Portal hypertension DR Walid Elshazly Portal hypertension Portal





 ®")


 ® It denotes increase resistance in the")
 ® It denotes increase in inflow to")






 ® ® ® Bed rest Diet Albumin infusion Fresh frozen plasma")








 ® Infection ® Bleeding ® Drugs ® Anesthesia ® surgery")
 ® Weakness ® Jaundice ® Fetor hepaticus ® Palmer erytems ®")

 ® Treat precipitating factors ® Diet ® Drugs ® Renal failure")




 <2 2– 3 >3 Albumin")

 Active bleeder ® Resusitation ® Specific measures ® Non-operative ® ® Naso-gastric")
 Huge splenomegally or hyper-splenism Small spleen ® No varices ® Decongestion conserve")
 Active bleeder ® Resusitation ® Specific measures ® Non-operative ® ® Naso-gastric")

 and 2. Crystalloids (Ringer,")


















- Slides: 75
Portal hypertension DR/ Walid Elshazly
Portal hypertension ® Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system ® Normal portal pressure is generally defined between 5 and 10 mm Hg.
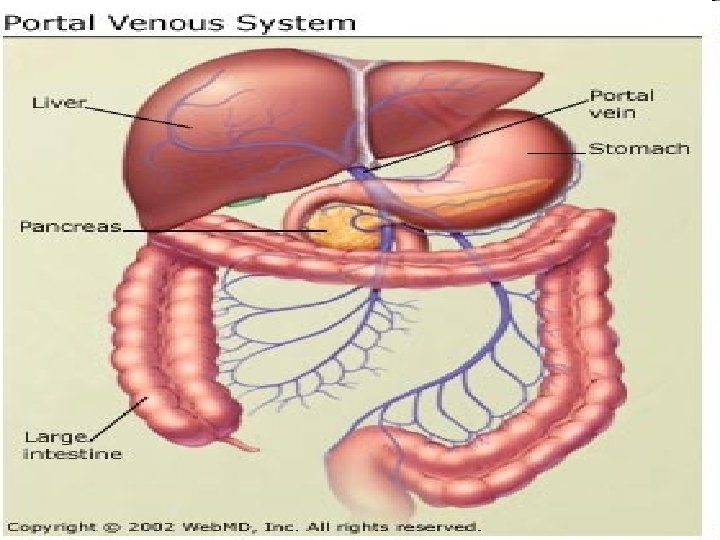
Portal hypertension The portal vein drains blood from the small and large intestines, stomach, spleen, pancreas, and gallbladder.
Portal Vein Anatomy
Portal hypertension The superior mesenteric vein and the splenic vein unite behind the neck of the pancreas to form the portal vein.
Etiology ® Functional ® Organic ® Pre-sinusoidal extra-hepatic ® Pre-sinusoidal intra-hepatic ( Fibrosis) ® Post-sinusoidal intra-hepatic ( Cirrhosis) ® Post-sinusoidal extra-hepatic
Etiology ® Presinusoidal ® Extrahepatic Cavernomatous malformation ® Malignant portal & splenic vein obstruction ® ® Intrahepatic Schistosomiasis ® Congenital hepatic Fibrosis ® Sarcoidosis ®
Etiology ® Post sinusoidal ® Intrahepatic Cirrhosis ® Venoocclusive disease ® ® Extra hepatic Hepatic vein obstruction ® Budd Chiari syndrome ® Constrictive pericadritis ®
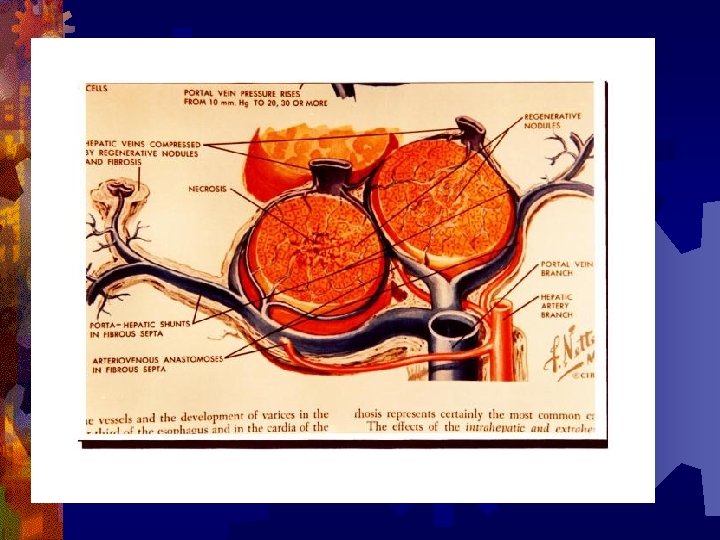
Pathogenesis ® Backward resistance theory (to initiate) ® It denotes increase resistance in the liver bed through a constant component (liver fibrosis and regenerating nodules) ® variable component through the action of humoral substances (endothelin, prostaglandins, adrenergic sububstances, and serotonin) ®
Pathogenesis ® Forward flow theory (to maintain) ® It denotes increase in inflow to the liver through the action of humoral substances that cause hyperdynamic and ® hypervolemic circulation (nitric oxide, glucagon and, prostacylin) ®
Mechanism of portal hypertension In Shistosomiasis ® Peri-portal fibrosis ® Portal hyper-volaemia ® Release of vaso-spastic substances ® Angiomatous mass ® Endo- arterial obstruction
Complication of portal hypertension 1. 2. 3. 4. 5. 6. Spleno-megally GIT congestion Ascites Opening of porto-systemic collaterals Hepatocelluar failure Portosystemic encephalopathy
Splenomegally ® Mechanisms ® RES hyper-plasia ® Opening of A/V shunts ® Venous congestion ® hypersplenism
Splenomegally ® Clinical picture ® Pressure manifestations ® Splenic pain ® Hypersplenism ® Psychic trauma
GIT congestion ®Gastric dyspepsia related to type of food ®Haematemesis dt gastropathy which cause sever form of bleeding
Ascites ® etiology of ascites 1. 2. 3. 4. 5. Hormonal factors lead to salt and water retention Hypo-proteinaemia Portal hypertension Lymphorrhoea Disturbed renal function
Ascites ( treatment) ® ® ® Bed rest Diet Albumin infusion Fresh frozen plasma Diuretics Refractory ascites require 1. 2. 3. 4. Therapeutic para-centesis Recirculation therapy Peritoneo-venous shunt Sapheno-peritoneal shunt
Porto-systemic Collaterals ® Cephalic ® Lower end of esophagus ® Bare area of liver ® Caudal ® Around umbilicus ® Rectal ® Retro-peritoneal
Portal Vein Collaterals Five Principle Routes • Esophageal Varices • Umbilical Vein • Hemorrhoids • Veins of Retzius • Adhesions
1 4 2 3
Lower end of esophagus There is four rather than three plexuses of veins (intraepithelial, superficial, sub mucus and periesophageal) with the intraepithelial plexus in excess
Lower end of esophagus In the palisade zone the veins are oriented in a special way, different from the gastric,
Lower end of esophagus The veins are condensed in the superficial plexus, rather than in the submucosal plexus opposite to the distribution in other zones
Endoscopic Views
Cirrhosis Childs-Pugh Endoscopy No Varices Classification System Varices b-blocker Endoscopy q 2 years 1 st Variceal Bleed Banding Evaluation Medical Tx Banding Parameter 1 Point 2 Points 3 Points Bilirubin <2 2 -3 >3 Albumin >3. 5 2. 8 -3. 5 <2. 8 D PTT 1 -3 4 -6 >6 Ascites None Slight Moderate Encepha- None 1 -2 3 -4 lopathy Rebleeding Childs A or B Childs C / Liver Failure 5– 6 Class A 7– 9 Class B > 10 Class C Surgical Shunt / TIPS Transplant
Hepato-cellular failure ( etiology) ® Infection ® Bleeding ® Drugs ® Anesthesia ® surgery
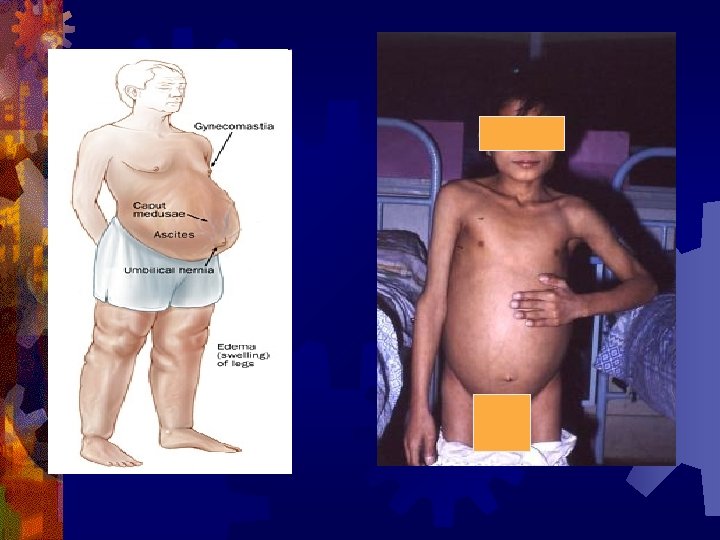
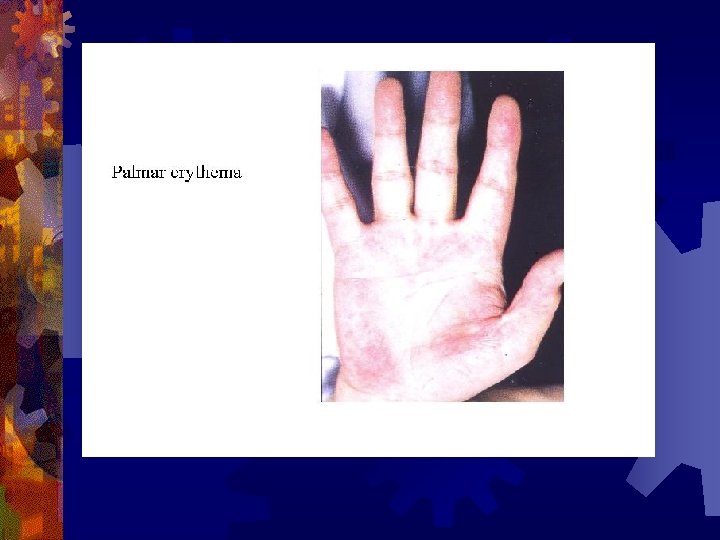
Hepato-cellular failure (C/P) ® Weakness ® Jaundice ® Fetor hepaticus ® Palmer erytems ® Spider angioma ® Gynaecomastia ® Loss of axially and pubic hair ® Testicular atrophy ® Acute liver failure
Gynecomastia
Hepato-cellular failure (R) ® Treat precipitating factors ® Diet ® Drugs ® Renal failure ® Correct clotting abnormalites ® If no response ® Exchange transfusion ® Cross circulation between donor and patient ® Extra-corporeal perfusion through pigs liver
Porto-systemic encephalopathy ® Due to materials that by pass the liver with its toxic effect over the brain (GABA, ammonia, methionine & short chain FA ) ® Clinically Personality changes ® Disorientation ® Slurring speech ® Flappy tremors ® Cogwheel rigidity ® Ankle clonus ® coma ®
Porto-systemic encephalopathy ® Treatment ® Chemical Intestinal antiseptic ® Lactulose ® ® Mechnical ® Liver support ® Nerve cell support glutamic acid
Investigations ® Laboratory ® Stool ® Urine ® CBC ® Kidney function ® Liver function Synthesis (proteins, prothrombin) ® Excretory ( bilirubin, dye excretion) ® Cell insult (SGOT, SGPT, alk phospatase, LDH) ®
Investigations ® Radiological ® U/S ® Doppler ® B swallow ® B enema ® Portography ® CT scan ® MRI ® Radio-isotope ® Instrumental ® Upper endoscopy ® Laparscopic U/S
Child-Pugh Classification Points 1 2 3 Bilirubin (mg/d. L) <2 2– 3 >3 Albumin (g/d. L) > 3. 5 2. 8 – 3. 5 < 2. 8 Prothrombin time (seconds ↑) 1 – 3 4– 6 >6 Ascites None Slight Moderate Encephalopathy None Minimal Advanced Grade A, 5 -6 points; Grade B, 7 -9 points; Grade C, 10 -15 points
Angio-graphy ® Indirect trans-femoral porto-grapgy ® Direct portigraphy ® Per-cutaneous trans-splenic ® Per-cutaneous trans-hepatic ® Umbilical catherization ® Direct operative ® Wedged hepatic venograpgy
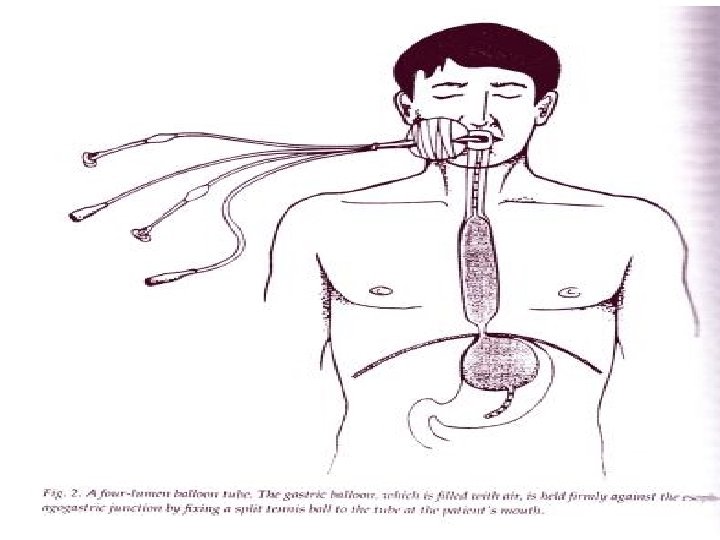
Treatment (Bleeder) Active bleeder ® Resusitation ® Specific measures ® Non-operative ® ® Naso-gastric Tr-iluminal tube Edo-scopic injection Cold case ® Child C injection sclerotherapy ® liver transplantation ® ® Child ® Operative to prevent encephalopathy Non shunt ® ® ® Measures ® ® A&B Hassab Sugura Tanner Shunt ® ® Non selective
Treatment (Non-Bleeder) Huge splenomegally or hyper-splenism Small spleen ® No varices ® Decongestion conserve ® Varices Sclerotherapy ® Decongestion prophylactic ? ? ®
Treatment (Bleeder) Active bleeder ® Resusitation ® Specific measures ® Non-operative ® ® Naso-gastric Tr-iluminal tube Edo-scopic injection Operative ® Measures to prevent encephalopathy
Active bleeder Resusitation On patient admission and after clinical evaluation three lines are installed ® I. V. line for blood sample, blood and fluid replacement ® Urinary catheter for monitoring tissue perfusion together with pulse and BP ® Nasogastric tube or Sangestaken Blackmore tube for monitoring the bleeding, and doing gastric lavage to prepare for endoscopy
Active bleeder Resusitation Resuscitation with transfusion of 1. Colloids (blood) and 2. Crystalloids (Ringer, or lactated Ringer or saline solutions) at the same time with monitoring the blood pressure, pulse and urinary output.
Active bleeder Resusitation Sandostatin infusion (0. 25 microg in 500 ml glucose over 4 to 8 hours, with or without an intramuscularly administered shot) ® Sangestaken tube to arrest the bleeding ® Sclerotherapy ® ® ® can be done immediately, however, it is better to be postponed until the hemodynamics of the patient are corrected and the stomach is washed from the retained blood which obscure the procedure and make it very difficult
Endoscopic Banding
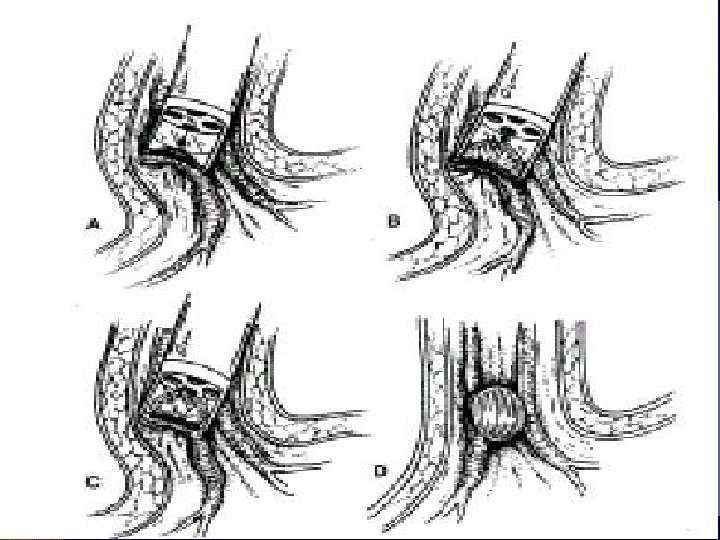
Endoscopic Sclerotherapy Intravariceal Paravariceal
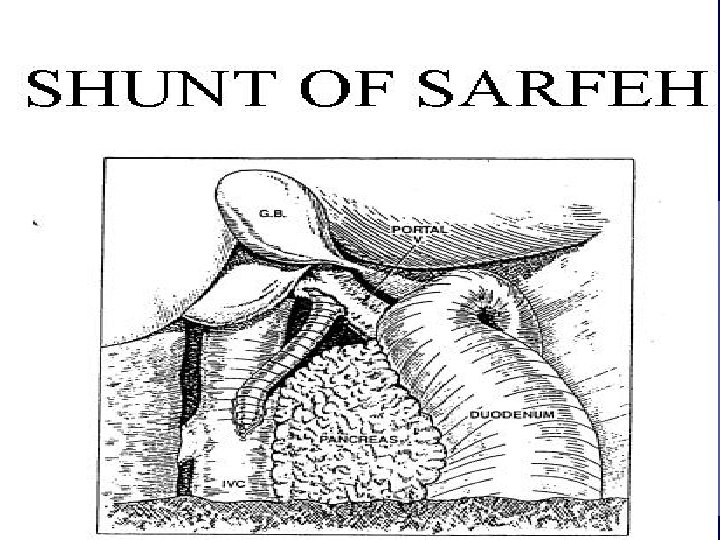
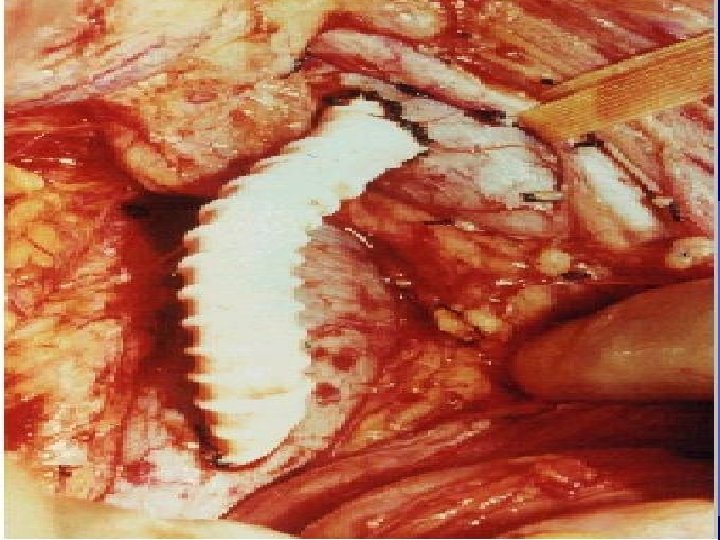
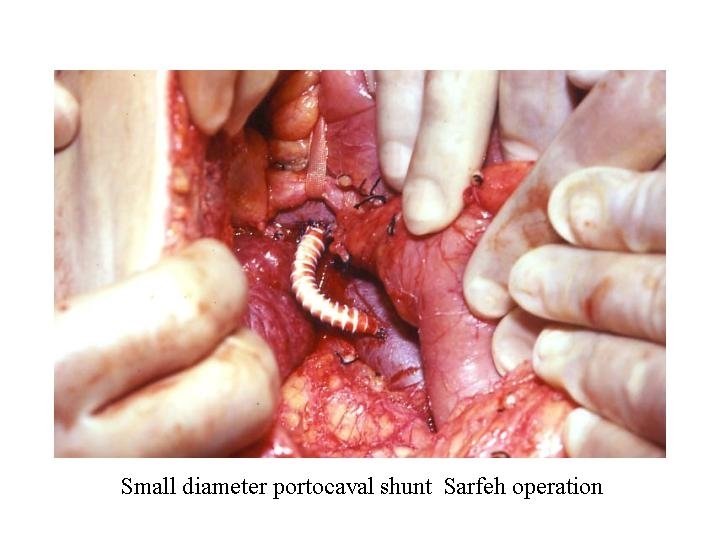
Surgical treatment Non shunt ® Direct ® Varix ligation ® Stappler transsection& reanstmosis ® Indirect ® Hassab ® Tanner ® Sugura Shunt ® Non-selective Porto-caval ® Mesocaval ® proximal- lieno-renal ® ® Selective ® Warren’s ® Modified warrien’s ® Coronary caval ® Sarfeh
Transjugular Intrahepatic PC Shunt
TIPS Transjugular Intrahepatic Portocaval Shunt
TIPS
TIPS
® The spleen is excised ® ® ® decrease the amount of portal blood flow help diaphragmatic excursions, and thus increase chest negativity. It also relieves the mechanical compression of the stomach that can cause dyspepsia. The left gastric is ligated and cut thus causing portoazugus disconnection ® The lower esophagus and the upper stomach are devascularized thus disconnecting the main stream from the esophageal varices area ®
These are devascularisaion operations aiming at portazygus disconnection by interrupting the intrinsic submucosal plexus continuity (Tanner operation)
® The spleen is also excised decreasing portal blood flow ® The esophagus in the thorax as well as in the abdomen is devascularized with the upper half of the stomach (can be done at two stages) ® The left gastric is not cut or ligated and left going up to the chest for azygus connection, only perforators are cut (paraesopahgeal devascularization rather than esophageal devascularization) ® The esophagus or the cardia is transected to interrupt the submucosal blood flow from below to feed the variceal area, in this step the vagus is cut, and pyloromyotomy should be added.
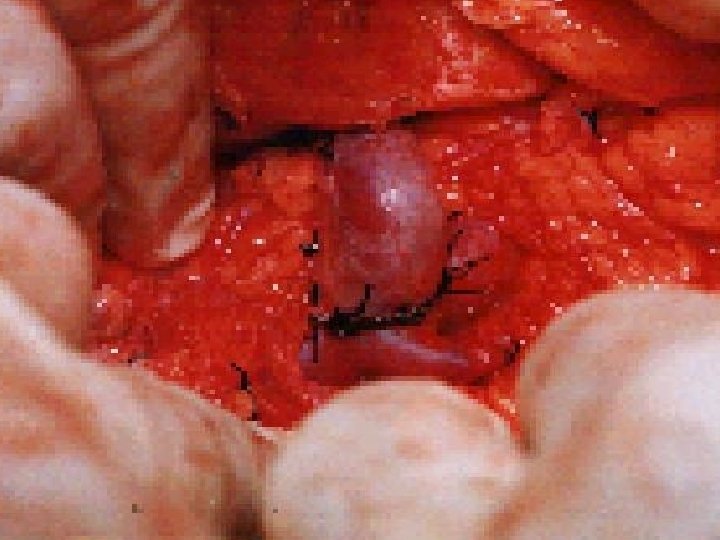
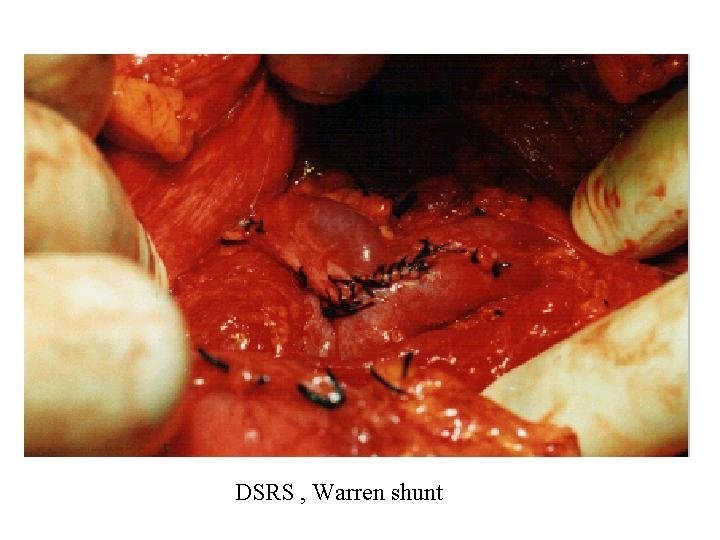
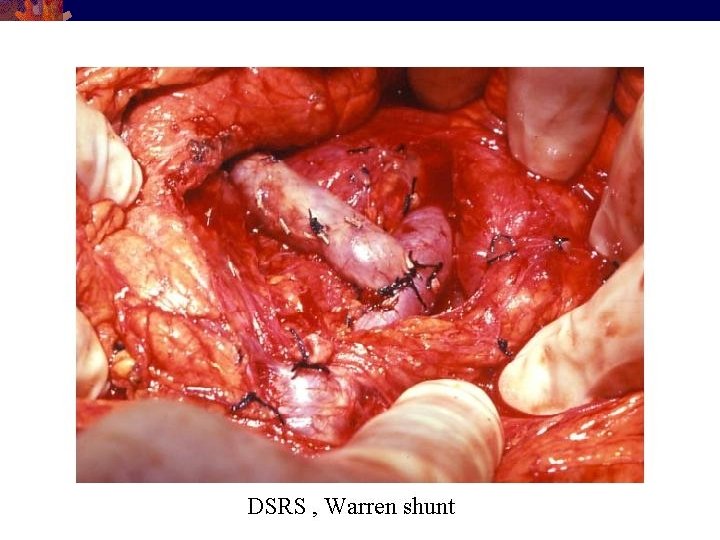
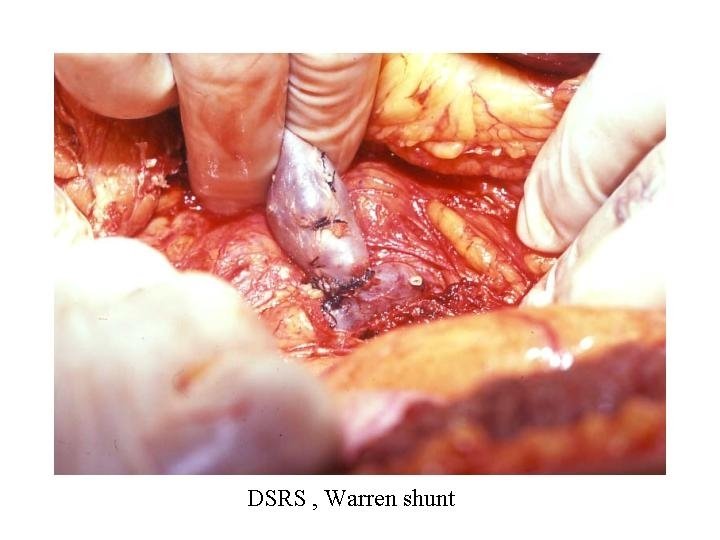
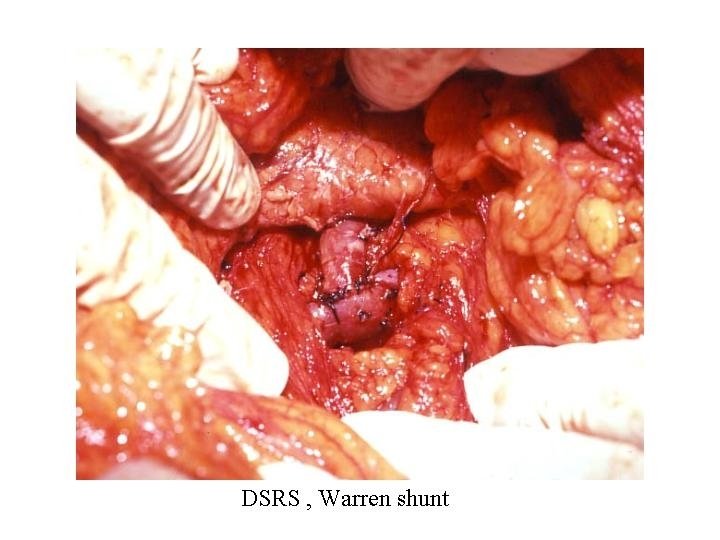
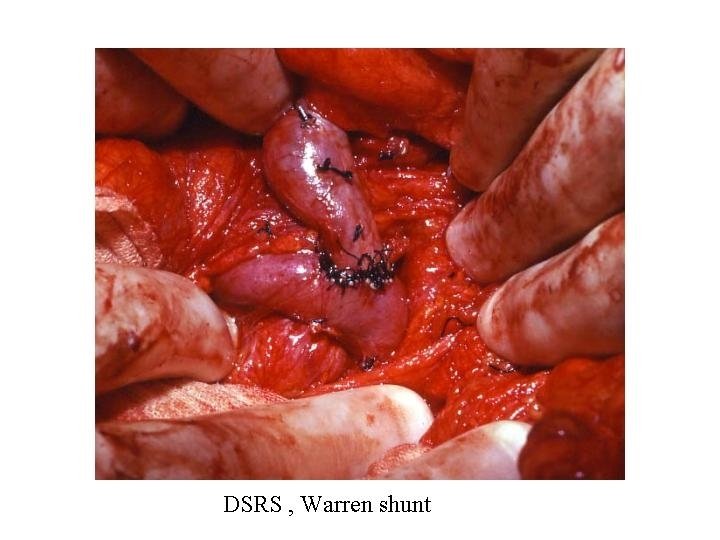
Splenorenal or Warren Shunt Connect the splenic v. to the renal v. Ligate and divide: Coronary v. R-gastroepiploic v. Inf. mesenteric v. Only the splenic, right gastric, and esophageal veins are shunted. Mesenteric flow still goes to the liver
Distal Splenorenal Shunt
Surgical Shunts – Pros and Cons Pros – Long term reduction in portal pressures Reduces ascites Reduces risk of bleeding Cons – Massively invasive procedure Can cause encephalopathy If total shunt, abolishes portal flow Can cause liver failure Patients are no longer candidates for transplant
Total Shunts End to Side Portocaval Interposition Shunts Side to Side Portocaval Central Splenorenal
Total Shunt Results ® Prevent rebleed > 90% ® Thrombosis with graft ® Encephalopathy rate 40%