KIDNEY TRANSPLANT AND NEPHROSTOMY TUBES Kidney transplantation A

KIDNEY TRANSPLANT AND NEPHROSTOMY TUBES

Kidney transplantation � � A kidney transplant is a surgical procedure to place a kidney from a live or deceased donor into a person whose kidneys no longer function properly. A kidney transplant is often the best treatment for kidney failure for both adult and pediatric patients. Kidney transplant survival rate with a 1 year graft is over 90% for a deceased donor transplant and 95% for live donor transplant. A kidney transplant often reverses the pathophysiological problems that are associated with Kidney failure and it eliminates the patient’s dependence on dialysis. This leads to less dietary and lifestyle restrictions.

Interesting facts about kidney transplant � � Fewer than 4% ever receive a transplant (high disparity between supply and demand for kidneys) More than 93, 000 are on the waiting list, but only ¼ receive a kidney

Indications for kidney transplant � � � � End-stage kidney disease. ESKD occurs when GFR is <15 ml/min. At this point dialysis or transplant is needed to sustain life. These are some conditions that lead to ESKD: Diabetes Hypertension Glomerulonephritis Pyelonephritis Polycystic kidney disease Obstructive uropathy Congenital urinary tract abnormalities � � � � � Alport's disease Hypertensive nephrosclerosis Reflux nephropathy Interstitial nephritis Ig. A nephropathy Goodpasture's syndrome Hemolytic uremic syndrome Chemical nephrotoxicity Renal artery emboli Sickle cell nephropathy

Advantages of Kidney transplant over dialysis � Resume normal lifestyle � Return to normal diet. On dialysis they require a diet that is high-protein, low-phosphorus, low-potassium, low-sodium, and fluid-restricted. � More free time & less time in dialysis clinics or doing treatments at home � � � Reverses many of the pathophysiologic changes associated with renal failure Decreases mortality rate Cost is cheaper after the first year

Suitable recipient for kidney transplant � 3 factors: 1. Blood type: Type A, B, AB, or O must be compatible with the donor’s blood type. 2. HLA: Human Leukocyte Antigen: A Protein/Genetic Marker found on the surface of your cells, a higher number of matching antigens with a donor increases the chances that the kidney will last a long time. (Individuals receive 3 HLA’s from mother and father, 6 Total)

Suitable recipient cont. 3. � � Antibodies: Small sample of a recipient’s blood will be mixed with the donor’s blood to see if a reaction occurs(type and match) A Negative Crossmatch is Good! Positive crossmatch means a recipient has cytotoxic antibodies to the donor and the organ would undergo hyperacute rejection.

Donor sources � 1. 2. 3. 4. 5. May be obtained from Compatible blood-type deceased donors Blood relatives Emotionally related Living Donors(spouse, friend) Paired Organ Donation “One Kidney Island” - Cash for Kidney Trade! Filipinos living in slums sell their kidneys for cash due to poverty - Foreigners visit the Philippines to buy a kidney for transplant

“One Kidney Island”

Criteria for deceased donor’s kidney � � 1. 2. 3. 4. UNOS: United Network for Organ Sharing distribute kidney based on an objective computerized point system. Points are given based on: How close HLA match is How long patient has been waiting Antibody level is high(extra points here because high antibody levels severely limit the number of donors with whom the patient will not have a positive crossmatch) Recipient is younger than 19 years old

Diagnostics for kidney transplant � Diagnostic Testing: � CT Scan with contrast � Proteinuria � Hematuria � Elevated BUN levels � Elevated Serum Creatinine � Elevated potassium and phosphorus levels � Decreased GFR � Decreased hemoglobin and hematocrit � Sodium normal, increased, or decreased.

Pre-operative care � � � Assess and acknowledge feelings about the procedure, answering questions and clarifying information as needed Listen and address concerns about surgery from both recipient and donor Continue dialysis as ordered Peritoneal Dialysis must empty the peritoneal cavity of all dialysis solution before surgery Ensure Patient is in optimal physical health for surgery: ECG, x-ray, blood testing or bladder augmentation or other GI surgeries Immunosuppressant therapy

Immunosuppressant therapy preop � � � Administer immunosuppressive drugs as ordered before surgery Immunosuppression is initiated before transplantation to prevent immediate graft rejection Most patients are initially on triple therapy which usually consists of a calcineurin inhibitor, a corticosteroid, and a mycophenolate mofetil.

Surgical procedure � � Live Donor: � Account for 27 % of all transplants. � Begins 1 -2 hours before recipient’s surgery. Laparoscopic donor nephrectomy � Most common technique. � Fever risk, shorter recovery time. � Decreased hospital stay, pain, operative blood loss, debilitation, and length of time off work. Open donor nephrectomy: � Donor placed in lateral decubitus position on the operating table exposing flank. � Incision is made at 11 th rib, removed of rib to provide visualization of kidney. Kidney is removed flushed with a chilled sterile electrolyte solution and prepared for immediate transplant into recipient.

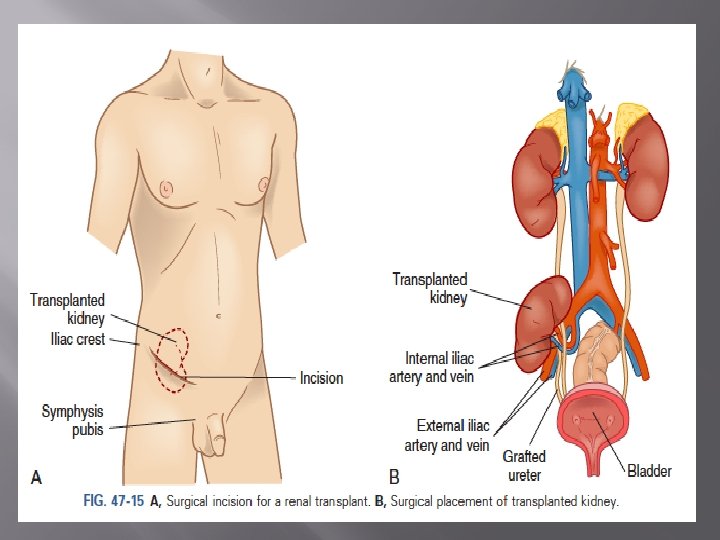
Surgical procedure cont. � Kidney transplant recipient: 3 -4 hours’ surgery. Installation of antibiotics in bladder to decrease risk of infection through catheter. � Crescent –shaped incision is made extending from the iliac crest to the symphysis pubis. � Transplanted kidney is usually placed extraperitoneally in the right ilia fossa. � Anastomoses of the blood vessels and ureter and minimize the occurrence of paralytic ileus Rapid revascularization is critical to prevent ischemic injury to kidney.

Post-op care for donor patient � � � Monitor renal function to assess for impairment and monitor hematocrit to assess for bleeding. Pain management: donors have more pain than their recipients do Urine output � Retention of fluid can increase the work required of the remaining kidney to perform its function. � Respiratory status � Ensure adequate ventilation � Incentive spirometers are used every � Frequent and early ambulation assist adequate respiratory function. � Abdominal distention � Oral � 2 hours. in maintaining intake is restricted until bowel sounds are present Discharge from the hospital 2 -5 days

Post op care for recipient patients � Maintenance of fluids and electrolytes � � � Urine output during this phase may be as high as 1 L/hr and gradually decrease as the BUN and creatinine levels return toward normal. Urine output is replaced w/fluids ml per ml for the first 12 -24 hours Monitor dressing for drainage Rapid diuresis d/t new kidney’s ability to filter BUN � � hyponatremia and hypokalemia r/t rapid diuresis metabolic acidosis may develop r/t delayed kidney function A sudden decrease in urine output in the early postoperative period is a cause for concern. Postoperative teaching � How to recognize signs of rejection, infection, and any complications of surgery.

Immunosuppressant therapy post op � � � Requires a balance - adequately suppress the immune response to prevent rejection while maintaining sufficient immunity to prevent infection Transplant recipients require life time immunosuppressant therapy - increase risk of toxicity Children: poor medication adherence d/t undesirable side effects - ex: cosmetic side effects
 and tacrolimus (Prograf) -")
Common immunosuppressant medications � Calcineurin inhibitors � - cyclosporine (Neoral) and tacrolimus (Prograf) - most effective � - Muromonab-CD 3 - cell lysis and inhibts function of cytotoxic T cells Antiproliferative drug - sirolimus (Rapamune) and mycophenolate mofetil (Cell. Cept) - decrease # and activity of T and B cells and suppresses immune response by blocking purine synthesis (Azathioprine) Monoclonal antibodies � Polyclonal antibody - Lymphocyte immune globulin (Atgam) - prepared by immunizing horse with human T cells � Corticosteriods - prednisone

Calcineurin inhibitors � � � � � Calcineurin inhibitors prevent a cell-mediated attack against the transplanted organ. Tacrolimus (Prograf®) is the most widely used. It also includes cyclosporine (Neoral). Drug levels are monitored to prevent toxicity Side effects: Kidney dysfunction High blood pressure High potassium in the blood Increased sugar level in the blood (drug-induced diabetes) Tremors Headaches Insomnia

Corticosteroids � � � � � Corticosteroid suppresses inflammatory response. Inhibits cytokine production. Prednisone is taken PO or IV. Prednisone is taken in low doses to minimize side effects Side effects: Weight gain Irritation of stomach lining Increase risk of bruising and infections Increase blood glucose levels Decrease healing time Mood changes Generalized weakness
 Mycophenolate mofetil")
Antiproliferative drugs � � � These include Mycophenolate mofetil and sirolimus (Rapamune) Mycophenolate mofetil is a lymphocyte-specific inhibitor of purine synthesis with suppresses proliferation of T and B lymphocytes and sirolimus suppresses T cell activation and proliferation. Side effects: Abdominal aches and/or diarrhea Decreased WBC count Decreased RBC count

Complications of kidney transplant � � Rejection - Hyperacute, acute or chronic rejection Infection - pneumonia, wound, IV or drain, UTI and CMV infections observed first month � � Cardiovascular disease - leading cause of death in transplanted pts Malignancies - skin cancers, Hodgkins and non-hodgkins lymphoma and Kaposi sarcoma most common � � Recurrent of original kidney disease Corticosteroid related complications - aspetic necrosis of hips, knees and other joints - after a year of transplant, dose decreases by 5 -10 mg/day - the use of corticosteroids have decreased over the years d/t adverse side effects

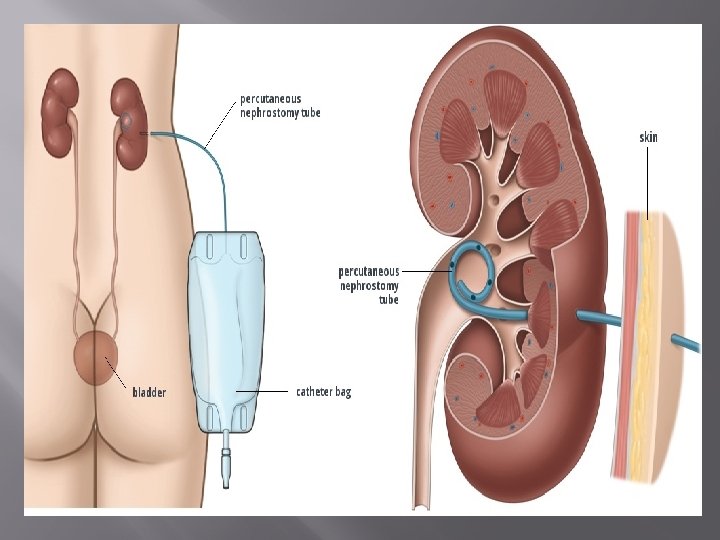
Nephrostomy tube � A catheter that is inserted into the kidney on a temporary basis. It is inserted through a small incision on the flank and terminates in the renal pelvis. Its function is to drain urine into a bag outside the body to preserve renal function when it cannot drain properly.

Indications for a Nephrostomy tube Indications for Nephrostomy: � Removal of renal calculi � Decompression of renal system following obstruction � Trauma distal to kidney causing urine to leak � Complications of renal transplant

Nursing considerations for nephrostomy � Patency � Make sure not kinked, compressed or clamped � Irrigate with NS as ordered (no more than 5 ml) � Pain is symptom tubing is not patent � � � � Assess site for leakage Drain catheter bag as needed I&O Assess characteristics of urine Sterile technique during irrigation, dressing changes, and collecting urine specimen Urine specimens should be collected by gravity, not aspiration Firmly secure catheter and drainage bag

Urine to win it!

Question #1 1. A patient with a ureterolithotomy returns from surgery with a nephrostomy tube in place. Postoperative nursing care of the patient includes A. Encouraging the patient to drink fruit juices and milk. B. Encouraging fluids of at least 2 to 3 L/day after nausea has subsided. C. Irrigating the nephrostomy tube with 10 m. L of normal saline solution as needed. D. Notifying the physician if nephrostomy tube drainage is more than 30 m. L/hr.

Question #2 2. A nurse is planning postoperative care for a client who had kidney transplant surgery. Which of the following should the nurse include in the plan of care? (Select all that apply. ) A. Obtain daily weights B. Assess dressings for bloody drainage C. Replace hourly urine output with IV fluids D. Position in semi-Fowler’s E. Monitor serum electrolytes

Question #3 3. A nurse is teaching diet recommendations to a client who had a kidney transplant and is taking cyclosporine (Neoral). Which of the following recommendations should the nurse include in the teaching? A. Decrease protein rich foods B. Drink grapefruit juice C. Take a magnesium supplement D. Restrict intake of bananas and raisins

Question #4 4. A nurse is providing information to a client who has chronic rejection of a transplanted kidney. Which of the following statements should the nurse include? A. “Immediate removal of the donor kidney is planned. ” B. “Monitoring electrolytes frequently determines kidney status. ” C. “Scheduled kidney biopsies determine kidney status. ” D. “Restarting dialysis depends on marked azotemia. ” E. “Plan to have the immunosuppressive medication increased. ”

Question #5 5. A client who is scheduled for kidney transplantation surgery is assessed by the nurse for risk factors of surgery. Which of the following findings increase the client’s risk of surgery? A. Older than 70 years of age. B. Has a BMI of 41 C. Administers NPH insulin each morning D. Past history of lymphoma E. Blood pressure averages 120/70 mm Hg

Question #6 6. A kidney transplant recipient complains of having fever, chills, and dysuria over the past 2 days. What is the first action that the nurse should take? A. Assess temperature and initiate workup to rule out infection. B. Reassure the patient that this is common after transplantation. C. Provide warm cover for the patient and give 1 g acetaminophen orally. D. Notify the nephrologist that the patient has developed symptoms of acute rejection.

Question#7 7. Which immunosuppressant therapy is most effective? A. Cytotoxic drugs B. Corticosteriod drugs C. Calcineurin drugs D. Monoclonal antibodies

Question #8 8. What complications of kidney transplant is the biggest problem? A. Infection B. Cardiovascular disease C. Rejection D. Malignancies E. Recurrence

Question #9 9. What are the standard immunosuppressive therapy agents used?

Presented and made by: Nicole Berndt, Gloria Tovar, Marcus Solorio, Julia Nelson, Andrew Yambao, and Chelsea Mc. Cown
. Nursing Management of Patients with Nephrostomy")
References � � � A. U. (2012, May). Nursing Management of Patients with Nephrostomy Tubes. Retrieved May 9, 2016, from http: //www. aci. health. nsw. gov. au/__data/assets/pdf_file/0011/165 917/Nephrostomy-Tubes-Toolkit. pdf Lewis, Heikemper, Dirkesen, & Bucher (2014). Medical- Surgical Nursing: Assessment and management of clinical problems (9 th edition) St. Louis: Elsevier/Mosby Sommer, S. , Johnson, J. , Roberts, K. , Redding, S. , Churchill, L. , Elkins, C. , & Roland, P. (2013). RN adult medical surgical nursing (9 th edition). Assessment Technologies Institute, LLC. U. (2016). Indications for Renal Transplant. Retrieved May 9, 2016, from https: //www. med. unc. edu/transplant/patientinfo/Kand. P/indicationscontraindication Hockenberry, (2015) Wong’s Nursing Care of Infants and Children, 10 th edition. Elsevier Inc.
- Slides: 40