG 14 x 480 m. L, with PEEP of 6 cm. H 2 O. • Vital signs: HR 115, BP 110/50 on 0. 2 mcg/kg/min of Noradrenaline, Sa. O 2 96%, temperature 38. 8 degrees. • Last ABG: p. H 7. 32, Pa. O 2 92 mm. Hg, Pa. CO 2 35 mm. Hg, Lactate 2. 2 mmol/l and BE -5. 3 mmol/l • What is the reason for mechanically ventilating this patient ? ? • What are the risks of mechanical ventilation ? ?
Why do we mechanically ventilate patients ? • Indications for mechanical ventilation – Impaired level of consciousness – Potential airway compromise – Respiratory failure • Hypoxaemic • Hypercapnoeic – Work of breathing and fatigue – Cardiac failure
Risks of mechanical ventilation 1. Respiratory Complications • Infection – Ventilator Associated Events • Ventilator Induced Lung Injury (VILI) – Barotrauma – Volutrauma – Atelectotrauma • Gas trapping and intrinsic PEEP • Oxygen toxicity 2. Non-respiratory complications • Haemodynamic compromise • Raised ICP • Reduced urine output
Modes of ventilation
Modes of invasive ventilation Nomenclature • Triggering – what initiates a breath – Ventilator – Patient • Inspiration – Volume – Pressure • Cycling – what determines change from inspiration to expiration – Volume – Time – Flow • Exhalation – Passive process due to lung elastic recoil
Modes of ventilation • Classification based on patient triggering: 1. Mandatory ventilation modes 2. Spontaneous ventilation modes 3. Adaptive ventilation modes
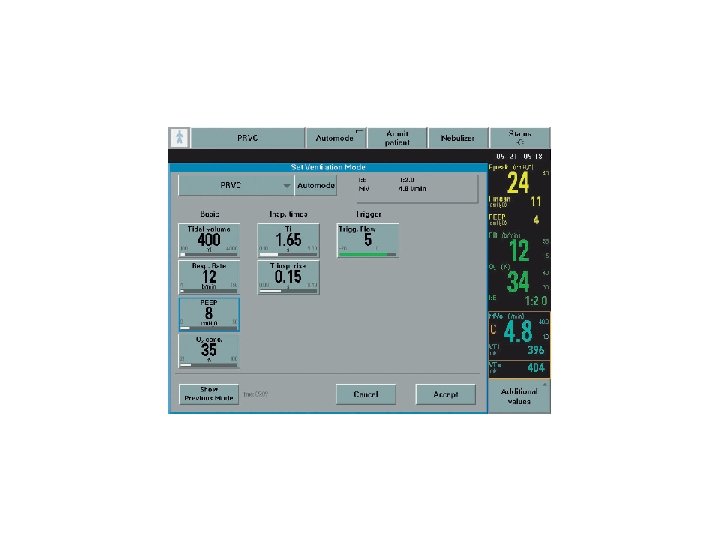
Modes of ventilation 1. Mandatory ventilation modes • Volume control ventilation (VCV) • Pressure control ventilation (PCV) • Synchronised Intermittent Mandatory Ventilation (SIMV)
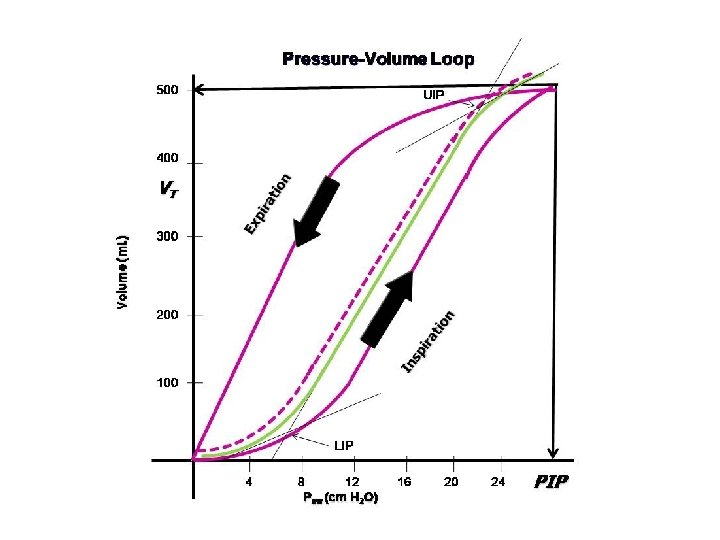
Ventilator waveforms
Volume Control Ventilation
Modes of ventilation 1. Mandatory modes • Volume control ventilation – All breaths given are the same preset volume • Advantages – Relatively simple to set – Guaranteed minute ventilation – Rests respiratory muscles • Disadvantages – Historically, no patient triggering – Ventilator-patient dysynchrony – Reduced lung compliance will result in increased pressures and potential barotrauma
PCV
Modes of ventilation 1. Mandatory modes • Pressure control ventilation – All breaths have same preset inspiratory pressure and time • Advantages – Simple to set – Avoids high inspiratory pressures – Rests respiratory muscles • Disadvantages – Historically, no patient triggering – Change in lung compliance results in change in tidal volumes – No guaranteed minute ventilation
SIMV
SIMV
Modes of ventilation 1. Mandatory modes • SIMV - Mandatory VCV or PCV with triggered PSV • Advantages - Better patient-ventilator synchrony - Guaranteed minute ventilation - Allows patient triggering and possible weaning • Disadvantages - More complicated mode with multiple settings
PSV
Modes of ventilation 2. Spontaneous ventilation modes • Pressure support ventilation – Provides a set inspiratory and expiratory pressure during patient initiated breathing – Inspiration ends when inspiratory flow falls to a preset level (usually 25%) • Advantages – Maintains full spontaneous ventilation – Better ventilator-patient synchrony – Weaning mode of ventilation • Disadvantages – Historically no back-up ventilation – Changes in patient effort and lung compliance effect tidal volumes
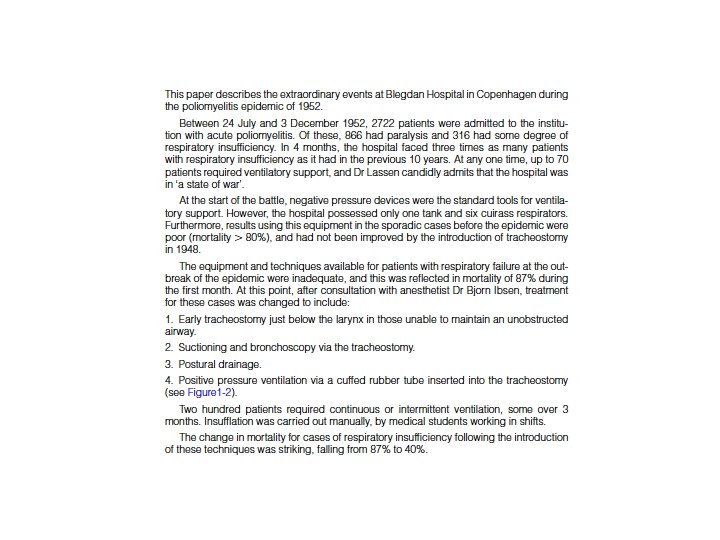
PRVC
Mechanical ventilation 3. Adaptive ventilation modes – Assist – Pressure regulated volume control – PCV - VG
Case study • Mr CS – 75 year old male, weighs 80 kg. • Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. • Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. • Currently ventilated in OT on Fi. O 2 50% PCV-VG 14 x 480 m. L, with PEEP of 6 cm. H 2 O. • Vital signs: HR 115, BP 110/50 on 0. 2 mcg/kg/min of Noradrenaline, Sa. O 2 96%, temperature 38. 8 degrees. • Last ABG: p. H 7. 32, Pa. O 2 82 mm. Hg, Pa. CO 2 35 mm. Hg, Lactate 2. 2 mmol/l and BE -5. 3 mmol/l • How are you going to set the ventilator ? ? • What other information would you want to know ? ?
Setting the ventilator • • • Fi. O 2 Mode Triggering Tidal volume Inspiratory pressure PEEP • • • Respiratory rate Inspiratory time I: E ratio Inspiratory flow Alarm settings – Peak pressure – PEEP – Minute ventilation
How to set a ventilator • Fi. O 2 • – Begin at 100% and wean as quickly as able to < 60% • Mode – Volume controlled ventilation • Set tidal volume 6 – 8 m. L/kg – Start at 10 – 12 breaths per minute • • • – Flow triggering : 1 – 5 L/min – Pressure triggering: -0. 5 to -2. 0 cm. H 2 o • Inspiratory pressure (Plateau) – Aim < 30 cm. H 2 O. – VCV or SIMV = plateau pressure – PCV = Sum of PEEP and Inspiratory pressure • PEEP – Start with 5 -10 cm. H 20 I: E ratio – Normally 1: 2 – Increase in obstructive airways disease (COPD/Asthma) Set inspiratory pressure 10 – 20 cm. H 2 O Triggering Inspiratory time – Normal 0. 8 – 1. 3 seconds – Pressure controlled ventilation • Respiratory rate • Inspiratory flow – 40 – 60 L/min
Case study • Mr CS – 75 year old male, weighs 80 kg. • Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. • Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. • Currently ventilated in OT on Fi. O 2 50% PCV-VG 14 x 480 m. L, with PEEP of 6 cm. H 2 O. • Vital signs: HR 115, BP 110/50 on 0. 2 mcg/kg/min of Noradrenaline, Sa. O 2 96%, temperature 38. 8 degrees. • Last ABG: p. H 7. 32, Pa. O 2 82 mm. Hg, Pa. CO 2 35 mm. Hg, Lactate 2. 2 mmol/l and BE -5. 3 mmol/l • How are you going to set the ventilator ? ? • What other information would you want to know ? ?
Setting the ventilator • • • Fi. O 2 Mode Triggering Tidal volume Inspiratory pressure PEEP • • • Respiratory rate Inspiratory time I: E ratio Inspiratory flow Alarm settings – Peak pressure – PEEP – Minute ventilation
What is the evidence ? ?
Ventilation modes - evidence • A single RCT and 3 observational trials • There were no statistically significant differences in mortality, oxygenation, or work of breathing • PCV – lower peak airway pressures – a more homogeneous gas distribution (less regional alveolar over distension) – improved patient-ventilator synchrony – earlier liberation from mechanical ventilation than volumelimited ventilation • VCV – it can guarantee a constant tidal volume, ensuring a minimum minute ventilation
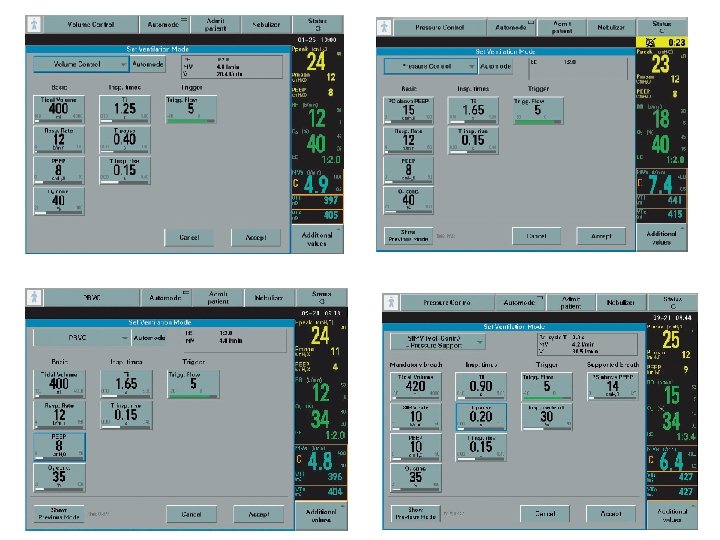
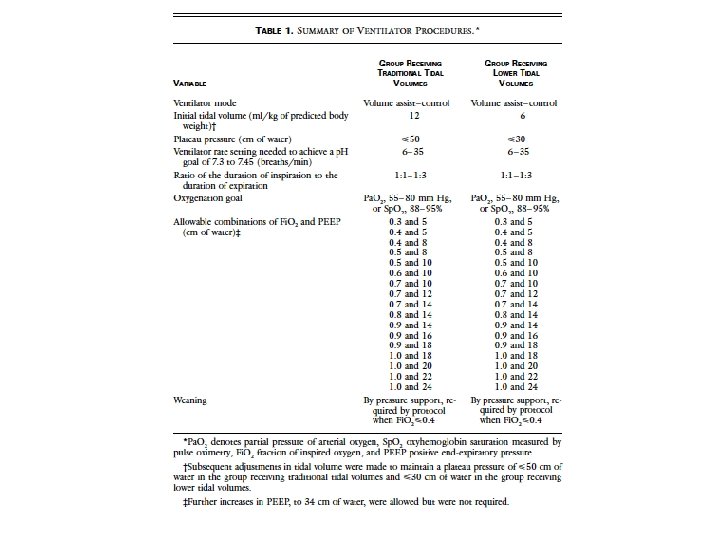
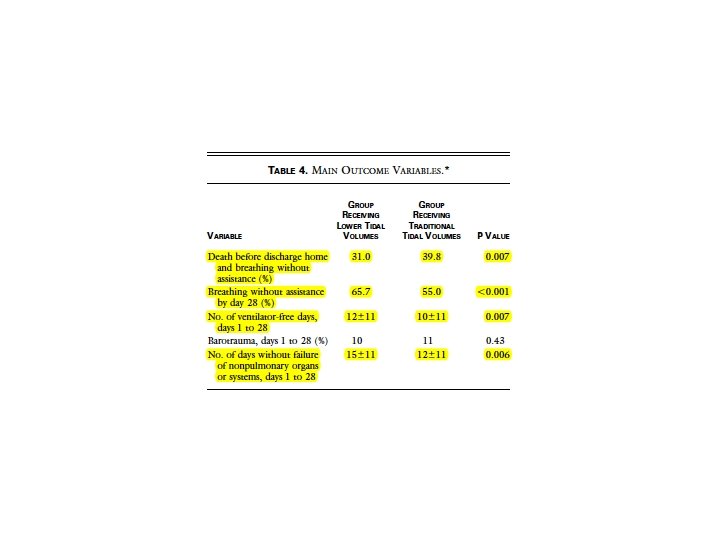
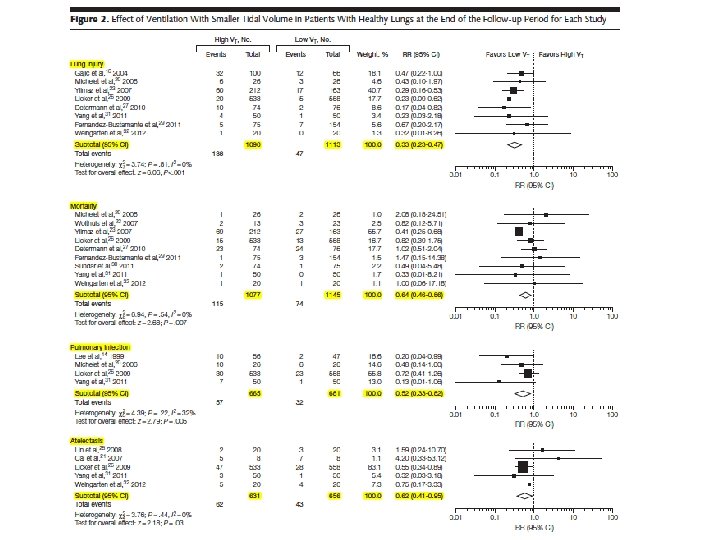
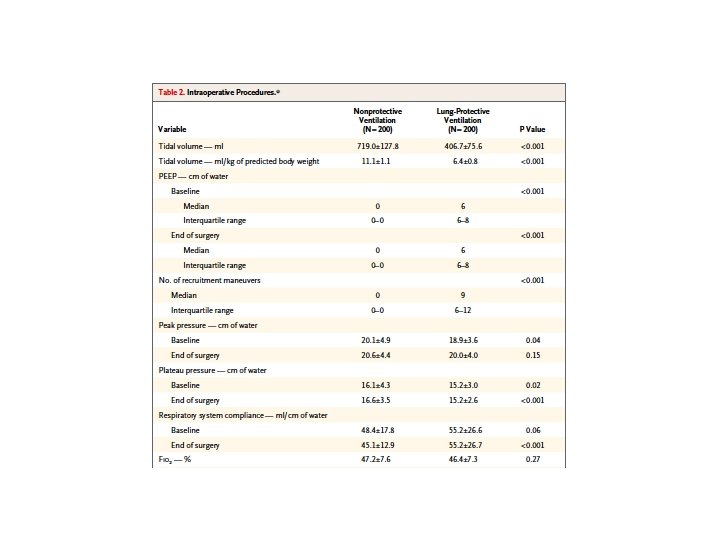
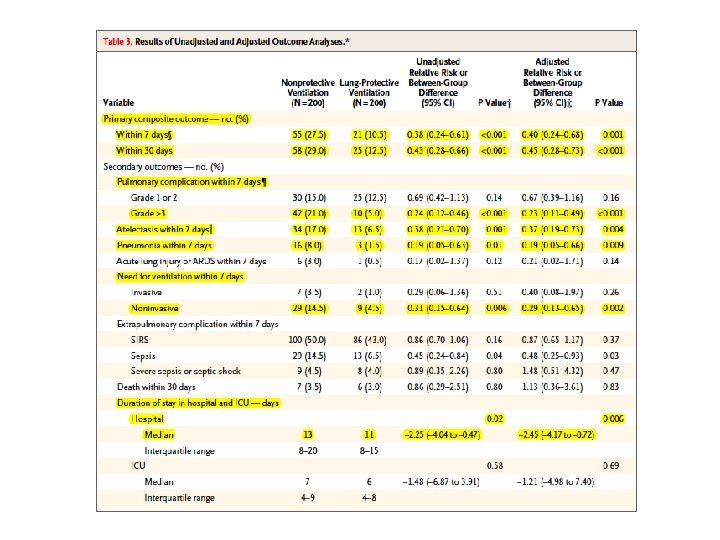
Evidence for ventilation
Evidence for ventilation
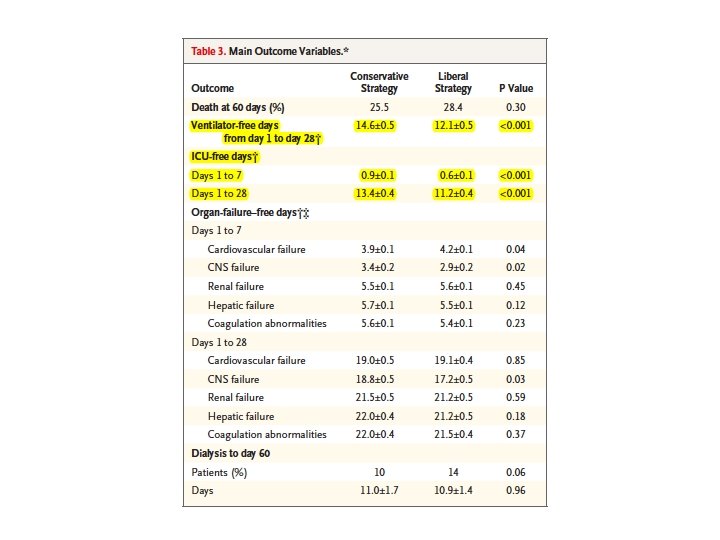
Evidence for ventilation –FACCT trial
Trouble shooting ventilation
Case study • Mr CS – 75 year old male, weighs 80 kg. • Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. • Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. • Vital signs: HR 115, BP 110/50 on 0. 2 mcg/kg/min of Noradrenaline, Sa. O 2 96%, temperature 38. 8 degrees. • The nursing staff come to you after one hour and show you the following ABG: – p. H: 7. 21, Pa. O 2 82 mm. Hg, Pa. CO 2 58 mm. Hg, Lactate 2. 1 mmol/l, BE 5. 2 mmol/l • How will you adjust the ventilator ? ?
Trouble shooting ventilation • We need to increase minute ventilation • Minute ventilation = TV x RR
Trouble shooting ventilation 1. Dead space ventilation - Excess tubing, especially in paediatrics 2. Tidal volume – Aim 6 -8 m. L/kg – Risk of barotrauma if plateau pressure > 30 cm. H 2 O – Risk of volutrauma 3. Respiratory rate – Aim for < 30 – Monitor for gas trapping, dynamic hyperinflation and intrinsic PEEP
Trouble shooting ventilation
Trouble shooting ventilation
Case study • Mr CS – 75 year old male, weighs 80 kg. • Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. • Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. • Vital signs: HR 130, BP 90/50 on 0. 3 mcg/kg/min of Noradrenaline, Sa. O 2 96%, temperature 38. 8 degrees • He is ventilated in ICU, and adjustments made after the last ABG. • The nursing staff come to you later that shift stating the patient has desaturated to 85% and shows you the following ABG: • p. H 7. 30, Pa. O 2 52 mm. Hg, Pa. CO 2 40 mm. Hg, lactate 2. 0 mmol/l, BE 5. 1 mmol/l • How will you manage this ? ?
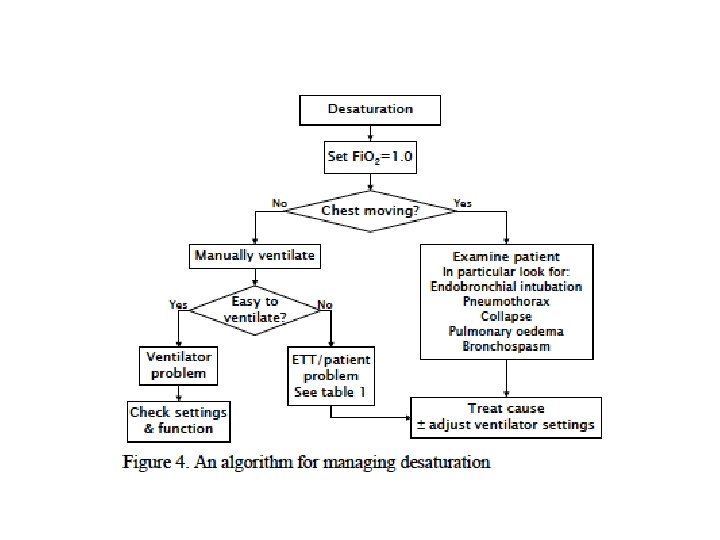
Trouble shooting ventilation • Hypoxaemia • Most patients need Sa. O 2 90 -94% at the most, some only 88 -92% (chronic respiratory disease) • What to do ? ?
Patient is still hypoxic !
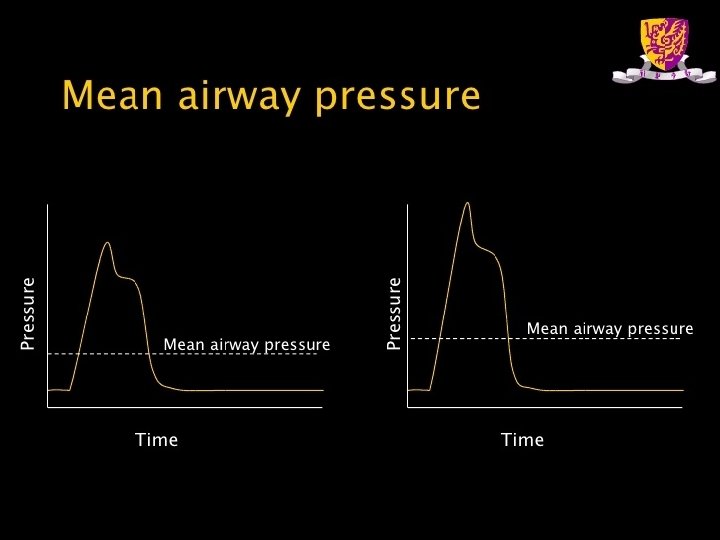
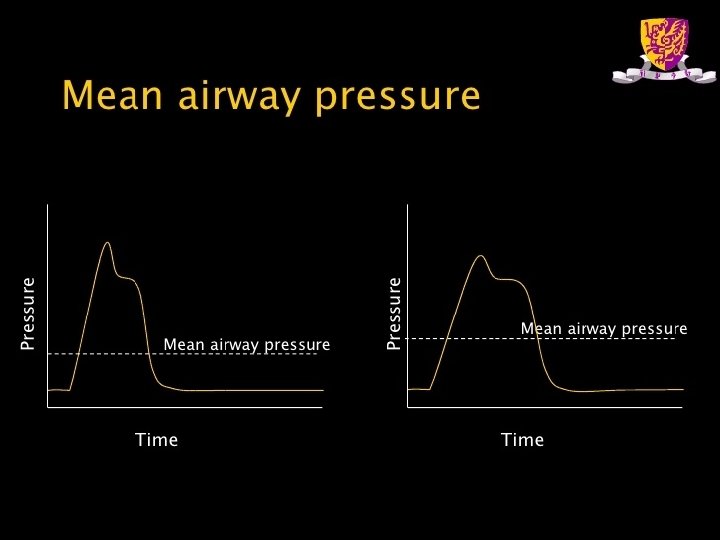
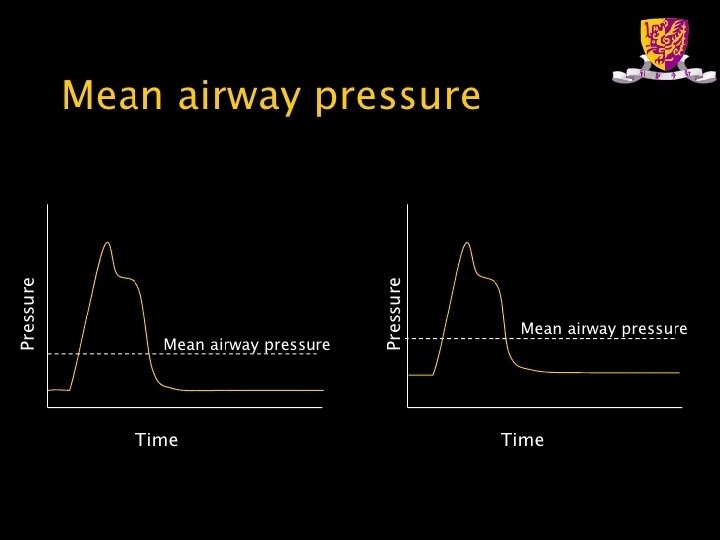
Trouble shooting ventilation • Increase Fi. O 2 • Increase mean alveolar pressure – Main determinant of oxygenation – Can be increased by increasing • Inspiratory pressure or tidal volume • Inspiratory time • PEEP • Increase PEEP – Maintains open alveoli and reduces shunt
What if Sa. O 2 is still only 85% ? ?
Refractory hypoxaemia
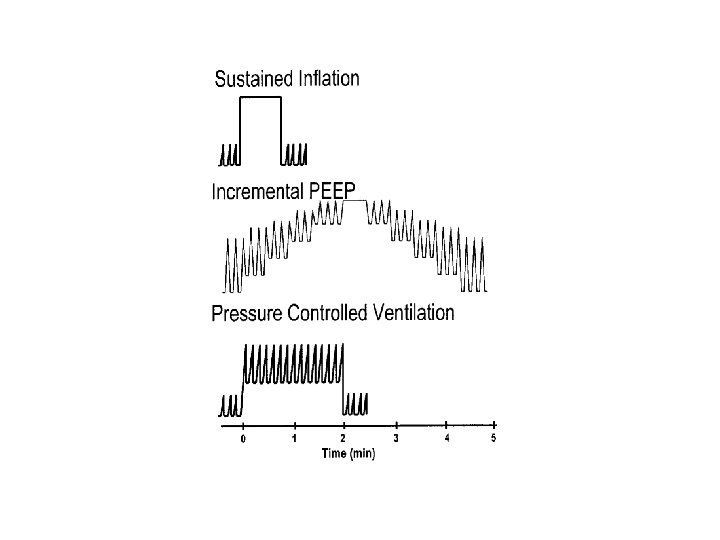
Refractory hypoxaemia 1. Recruitment maneuvers • Is a high pressure inflation maneuver aimed at temporarily raising the transpulmonary pressure above levels typically obtained with mechanical ventilation. • Purpose is to overcome the high “opening pressures” of diseased and collapsed alveoli. • By opening alveoli, this increases the area available for gas exchange and oxygen transfer.
Spectrum of Regional Opening Pressures (Supine Position) Opening Pressure Collapse Superimposed Pressure Inflated Small Airway Alveolar Collapse (Reabsorption) Consolidation = Lung Units at Risk for Tidal Opening & Closure 0 10 -20 cm. H 2 O 20 -60 cm. H 2 O
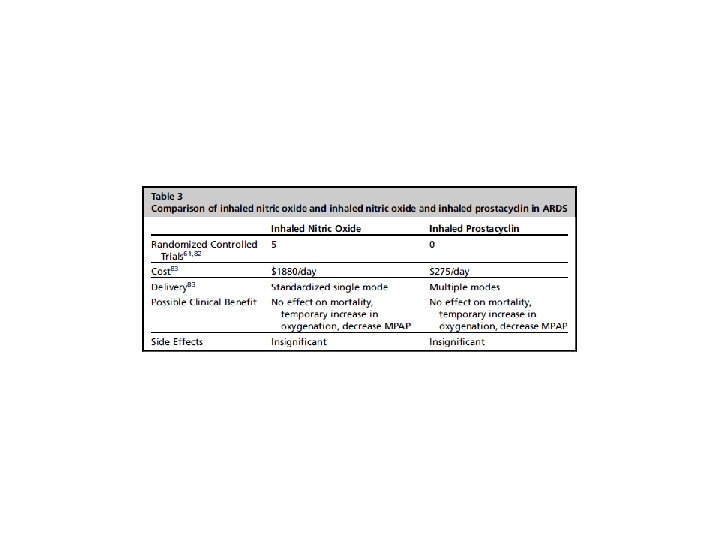
Refractory hypoxaemia 2. Inhaled prostacyclin • Nebulised prostacylin (PGI-2) given continuously via an ultrasonic nebuliser attached to the inspiratory limb of the ventilator. • An alternative to inhaled Nitric Oxide which is expensive and requires scavenging set-up.
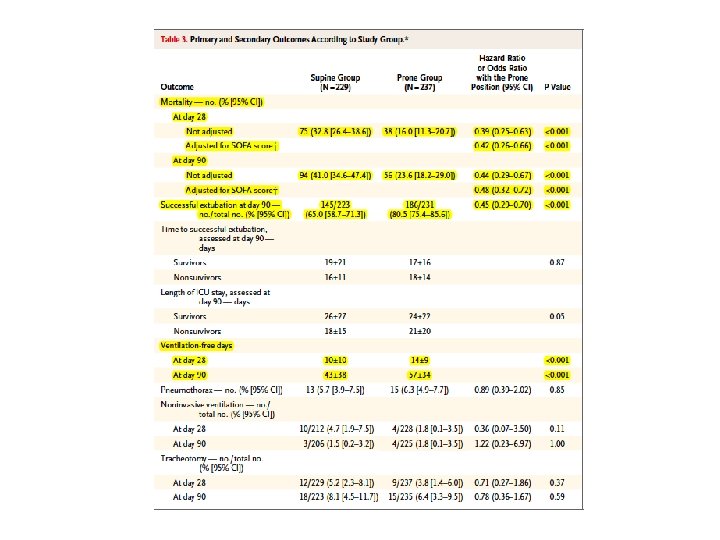
Refractory hypoxaemia 3. Prone ventilation • Has been studied in severe ARDS • Complex process with safety issues – Risk of extubation – Risk of removing lines – Pressure areas – OH and S
PROSEVA trial
Refractory hypoxaemia 4. High frequency oscillatory ventilation • Specialised equipment • Respiratory rates of 5 -15 Hz • Mean airway pressures of 30 cm. H 2 O • Tidal volumes smaller than dead space ! • Effective at rescue oxygenation
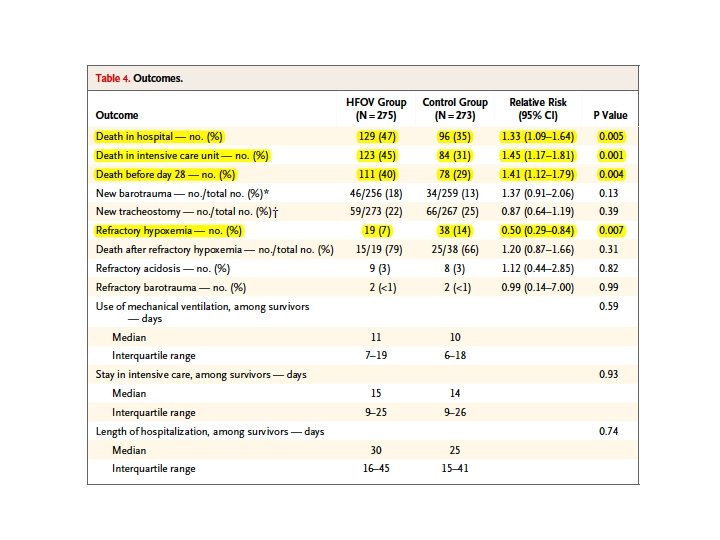
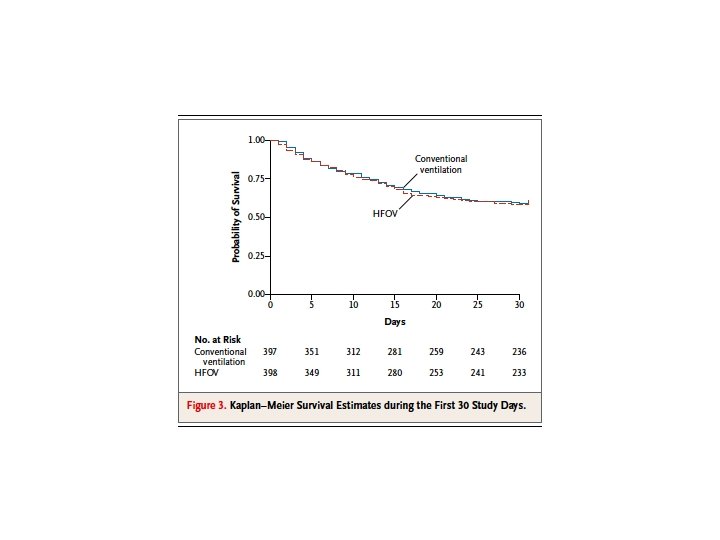
OSCILLATE trial
OSCAR trial
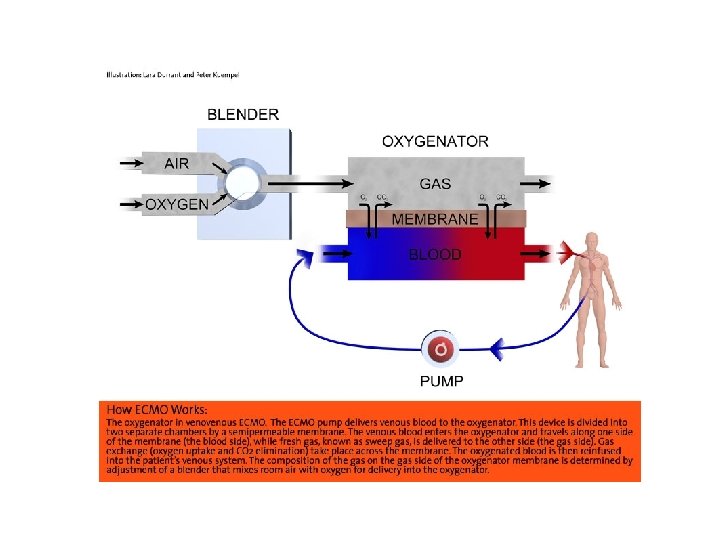
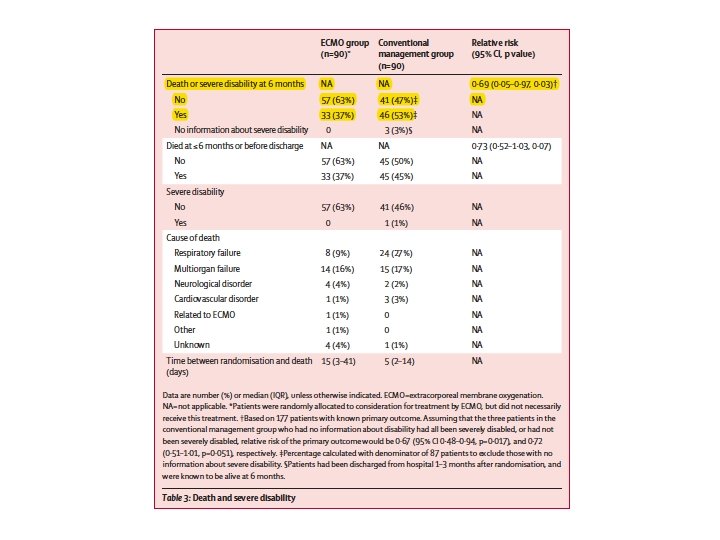
Refractory hypoxaemia 5. Extracorporeal Membrane oxygenation (ECMO) • Involves gas exchange via an extracorporeal circuit. • Can support the lungs alone (V-V ECMO) or the heart and lungs (V-A ECMO) • Significant risks and costs
CESAR trial
Case study • • Mr CS – 75 year old male, weighs 80 kg. Background – IHD, Ex-smoker 20 years ago, Type II DM, AF. • • • Day 4 post Hartmans procedure for colorectal cancer, severe abdominal pain and fever. Anastamotic leak on CT scan. Commenced on IV Tazocin. Taken to OT and had extensive washout of abdomen and stoma formed. Abdomen is closed. He has been ventilated in ICU for 5 days. He had a brief period of hypoxaemia due to bibasal atelectasis. It resolved with a recruitment maneuver and increased PEEP. He has been on PSV for 24 hours, with settings Fi. O 2 30%, Inspiratory pressure 10 cm. H 2 O and PEEP 5 cm. H 2 O. His vital signs are: HR 90, BP 130/70, Sa. O 2 98%, temperature 37. 2 degrees His latest blood gas shows: – p. H 7. 38, Pa. O 2 95 mm. Hg, Pa. CO 2 39 mm. Hg, lactate 0. 7 mmol/L and BE 1. 0 mm 0 l/L • • How will you assess him for extubation ? ? Should you extubate him onto NIV ? ?
Assessment for extubation 1. Disease process – Has disease process that required MV resolved – Complications – sepsis, transfusion – Pain – especially with thoracotomy, laparotomy – Fluid balance : ideally cummulative balance < 3 L 2. Airway – Grade of intubation – How patient was intubated – Presence of cuff leak – Appropriate assistance available
Assessment for extubation 3. Neurological – Awake and co-operative – Pain controlled – Weakness 4. Respiratory – – – – Ventilator support – ideally PSV < 10/5 cm. H 2 O RR <30 Vital capacity > 10 m. L/kg Cough Secretion load – small load Rapid shallow breathing index (f/Vt) <100 Review of CXR 5. Cardiovascular – Stable cardiac rhythm – Minimal ionotrope/vasopressor requirement
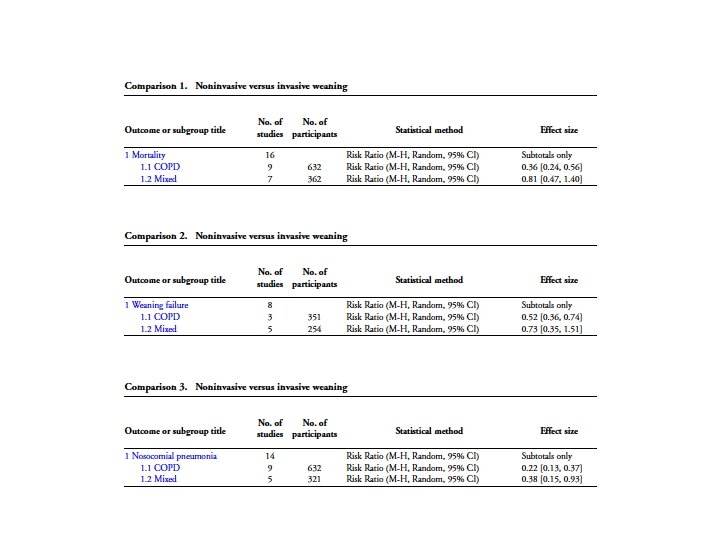
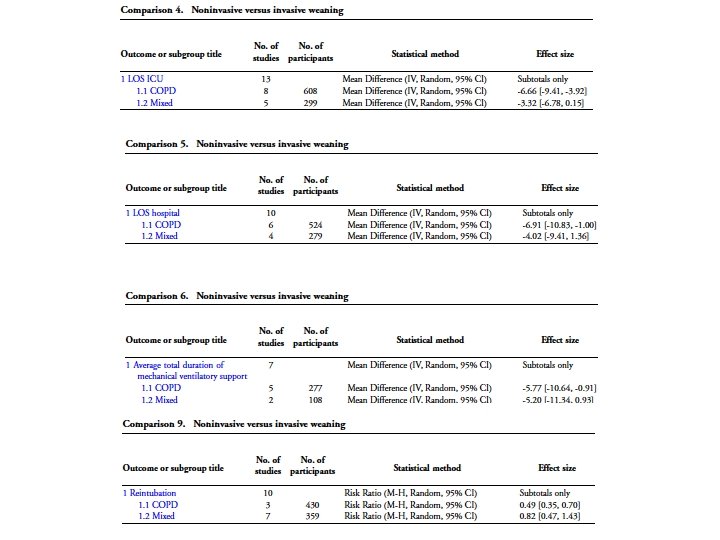
Extubation onto NIV
Conclusion • Modes of ventilation – Mandatory – Spontaneous – Adaptive • • • How to set the ventilator Evidence for ventilator strategies Trouble shooting ventilation Refractory Hypoxia Assessment for extubation