Physiologic changes of pregnancy Prof Aziza Tosson AIMS






















 output ® Stroke volume")




























































- Slides: 85
Physiologic changes of pregnancy Prof. Aziza Tosson
AIMS ® TO GAIN AN UNDERSTANDING OF THE PHYSIOLOGICAL CHANGES THAT OCCUR DURING PREGNANCY
LEARNING OUTCOMES ® IDENTIFY THE CHANGES THAT TAKE PLACE WITHIN THE UTERUS AND BODY SYSTEMS DURING PREGNANCY ® CONSIDER THE EFFECT THESE CHANGES HAVE ON THE WOMAN ® EXPLORE THE ROLE OF THE MIDWIFE WHEN GIVING ADVISE TO THESE WOMEN
Objectives ® Symptoms and physical findings of each organ system ® Physiologic versus pathologic changes ® Diagnostic tests and interpretations during physiological changes
UNDERSTANDING NEEDED ® TO EXPLAIN THE PHYSIOLOGICAL CHANGES THAT TAKE PLACE TO THE WOMAN ® TO UNDERSTAND THE MINOR DISORDERS OF PREGNANCY ® RECOGNISE PATHOLOGICAL CHANGES IN ORDER TO REFER APPROPRIATELY
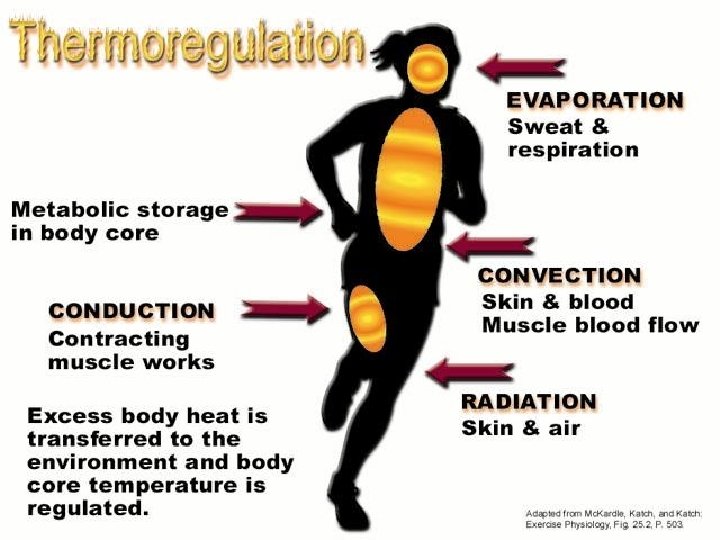
Physiological Changes ® Circulatory ® Urinary ® Thermoregulation ® Skin ® Metabolic ® Breasts ® Respiratory ® Biomechanical ® Digestive
DEFINITION THE CHANGES THAT TAKE PLACE IN THE MATERNAL ORGAN SYSTEM IN RESPONSE TO PREGNANCY. TO ACCOMADATE THE PREGNANCY AND TO PREPARE THE WOMAN FOR LABOUR
Organ systems ® Cardiovascular system ® Pulmonary system ® Genital tract ® Urinary system ® Endocrine system ® Gastrointestinal Tract ® Skin
CHANGES ARE DUE TO ® ALTERATIONS IN ® HORMONAL PRODUCTION ® CIRCULATION ® METABOLISM
HORMONES OESTROGEN ® Produced in corpus luteum ® Produced by placenta after 12 weeks ® Responsible for growth particularly of uterus and breasts
progesterone ® Produced in corpus luteum and then the placenta ® Relaxes smooth muscle ® Inhibits uterine contractions until uterus is prepared for labour ® Regulates storage of body fat
Human chorionic gonadotrophic ® Secreted from trophoblast of the developing embryo ® Maintains corpus luteum until placenta takes over ® Used in tests to confirm pregnancy
Human placental lactogen ® Alters maternal metabolism ® Diverts glucose to fetus ® Mobilises stores free fatty acids from maternal
RELAXIN ® Released by corpus luteum then the Placenta ® Softens pelvic ligaments ® Reduces myometrial tone
Maternal changes - anatomical and physiological ® Cardiovascular changes ® increase in SV ® increase in cardiac output ® increase in HR at given work load ® increase in blood volume (mostly during latter half of pregnancy) ® Uterus may compress large blood vessels reducing venous return ® Total Body water
Circulatory System
Cardiovascular Changes INCREASE ® Blood DECREASE volume ® Cardiac (heart) output ® Stroke volume ® End diastolic volume ® Resting ®% ® Hematocrit ® Blood pressure ® Blood supply to uterus ® Cardiac reserve ® Vascular pulse of blood plasma resistance
Cardiovascular System ® Heart shifts up and to the left ® Hemoglobin stays the same (12 -16 g/d. L) initially ® May drop down to 10 g/d. L and still be normal physiologic anemia. ® Normal pregnancy Hgb is 10 -14 g/d. L later in pregnancy Decreased Hct (38 -47%) ® Normal pregnancy Hct is 32 -42 later in pregnancy Pulse rate may increase 10 -15 beats. Weight of uterus can cause supine hypotensive syndrome. ® ® ® Wajed Hatamleh RN, MSN, Ph. D.
Supine hypotension related to Venal cava syndrome This leads to dizziness, air hunger, nausea
Total body water ® Increases 6 -8 L ® Increases by 40 % ® Normal body water ® 2/3 intracellular ® 1/3 extracellular ¾ interstitial ® ¼ intravasular ® ® 2/3 increase is extravascular
Physiologic anemia of pregnancy ® Physiologic intravascular change ® Plasma volume increases 50 -70 % ® Beginning by the 6 th wk ® RBC mass increases 20 -35 ® Beginning by the 12 th wk ® Disproportionate % increase in plasma volume over RBC volume----Hemodilution ® Despite erythrocyte production there is a physiologic fall in the hemoglobin and hematocrit readings
Iron deficiency anemia ® With erythropoiesis of pregnancy, iron requirements increase. ® Because large amounts of iron may not be available from body stores and may not be in the diet ® Supplementation is recommended to prevent iron deficiency anemia ® At term, Hemoglobin less than 10. 0 is usually due to iron deficiency anemia rather than the hemodilution of pregnancy
Normal Iron Requirements ® Total body iron content average in normal adult females is 2 gm ® Iron requirement for normal pregnancy is 1 gm 200 mg is excreted ® 300 mg is transferred to fetus ® 500 mg is need for mom ® ® ® Daily Total volume of RBC inc is 450 ml 1 ml of RBCs contains 1. 1 mg of iron 450 ml X 1. 1 mg/ml = 500 mg average is 6 -7 mg/day ® Small intervals between pregnancies are most concerning
Respiratory system ® Mechanical ® diaphragm ® Consumption ® Increase in needed oxygen ® Stimulation ® Progesterone stimulation
Physiologic changes ® RESPIRATORY SYSTEM ® increase respiratory rate ® increased oxygen consumption ® common are nasal stuffiness, nosebleeds due to Increased vascular swelling to nose
Respiratory ® Consumption O 2 consumption Increases 15 -20 % ® 50 % of this increase is required by the uterus ® Despite increase in oxygen requirements, with the increase in Cardiac Output and increase in alveolar ventilation oxygen consumption exceeds the requirements. ® Therefore, arteriovenous oxygen difference falls and arterial PCO 2 falls. ®
Physiologic changes ® GASTROINTESTINAL ® Digestive system slow due to progesterone ® Nausea and vomiting ® Ptyalism: increase salivation ® Heartburn ® Hemorrhoids ® Prolonged gallbladder emptying time may lead to gall stones ® Bile salt buildup may lead to itching.
Gastrointestinal Tract ® Displacement of the stomach and intestines ® Appendix can be displaced to reach the right flank ® Gastric emptying and intestinal transit times are delayed secondary to hormonal and mechanical factors ® Pyrosis is common due to the reflux of secretions ® Vascular swelling of the gums ® Hemorrhoids due to elevated pressure in veins
Physiologic changes ® METABOLISM ® BMR increases by 20 -25 % during pregnancy ® Recommended weight gain – 25 -35 lb ® Overweight – 15 -25 lb ® Underweight – 25 -35 lb ® Need for increased iron, calcium, fat, and protein
Metabolic Changes INCREASES IN: ® Insulin level ® Carbohydrate utilization during exercise as weight increases ® Estrogen ® Progesterone ® Relaxin ® Caloric requirements by ~ 300 calories/day ® Protein and fluid requirements
Genital Tract ® Increased vascularity ® Vagina ® Perineum ® Vulva and hyperemia ® Increased secretions ® Characteristic violet color of the vagina ® Chadwick’s sign ® Increased length to the vaginal wall ® Hypertrophy of the papillae of the vaginal mucosa
Physiologic changes in pregnancy - Reproductive system Uterus – ® Enlarges : esp fundal area thickens, then thins later in preg ® Umbilicus by 20 weeks ® Xyphoid by 36 weeks fundus, Braxton. Hicks irregular contractions after 4 months ® Cervix – mucous plug, Goodell’s sign, Chadwick’s sign ® Ovaries –after 11 weeks, the plac prod progesterone and estrogen ®
Changes in the cervix ® Length remains the same ® Increase in width ® Softening after third month due to oestrogen ® Increased vascularity ® Increased cervical mucosa ® Increased glandular function
changes in size uterus grows to 30 x 23 x 20 at term weight increases to 900 gms hypertrophy. . Oestrogen causes cells to increase until 20 weeks gestation Hyperplasia: - number of cells increase under the influence of oestrogen.
After 20 weeks gestation ® Uterine muscle tissue stretches to allow fetus to grow ® Progesterone relaxes the smooth muscles enabling it to stretch
Relative Uterus Size During Pregnancy Figure 28. 15
Changes in the shape of the uterus ® Isthmus elongates during the 1 st 10 weeks like a stalk ® From ® Later 7 mm to 2. 5 cms at 10 weeks becomes the lower segment with the globular uterus sitting on top
® ORGANISATION OF MUSCLE FIBRES ® Inner circular layer ® Surrounds cornua, lower uterine segment and cervix ® Middle layer ® Oblique, crisscross arrangement involved in contractions to expel fetus ® Outer longitudinal layer ® Contracts and retracts thickening the upper segment
BY 12 WEEKS ® Uterus is upright and leans slightly to the right ® No longer a pelvic organ ® Uterus may be palpable above the pubic bone ® Fetus now occupies most of the uterine cavity ® Placenta now developed
ND 2 TRIMESTA ® Development of the upper and lower uterine segment ® Upper segment, thicker containing oblique muscles ® Lower segment formed from the isthmus contains circular and longitudinal muscles ® Uterus is pear shaped again ® Braxton Hicks contractions
rd TRIMESTA 3 ® Lower segment formed from isthmus and contains longitudinal fibres ® Upper segment thick and contains oblique muscle fibres ® By 36 weeks lower segment measures 8 -10 cms ® Engagement ® By 38 weeks the cervix is taken up into the lower segment
BLOOD CHANGES ® Increase in oestrogen: new blood vessels formed growth of existing ones ® Therefore an increase in blood volume.
BLOOD SUPPLY TO UTERUS ® Blood supply pregnancy = 10 mls/min ® At 40 weeks 800 – 900 mls/min ® 20% of cardiac output goes to uterus
® Blood ® Red volume: from 5 litres to 7. 5 total volume up by 40 -50% cell mass: rises constantly throughout pregancy Up by 20% by end of pregnancy
PLASMA VOLUME Increases from 10 th week of pregnancy variable related to parity, fetal weight and number Reaches maximum level approx 50% above non-pregnant levels at 32 -34 weeks then maintained
® 50% rise in plasma volume ® 20% rise in red cell mass ® Heamodilution: Physiological anaemia ® Most apparent at 32 -34 weeks
RENAL SYSTEM ® DILATION OF THE RENAL VESSELS ® DUE THE EFFECTS OF PROGESTERONE ® INCREASED RENAL BLOOD FLOW ® GFR INCREASES BY 60% IN EARLY PREGNANCY ® SIZE OF PORES INCREASED
Urinary Changes ® Kidneys grow and filter more blood as the blood volume increases ® Become more susceptible to bladder and kidney infections ® Bladder becomes compressed causing frequent urination and incontinence
Physiologic changes ®URINARY TRACT ®Increased glomerular filtration rate ®Frequency ®Infection : Smooth muscle of bladder relaxes/stasis Wajed Hatamleh RN, MSN, Ph. D.
Endocrine ® Normal pregnancy physiology ® “lower lows and higher highs” shows ® Postprandial hyperglycemia ® To ensure sustained glucose levels for fetus ® Accelerated starvation ® Early switch from glucose to lipids for fuels ® Insulin resistance promotes hyperglycemia ® Resistance-Reduced peripheral uptake of glucose for a given dose of insulin ® Mild fasting hypoglycemia occurs with elevated FFA, triglycerides, and cholesterol
WATER, WATER Hydration is a major concern during maternal exercise. ® Provide a ready source of water ® Encourage frequent water breaks
Insulin resistance ® Anti-insulin environment is aided by: ® placental lactogen ® Like growth hormone ® Increases lipolysis and FFA ® Increases tissue resistance to insulin ® Increased unbound cortisol ® Estrogen and Progesterone may also exert some anti-insulin effects
Thyroid ® Estrogen stimulates Increase in TBG ® Total T 3 and T 4 are increased ® However the active hormones remains unchanged ® h. CG stimulates thyroid ® TSH is reduced ® Iodine deficient state ® Due to Increased renal clearance ® To rule out pathologic changes ® Early in pregnancy TSH can be used ® Later free T 4 is needed
Liver ® Liver morphology unchanged ® Lab Tests similar to liver disease ® Alkaline phosphatase doubles ® AST, ALT, GGT and bilirubin are slightly lower ® Decreased plasma albumin
Gallbladder ® Impaired contraction ® High residual volumes ® Promotion of stasis ® Stasis associated with increased cholesterol saturation of pregnancy, supports predisposition of stones ® Intrahepatic cholestasis ® Retained bile salts-pruritus gravidarum
Physiologic changes ® INTEGUMENTARY SYSTEM These result from stretching of the skin and hormonal changes ® Linea nigra: pigmentation down middle line of abd ® Chloasma – “mask of pregnancy” ® Straie: stretch marks of abd, breasts, thighs and buttocks ® Sweating Wajed Hatamleh RN, MSN, Ph. D.
Skin changes ® Chloasma or melasma gravidarum ® Striae ® Linea nigra
Skin Changes ® Stretch marks ® Dark pigmented line on there abdomen which is called Linea Nigra ® Pigment changes on their face and neck ® Small blood vessels in the face, neck and upper chest ® MOST OF THESE RESOLVE AFTER PREGNANCY
Melasma
Melasma
Melasma ® Also known as the mask of pregnancy ® More common in dark skin people ® More pronounced in the summer ® Fades a few months after delivery ® Repeated pregnancy can intensify ® Can occur in normal non-pregnant women with harmless hormonal imbalances or women on OCPs or depo
Striae
Striae ® Reddish slightly depressed ® Breasts, thighs, and abdomen ® In future pregnancies they appear as glistening, silver lines
Linea nigra
Hyperpigmentation ® Melasma and linea nigra ® Estrogen and progesterone ® Some melanocyte stimulating effect
Breast Changes | Early in pregnancy, tenderness and tightness is common | After 8 weeks, breasts grow and blood vessels often are visible ® Nipples ®A become larger and darker thick yellowish fluid can be expressed from the nipple
MS system ® Joint relaxation ® Posture changes -lordosis/center of gravity Back ache ® Diastasis recti: separation of rectus abdominous ® Leg cramp due to calcium, and stretching Wajed Hatamleh RN, MSN, Ph. D.
Pelvic Floor Muscle Functions ® Maintain alignment and support of internal organs ® Control of urine flow ® Sexual enhancement ® Eliminate ® Improve waste from rectum recovery from episiotomy
Uterus & Uterine Ligaments Uterus Round ligament Broad ligament
Biomechanical Changes ® Weight ® Joint distribution shifts movement ® Balance ® Spinal of muscle strength curves increase ® Joint laxity becomes greater ® More structural discomfort ® Increased potential for nerve compression
Potential for Injury ® Nerve compression syndromes ® Low back discomforts or pelvic pain ® Upper back fatigue ® Lower extremity ® Pelvic floor function
Postural Dynamics ® Increased ® Top curve of the waist of pelvis tilts forward ® More flexion in the hip joint ® Increased hunching in the upper back and neck ® Tailbone is pushed back
Muscles Affected ® Overstretching & weakening of gluteal muscles & hamstrings ® Overstretching & weakening of abdominal muscles & pelvic floor ® Overstretching & weakening of upper back muscles ® Shortening and tightening of low back & hip flexors muscles ® Shortening of upper back flexors & pectoral muscles
Neurological and sensory ® Decreased intraoccular pressure ® Corneal thickening ® Altered sense of smell ® Decreased attention span ® Problems with memory ® Altered CNS physiology leading to mood disturbance. Wajed Hatamleh RN, MSN, Ph. D.
Combat Effects of Gravity/ Hormones ® Do pelvic tilts ® Do pelvic floor exercises to prevent ® Alter the stance trauma ® Shorten the jog stride ® Emphasize ® Lower or eliminate the strengthening & step in aerobics stretching exercises ® Avoid rapid leg abduction ® Wear abdominal ® Avoid breast stroke kick support/ sports bra in swimming when exercising for ® Recognize tolerance for support activities will vary
Changes to Body System ® First Trimester ® Third Trimester ® ® ® Baby begins to grow Increased urination Changes with skin and hair Thickening waistline Nausea/fatigue Second Trimester ® ® ® Baby’s weight increases Energy level improves Heartburn Leg cramps Pelvis relaxes causing SI discomfort ® ® ® Baby has more rapid growth & weight gain Backaches Swelling of the hands, legs, and feet Breathlessness More frequent urination